2775
2D Flow-Inversion Non-Enhanced (FINE) MRA of lower extremities: comparison with 2D TOF1Institute of Science and Technology for Brain-Inspired Intelligence, Fudan University, Shanghai, Chi, Shanghai, China, 2Radiology, Zhongshan Hospital, Fudan University, Shanghai, China, Shanghai, China, 3United Imaging Healthcare, Shanghai, China, Shanghai, China, 4Central Research Institute, United Imaging Healthcare Group, Shanghai, China, Shanghai, China, 5Institute of Science and Technology for Brain-Inspired Intelligence, Fudan University, Shanghai, China, Shanghai, China
Synopsis
Keywords: Vessels, Blood vessels
Motivation: Inflow-based NCE MRA techniques have limited capability of background and venous suppression at the high field strength.
Goal(s): This study described a new arterial spin labeling (ASL)-based method for lower limb MR angiography (MRA) called FINE (Flow-Inversion Non-Enhanced).
Approach: The performance of FINE was evaluated on ten healthy volunteers and compared with 2D TOF MRA on 3T.
Results: 2D FINE technique provides superior suppression of background and venous signal with reduced acquisition time than that of 2D TOF.
Impact: The results of this study demonstrate the feasibility of FINE MRA of the lower limbs at 3T.
Introduction
Peripheral NCE MRA has received considerable attention during the last few decades due to its no-invasiveness and safety in patients with impaired renal function. Inflow-based NCE MRA like 2D TOF, Quiescent-interval single-shot (QISS) and Inflow