2771
Ultra-low-field Neck Time-of-flight MRA at 0.05 Tesla: A Preliminary Study1Laboratory of Biomedical Imaging and Signal Processing, The University of Hong Kong, Hong Kong SAR, China, 2Department of Electrical and Electronic Engineering, The University of Hong Kong, Hong Kong SAR, China
Synopsis
Keywords: Vessels, Low-Field MRI, Magnetic Resonance Angiography
Motivation: The recent resurgence of ultra-low-field MRI (i.e., below 0.1 T) is showing great promise for future clinical applications due to its low cost, portability, and accessibility, potentially advancing neck MRA for evaluating and diagnosing carotid diseases in point-of-care scenarios and low/mid-income countries.
Goal(s): To explore the neck MRA using TOF technique at 0.05 Tesla.
Approach: Flow-compensated 2D GRE sequences with and without flow saturation for multi-slice neck scans.
Results: Carotid arteries/bifurcations and jugular veins can be visualized with strong vessel-to-background contrast. We envision that usable and quality neck MRA can be potentially achieved at ULF with further sequence and/or post-processing optimization.
Impact: Ultra-low-field (ULF) neck MRA can potentially advance the evaluation of carotid stenosis and occlusion, as well as the diagnosis of stroke and aneurysms, in point-of-care scenarios and low/mid-income countries.
Introduction
Magnetic resonance angiography (MRA), including the inflow time-of-flight (TOF) technique1,2, has proven to be valuable in the evaluation of carotid stenosis and occlusion, as well as the diagnosis of stroke and aneurysms3-5. The recent resurgence of ultra-low-field (ULF) MRI (i.e., below 0.1 T) is showing great promise for future clinical applications due to its low cost, portability, and accessibility6-14. ULF MRI holds the possibility to advance neck MRA for the evaluation and diagnosis of carotid diseases in point-of-care scenarios and low/mid-income countries. In this study, we explore the feasibility of neck MRA using the TOF technique on a low-cost and shielding-free 0.05 Tesla MRI scanner.Method
In vivo experimentsAll in vivo experiments were conducted on a permanent magnet based 0.05 Tesla MRI scanner using neck coil for signal receiving. The scanner had a similar design to that reported in our previous work6, which was free from any magnetic and RF shielding. Healthy subjects were enrolled in this study under institutional review board approval. Written informed consents were obtained.
Multi-slice 2D GRE sequences with and without flow saturation were implemented to visualize neck vessels. Sequence parameters were: FA = 90°, TR/TE = 38/10ms, BW = 5kHz, 75% partial echo in readout (RO) direction and 80% undersampling in phase encoding (PE) direction, acquisition resolution = 2×2×4mm3, matrix size = 80×86×34, NEX = 4, and total acquisition time = 7.4mins. To reduce the signal loss due to flowing blood spin dephasing, first-order flow compensation was applied in all three directions.
For carotid artery and jugular vein imaging, a selective flow saturation pulse followed by spoiler gradients in all three directions was applied before each excitation pulse, to saturate the signal of downstream venous blood and upstream artery blood, respectively.
Image reconstruction and processing
K-space data were first processed for electromagnetic interference (EMI) signal removal by utilizing active EMI sensing and deep learning EMI signal prediction and cancellation6,15, without any EMI characterization data acquisition. Then partial Fourier reconstruction was applied in both RO and PE directions. Afterward, 4× in-plane and 8× through-plane zero-padding was conducted before image reconstruction and maximum intensity projection (MIP).
