2768
Variability in measurements of abdominal blood flow using non-invasive phase-contrast-mapping MRI1Department of Clinical Physiology and Nuclear Medicine, Department of Clinical Physiology and Nuclear Medicine, Rigshospitalet, Copenhagen University Hospital, Denmark, Glostrup, Copenhagen, Denmark, 2Department of Biomedical Sciences, Faculty of Health and Medical Sciences, University of Copenhagen, Copenhagen, Denmark, Copenhagen, Denmark, 3Department of Clinical Physiology and Nuclear Medicine, Bispebjerg and Frederiksberg Hospital, University Hospital of Copenhagen, Copenhagen, Denmark, Copenhagen, Denmark, 4Department of Clinical Physiology and Nuclear Medicine, Department of Clinical Physiology and Nuclear Medicine, Rigshospitalet, Copenhagen University Hospital, Denmark, Copenhagen, Denmark
Synopsis
Keywords: Digestive, Digestive, PC-MRI, Intestine
Motivation: Measuring the reproducibility of 2D PC-MRI measures of intestinal blood flow is important for its clinical application.
Goal(s): The aim is to examine the precision of 2D PC-MR measures of resting intestinal blood flow and postprandial blood flow changes.
Approach: Ten healthy men were scanned on eight different days collecting at least three repeated 2D PC-MRI measures each day. Participants were also given an oral glucose tolerance test.
Results: A CoV of 6%-9% was obtained for consecutive flow measures and 13%-15% for between day measurements. Flow increased 75% in the arteria mesenterica superior and 60% in the vena portae after glucose consumption.
Impact: The low variability of repeated flow measures in the arteria mesenterica superior and vena portae compared to the high change in flow after glucose consumption makes 2D PC-MRI measures of flow changes in these vessels a feasible diagnostic test.
Methods: This prospective study included ten healthy men who were scanned on eight different days collecting at least three repeated 2D PC-MRI measures in an imaging plane intersecting the arteria mesenterica superior (AMS) and truncus coeliacus interceded with three repeated measures in a plane intersecting the arteria hepatica and the vena portae. On two of the days, nine additional repeated scans were acquired after the participants were given an oral glucose tolerance test (75 grams of glucose in 250 ml water) or 250 ml water, respectively.All MRI-scans were performed on a 3 Tesla Siemens Biograph mMR PET-MRI scanner using a surface body coil combined with coils integrated into the table. The sequence used was a 2D gradient echo sequence with retrospective cardiac triggering (1 slice, Field of view (FOV) = 240x340 mm2, voxel size = 0.71x0.71x5 mm3, repetition time (TR)= 11.0 ms, echo time (TE)= 3.17 ms, flip angle = 15o, 25 samples per cardiac cycle, GRAPPA acceleration factor = 2). For measurements of blood flows in AMS and truncus coeliacus a velocity encoding factor (VENC) of 200 cm/s was used and for flow in arteria hepatica and vena portae a VENC of 100 cm/s. Region of interests (ROI) delineating the vessels were manually drawn by two separate observers using in-house developed software ((https://github.com/MarkVestergaard/PCMCalculator/). The blood flow was then calculated as mean blood velocity times the cross-sectional areal of the delineated vessel.
Results: Mean blood flow values and reproducibility results in coefficients of variations (CoV) for variance between observers, day to day variance, and variance in repeated measures are presented in Figure 1. All vessels demonstrated low CoV (6%-9%) for within sessions repeated consecutive measures which was fair for between day measurements (13-15%) with the exception of large variance in arteria hepatica flow (30%). Consumption of glucose induced an average peak flow increase of 75% (+/-45) in the AMS and 60% (+/- 30%) flow increase in the vena portae, but no significant change in the arteria hepatica or truncus coeliacus (Figure 2). Individual flow measures for the prolonged postprandial and placebo skanning days are presented in Figure 3.
Conclusions: The low variability of repeated flow measures in the AMS and vena portae compared to the high change in flow after glucose consumption makes flow changes in these vessels feasible as a future diagnostic test to identify CMI patients among patients with a high clinical suspicion of CMI.