Inversion Recovery (IFIR) have a common drawback of insufficient background suppression, especially when B1 inhomogeneity is severe at the high field strength1-3. By performing image subtraction between unlabeled and labeled images, arterial spin labeling (ASL)-based techniques show distinct advantages in background suppression. Previous ASL-MRA studies mainly focus on the upper body such as renal,neck and head4-6, but the feasibility of using ASL-MRA in the lower limb remains unexplored. This study introduces an optimized variation of ASL-MRA, termed Flow-Inversion Non-Enhanced (FINE), provided by United Imaging. Its performance is compared to 2D TOF at 3T.Method
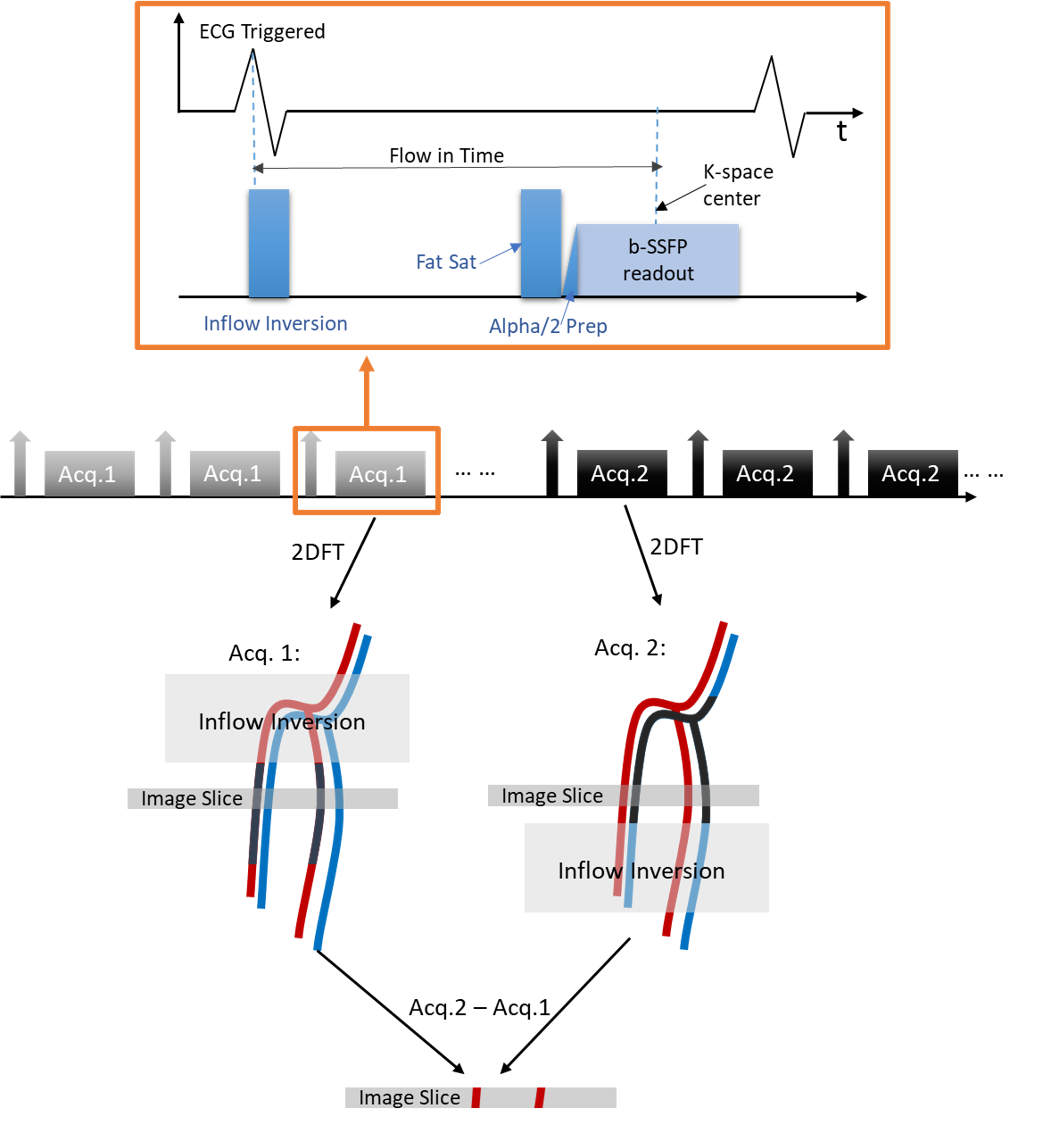
FINE MRAThe sequence diagram of FINE MRA is illustrated in Figure 1. The sequence of events can be summarized as follows:
- The R wave triggers the application of the tracking inversion RF pulse to tag a large volume of inflow blood from the artery;
- After a user-defined flow-in time, a CHESS fat saturation pulse is applied followed by a 2D single-shot b-SSFP readout to acquire the data in the axial orientation during the diastole period;
- After Acq. 1, the same process is repeated for Acq.2, except that the inversion RF pulse in Acq.2 is placed below the image slice to tag the flowing blood from the vein and also create magnetic transfer effects equivalent to Acq.1.
- Angiogram is obtained by subtracting Acq.1 from Acq.2.
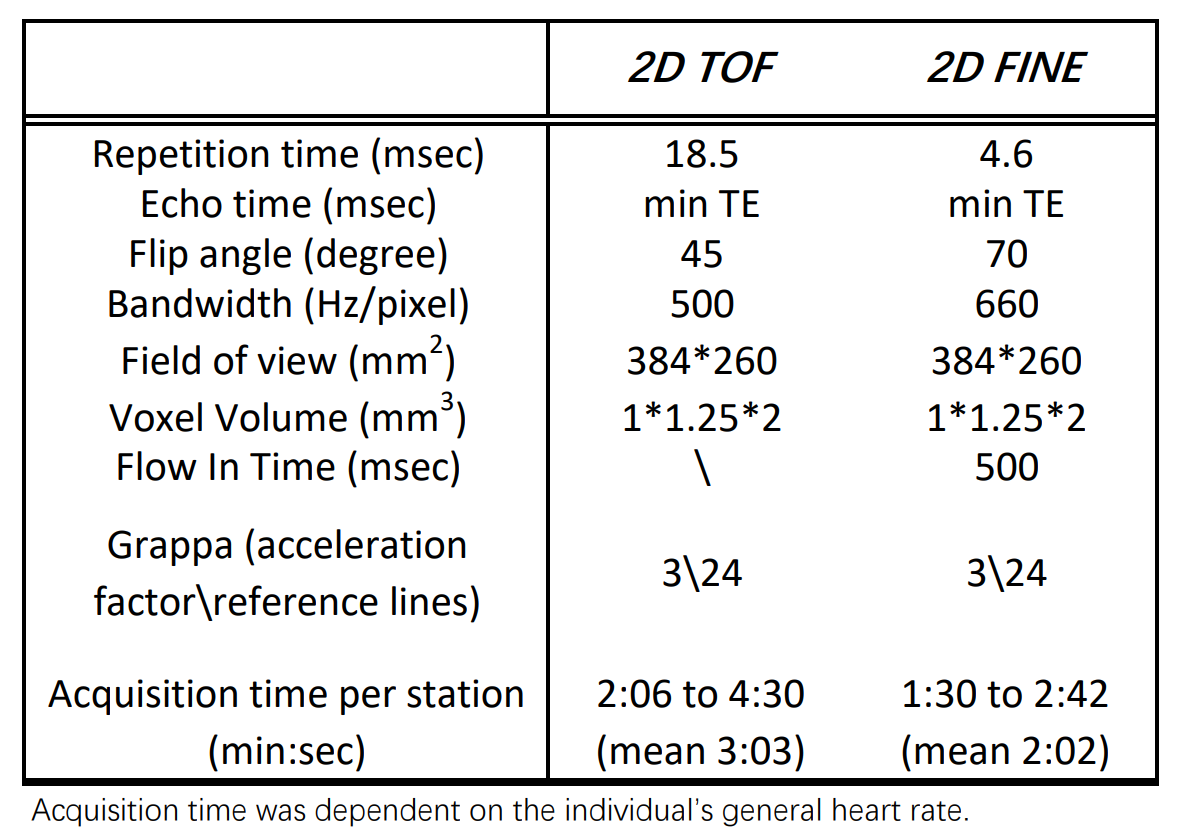