Results
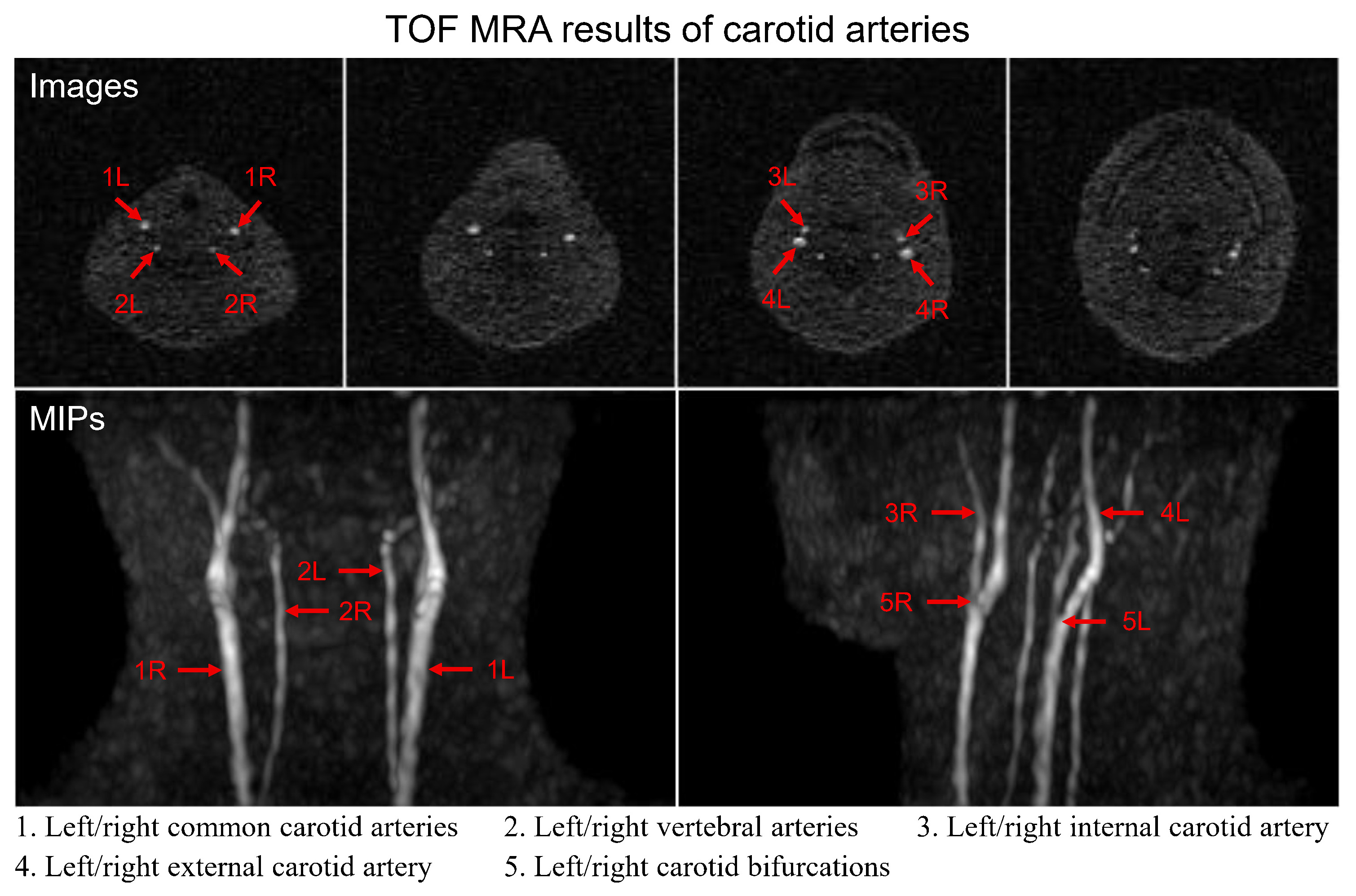
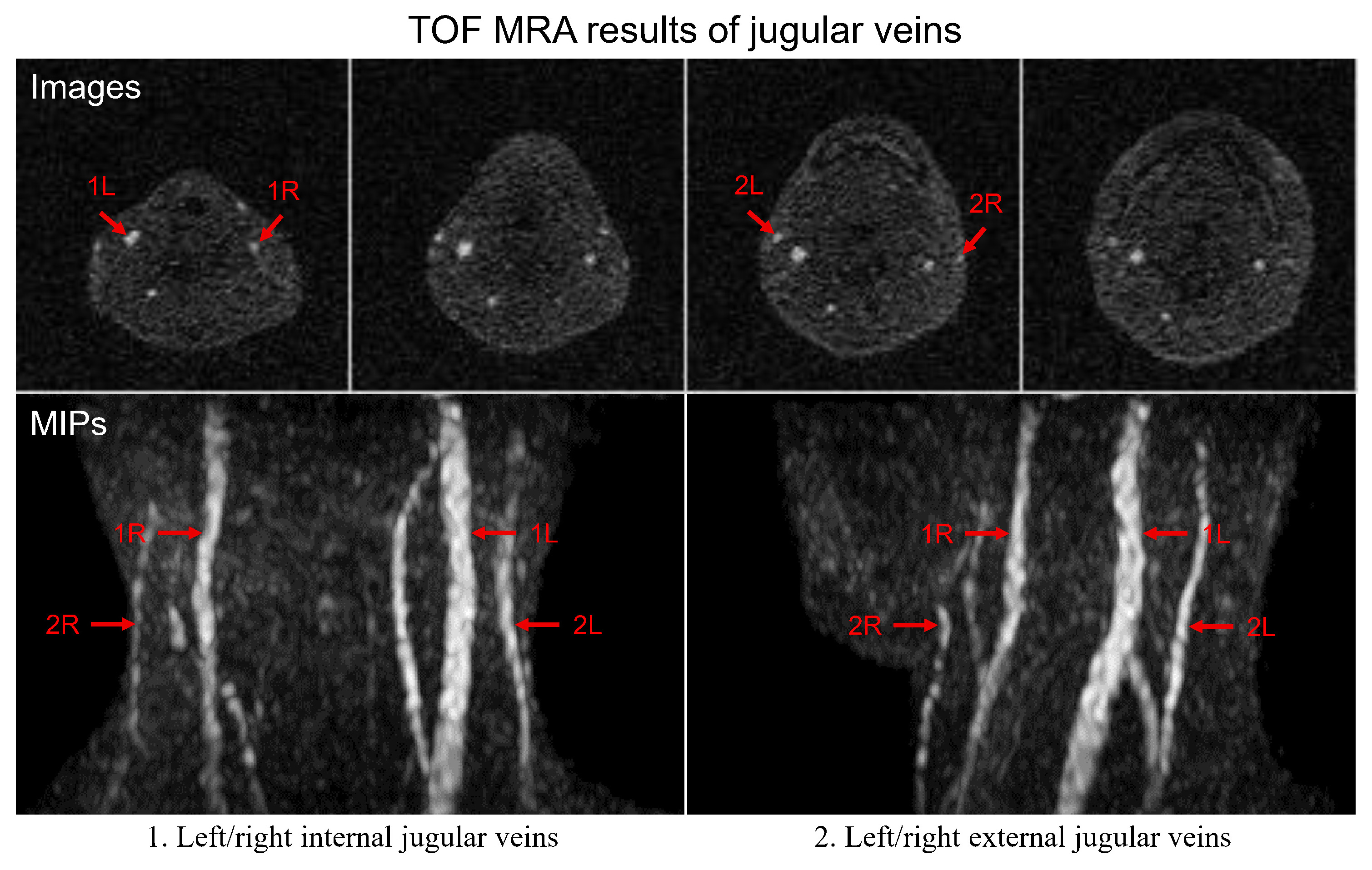
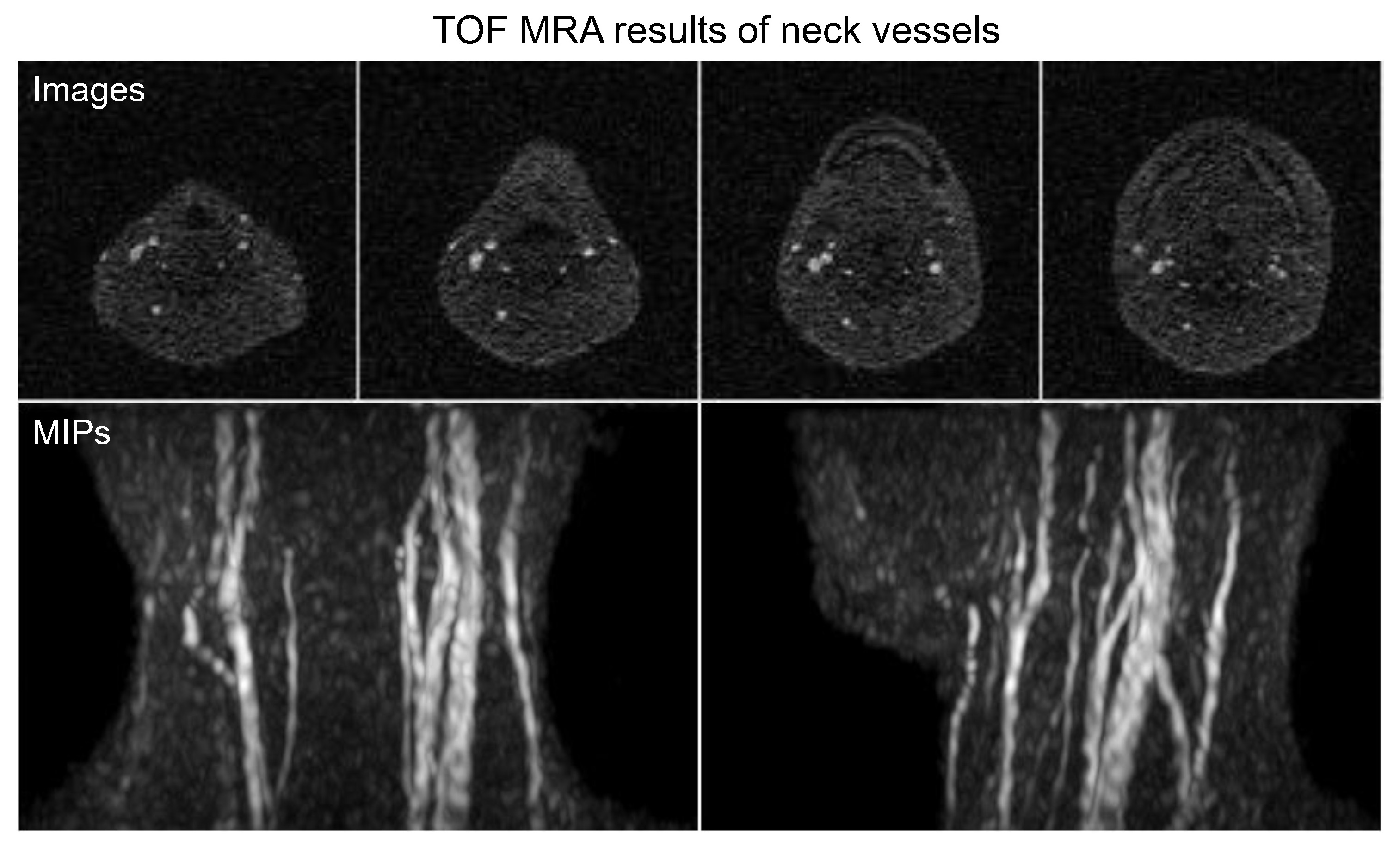
Multi-slice 2D TOF MRA achieved strong vessel-to-background contrast. In general, 2D GRE with a large FA of 90° and short TR effectively suppressed the background signal and enhanced the vessels through a strong inflow effect. Note that the same slices and MIP rotation angles were selected and shown in the following figures. As shown in Fig. 1, without venous contamination, the left and right common carotid arteries, vertebral arteries, internal carotid arteries, and external carotid arteries (Fig. 1, red arrows) could be readily identified and visualized in both the raw 2D images and MIPs. Moreover, the left and right carotid bifurcations were clearly visible in the MIPs (Fig. 1, red arrows). Note that the arteries were not smooth or incomplete in some regions. Fig. 2 shows the jugular veins results obtained with carotid artery saturation. The jugular veins, including the left and right internal and external jugular veins (Fig. 2, red arrows), could be observed. The