Acknowledgements
No acknowledgement found.References
1. Terlouw LG, van Dijk LJD, van Noord D, et al. MRI-based pre- and postprandial flow in the mesenteric vasculature of patients with suspected chronic mesenteric ischemia. Eur J Radiol. 2022;151:110316.
2. Terlouw LG, Verbeten M, van Noord D, et al. The Incidence of Chronic Mesenteric Ischemia in the Well-Defined Region of a Dutch Mesenteric Ischemia Expert Center. Clin Transl Gastroenterol. 2020;11:e00200.
3. van Dijk LJD, Moons LMG, van Noord D, et al. Persistent symptom relief after revascularization in patients with single-artery chronic mesenteric ischemia. J Vasc Surg. 2018;68:779–785.
Figures
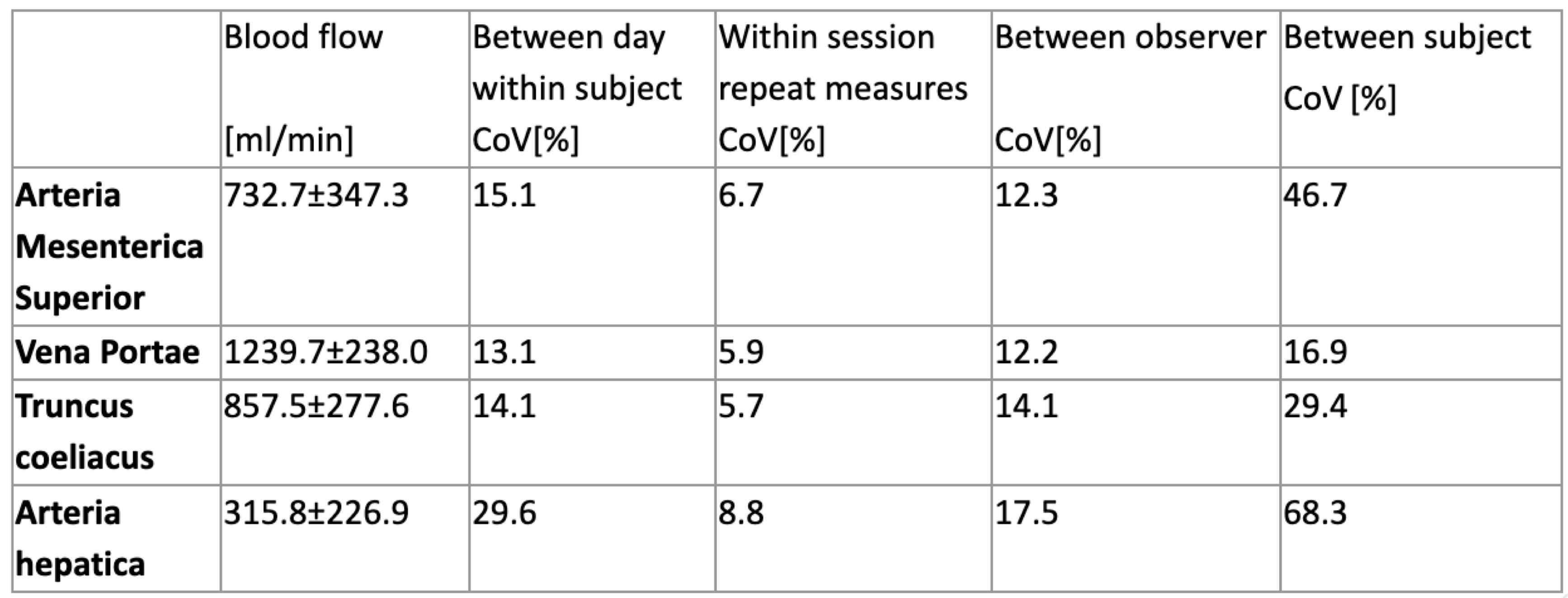
Figure 1. Variation in flow measures
Variation between days and repeated measures are based on eight visits on separate days where three flow measures were acquired each day and analysed twice by different observers. With the exception of between observer variation, flow measures for CoV calculations were based on the average measure from the two observers.