2D FINE and TOF MRA of lower extremities were performed on ten healthy volunteers (6 men, and 4 women; mean age 41±8 years) using a 3 T whole-body MRI system (uMR 790, United Imaging Healthcare). The spatial resolution was kept consistent between FINE and TOF (summarized in Table 1). 70 transversal slices were acquired per station with 10% overlap between each station. Six volunteers required 6 stations to obtain a complete angiogram while the other four volunteers required 7 stations.
Image Analysis
Quantitative evaluation was performed between 2D FINE and TOF in this study. The arterial tree was classified into 16 segments for evaluation. Vessel-to-background ratio: $$VBR = Signal_{Vessel}/Signal_{Tissue}$$ and vessel contrast-to-background ratio: $$VCBR = ({Signal_{Vessel}-Signal_{Tissue}})/({Signal_{Vessel}+Signal_{Tissue}})$$ were calculated for each vessel segment. A pairwise one-sided t-test was performed to check for statistically significant differences between different methods.
Results
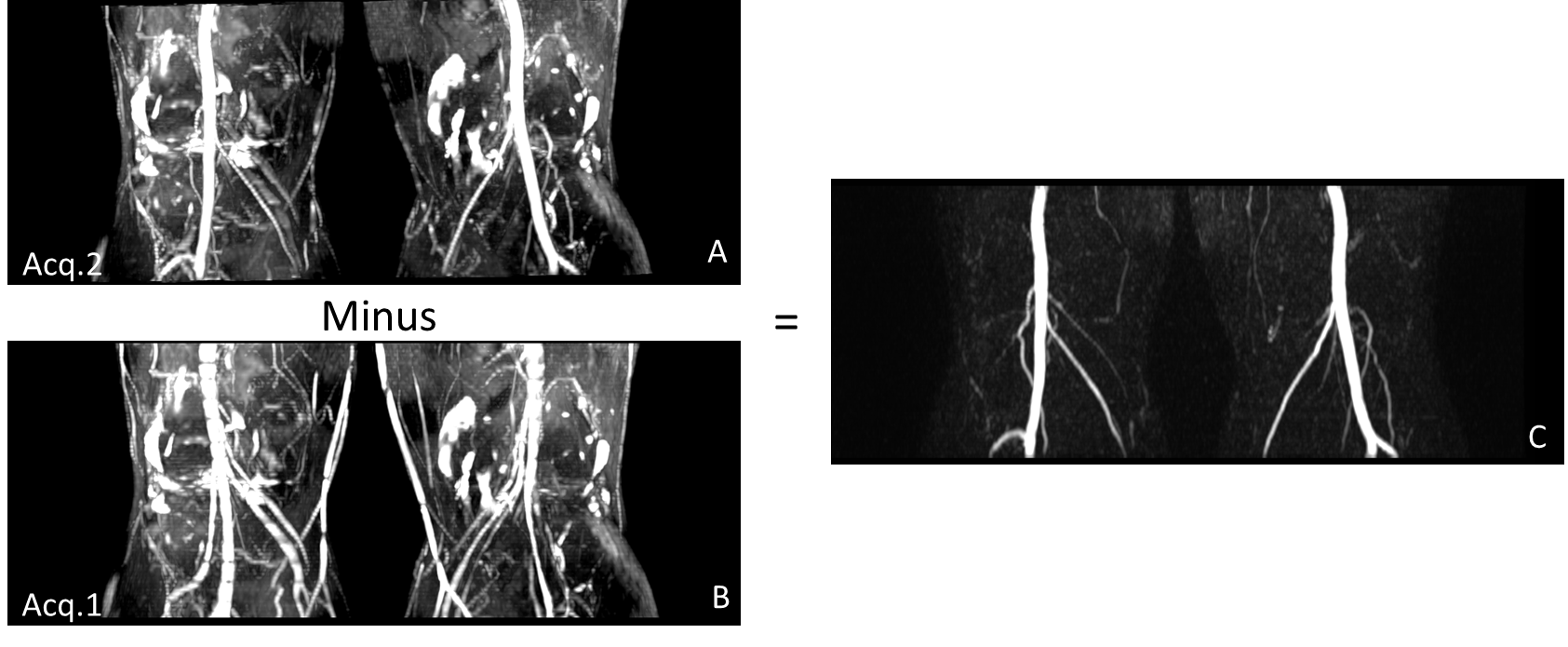
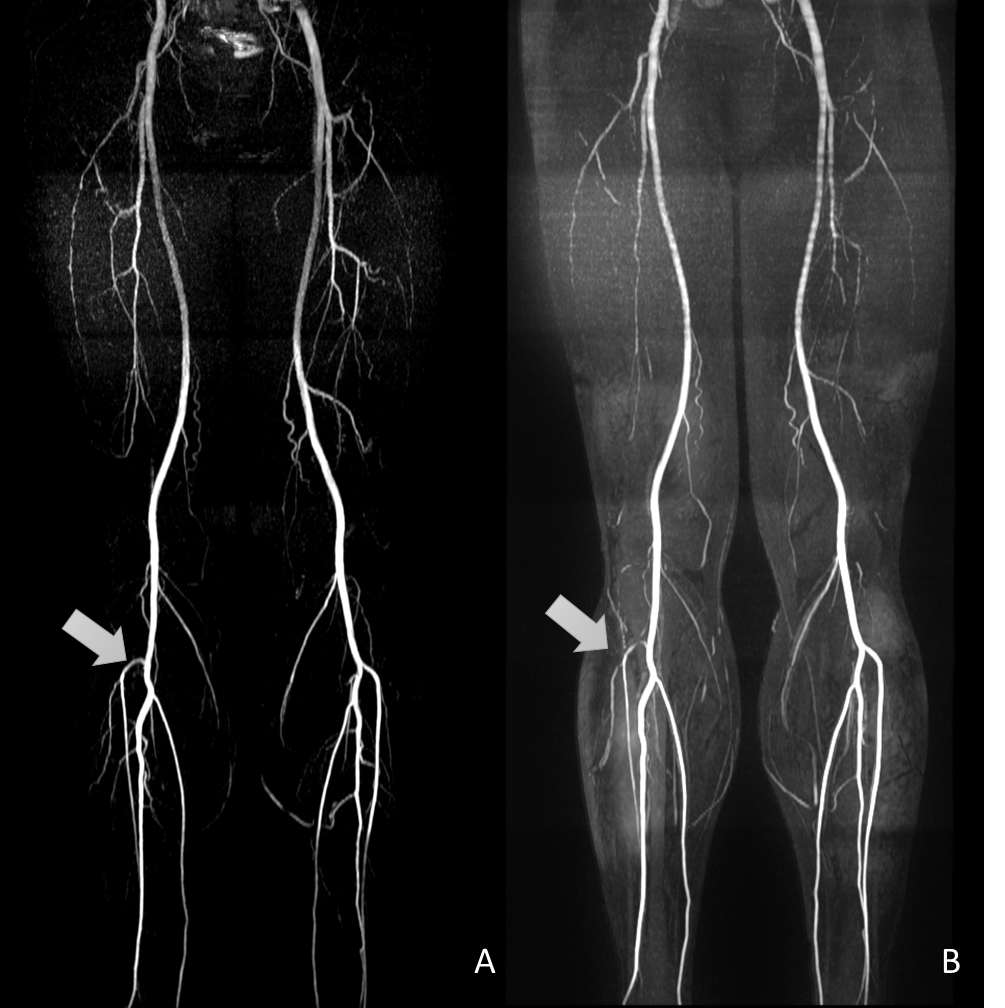
Figure 2 shows the acquisition workflow of FINE technique using one image station as an example, the final angiogram is obtained by subtracting bright-vein image (Acq.1) from bright-artery image (Acq.2). Figure 3 compares maximum intensity projections (MIPs) of all acquired stations for one volunteer of 2D FINE (Figure 3A) and 2D TOF (Figure 3B). 