observed signal intensity differences between the left and right jugular veins might be attributed to different in-plane saturation of the slow flowing venous blood. Fig. 3 shows the neck vessel results obtained without flow saturation. The morphology of carotid arteries and jugular veins is consistent with those in Figs. 1 and 2, demonstrating the robustness of neck MRA in different scans at ULF.Discussion and Conclusions
Neck MRA is a key protocol for the assessment of carotid diseases3-5. In this preliminary study, we demonstrate the possibility of non-contrast enhanced neck MRA at ULF for the first time. Both carotid arteries and jugular veins could be visualized at 0.05 Tesla. The preliminary results clearly indicated the potential of ULF MRI for neck MRA despite the low SNR.To improve neck TOF MRA quality at ULF, several steps can be taken in future development: (i) sequence optimizations of slice overlapping and thinner slice thickness to reduce the non-smooth vessel visualization16; (ii) utilization of large power flow saturation pulses or extra strong magnetization transfer preparation to suppress stationary muscle tissues, especially given the extremely low RF SAR at ULF; (iii) use of compressed sensing acquisition and reconstruction to reduce scan time, increase the spatial resolution, or/and suppress noise; and (iv) use of intravascular blood pool contrast agent to shorten blood T1, then use 3D acquisition to increase SNR or/and spatial resolution. These strategies may also advance the potential use of ULF MRI for abdominal and peripheral vessel imaging in the future.
Acknowledgements
This work was supported in part by Hong Kong Research Grant Council (R7003-19F, HKU17112120, HKU17127121, HKU17127022 and HKU17127523 to E.X.W).References
[1] Alfidi RJ, Masaryk TJ, Haacke EM, Lenz GW, Ross JS, Modic MT, Nelson AD, LiPuma JP, Cohen AM. MR angiography of peripheral, carotid, and coronary arteries. AJR Am J Roentgenol 1987;149(6):1097-1109.[2] Laub GA. Time-of-flight method of MR angiography. Magn Reson Imaging Clin N Am 1995;3(3):391-398.
[3] Wagle WA, Dumoulin CL, Souza SP, Cline HE. 3DFT MR angiography of carotid and basilar arteries. American journal of neuroradiology 1989;10(5):911-919.