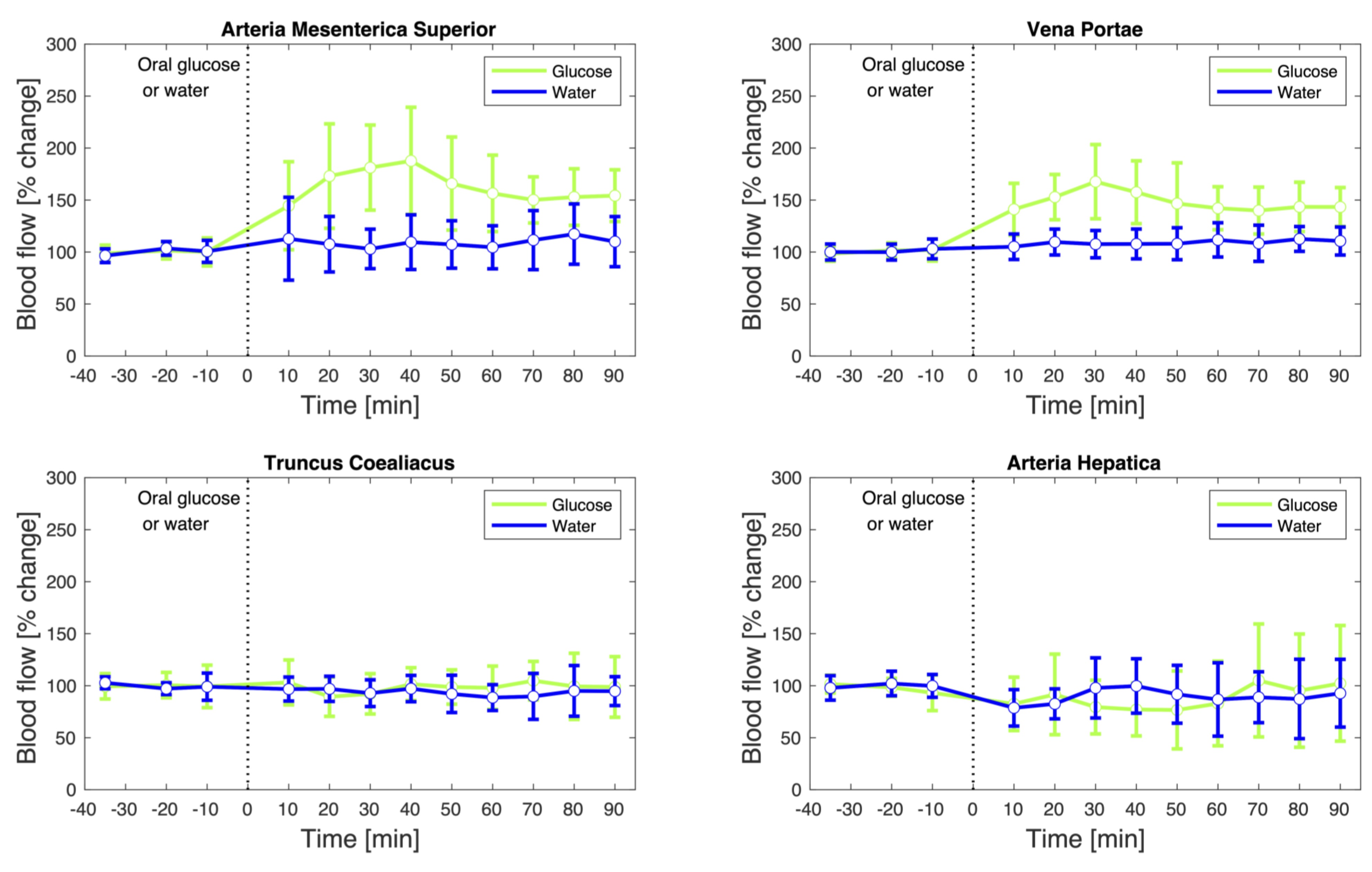
Figure 2. Flow response to oral glucose vs. placebo
On two of the examination days, subjects were given a drink after baseline flow measures and scanning continued. Flow measures (mean +/- SD) for the four vessels are shown. Flow in AMS and vena portae were significantly higher after a glucose rich drink compared to plain water.