2D FINE MRA achieved better background and venous suppression as well as improved visualization of branch details than that of 2D TOF. As shown in Table 2, there is also statistically significance that the VBRs and VCBRs of 2D FINE (32.10± 3.76 and 0.92± 0.01) is higher than that of 2D TOF (11.53±2.00 and 0.81± 0.03) (datas are means ± SDs; P<.001).Discussion and Conclusion
This study presents a new ASL-based technique for lower limb MRA, which shows advantages over 2D TOF in terms of acquisition time and background suppression. Compared to 2D TOF, the average acquisition time of 2D FINE was reduced from 3:03 min to 2:02 min per station. Benefiting from the image subtraction scheme, 2D FINE achieved a background signal level close to zero, which is indicated by the significant increase in VBR and VCBR. Improved visualization of small arteries can also be observed but needed further evaluation in future studies.The current FINE method has a potential limitation due to its sensitivity to motion caused by image subtraction of two datasets. Future studies will develop image registration method to reduce misregistration artefacts and explore the potential of applying in pelvis and abdomen. In addition, the sensitivity to B1 and B0 field inhomogeneity may affect image quality in certain regions, as seen by the obscurity of arteries and increased level of noise in the femoral station. RF pulse design and shimming method could play an important role in obtaining sharp and uniform delineation of arteries in large anatomy size.