[4] Keller PJ, Drayer BP, Fram EK, Williams KD, Dumoulin C, Souza SP. MR angiography with two-dimensional acquisition and three-dimensional display. Work in progress. Radiology 1989;173(2):527-532.
[5] Heiserman JE, Drayer B, Fram E, Keller P, Bird C, Hodak J, Flom R. Carotid artery stenosis: clinical efficacy of two-dimensional time-of-flight MR angiography. Radiology 1992;182(3):761-768.
[6] Liu Y, Leong AT, Zhao Y, Xiao L, Mak HK, Tsang ACO, Lau GK, Leung GK, Wu EX. A low-cost and shielding-free ultra-low-field brain MRI scanner. Nature communications 2021;12(1):7238.
[7] Yuen MM, Prabhat AM, Mazurek MH, Chavva IR, Crawford A, Cahn BA, Beekman R, Kim JA, Gobeske KT, Petersen NH, Falcone GJ, Gilmore EJ, Hwang DY, Jasne AS, Amin H, Sharma R, Matouk C, Ward A, Schindler J, Sansing L, Havenon AD, Aydin A, Wira C, Sze G, Rosen MS, Kimberly WT, Sheth KN. Portable, low-field magnetic resonance imaging enables highly accessible and dynamic bedside evaluation of ischemic stroke. Science advances 2022;8(16):eabm3952.
[8] He Y, He W, Tan L, Chen F, Meng F, Feng H, Xu Z. Use of 2.1 MHz MRI scanner for brain imaging and its preliminary results in stroke. Journal of Magnetic Resonance 2020;319:106829.
[9] O’Reilly T, Teeuwisse WM, de Gans D, Koolstra K, Webb AG. In vivo 3D brain and extremity MRI at 50 mT using a permanent magnet Halbach array. Magnetic resonance in medicine 2021;85(1):495-505.
[10] Mazurek MH, Cahn BA, Yuen MM, Prabhat AM, Chavva IR, Shah JT, Crawford AL, Welch EB, Rothberg J, Sacolick L, Poole M, Wira C, Matouk CC, Ward A, Timario N, Leasure A, Beekman R, Peng TJ, Witsch J, Antonios JP, Falcone GJ, Gobeske KT, Peterson N, Schindler J, Sansing L, Gilmore EJ, Hwang DY, Kim JA, Malhotra A, Sze G, Rosen MS, Kimberly WT, Sheth KN. Portable, bedside, low-field magnetic resonance imaging for evaluation of intracerebral hemorrhage. Nature communications 2021;12(1):5119.
[11] Sheth KN, Mazurek MH, Yuen MM, Cahn BA, Shah JT, Ward A, Kim JA, Gilmore EJ, Falcone GJ, Petersen N, Gobeske KT, Kaddoub F, Hwang DY, Schindler J, Sansing L, Matouk C, Rothberg J, Sze G, Siner J, Rosen MS, Spudich S, Kimberly WT. Assessment of brain injury using portable, low-field magnetic resonance imaging at the bedside of critically ill patients. JAMA neurology 2021;78(1):41-47.
[12] Cooley CZ, McDaniel PC, Stockmann JP, Srinivas SA, Cauley SF, Śliwiak M, Sappo CR, Vaughn CF, Guerin B, Rosen MS. A portable scanner for magnetic resonance imaging of the brain. Nature biomedical engineering 2021;5(3):229-239.
[13] Lau V, Xiao L, Zhao Y, Su S, Ding Y, Man C, Wang X, Tsang A, Cao P, Lau GK, Leung GK, Leong ATL, Wu EX. Pushing the limits of low‐cost ultralow‐field MRI by dual‐acquisition deep learning 3D superresolution. Magnetic resonance in medicine 2023.
[14] Man C, Lau V, Su S, Zhao Y, Xiao L, Ding Y, Leung GK, Leong AT, Wu EX. Deep learning enabled fast 3D brain MRI at 0.055 tesla. Science advances 2023;9(38):eadi9327.
[15] Zhao Y, Xiao L, Liu Y, Leong AT, Wu EX. Electromagnetic Interference (EMI) Elimination via Active Sensing and Deep Learning Prediction for RF Shielding‐free MRI. NMR in Biomedicine 2023:e4956.
[16] Kaufman JA, McCarter D, Geller SC, Waltman AC. Two-dimensional time-of-flight MR angiography of the lower extremities: artifacts and pitfalls. AJR American journal of roentgenology 1998;171(1):129-135.
Figures