In conclusion, 2D FINE is a promising method for lower limb NCE-MRA at 3 T. It offers improved background suppression and reduced acquisition time compared to 2D TOF.
Acknowledgements
No acknowledgement found.References
1. Edelman RR, Sheehan JJ, Dunkle E, Schindler N, Carr J, Koktzoglou I. Quiescent‐interval single‐shot unenhanced magnetic resonance angiography of peripheral vascular disease: technical considerations and clinical feasibility. Magnetic Resonance in Medicine: An Official Journal of the International Society for Magnetic Resonance in Medicine. 2010;63(4):951-8.
2. Johst S, Orzada S, Fischer A, Schäfer LC, Nassenstein K, Umutlu L, et al. Sequence comparison for non-enhanced MRA of the lower extremity arteries at 7 Tesla. PloS one. 2014;9(1):e86274.
3. Metzger GJ, Auerbach EJ, Akgun C, Simonson J, Bi X, Uğurbil K, et al. Dynamically applied B1+ shimming solutions for non‐contrast enhanced renal angiography at 7.0 Tesla. Magnetic resonance in medicine. 2013;69(1):114-26.
4. Edelman RR, Siewert B, Adamis M, Gaa J, Laub G, Wielopolski P. Signal targeting with alternating radiofrequency (STAR) sequences: application to MR angiography. Magnetic resonance in medicine. 1994;31(2):233-8.
5. Yan L, Wang S, Zhuo Y, Wolf RL, Stiefel MF, An J, et al. Unenhanced dynamic MR angiography: high spatial and temporal resolution by using true FISP–based spin tagging with alternating radiofrequency. Radiology. 2010;256(1):270-9.
6. Miyazaki M, Isoda H. Non-contrast-enhanced MR angiography of the abdomen. European journal of radiology. 2011;80(1):9-23.
Figures