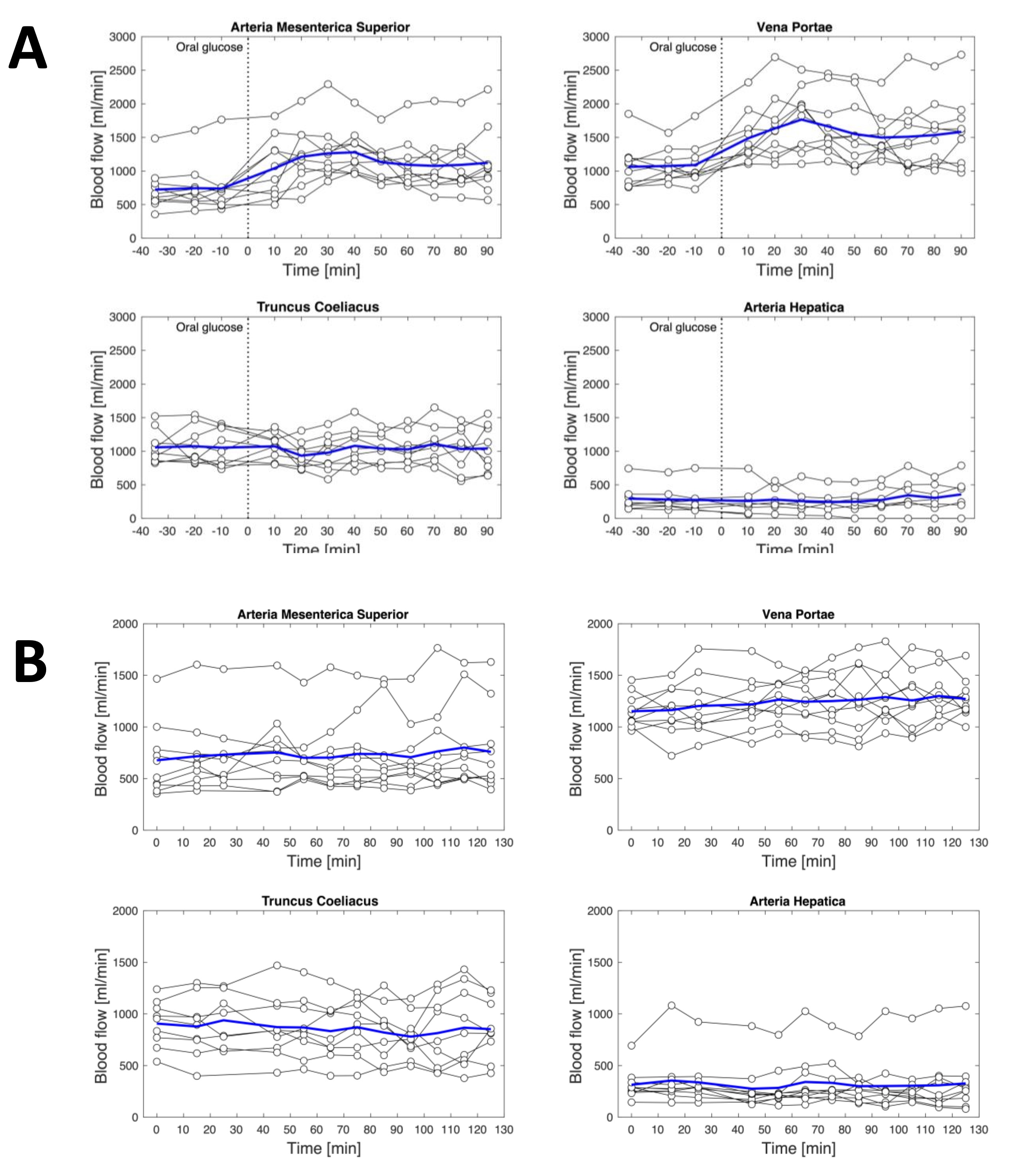
Figure 3. Flow measures for individual subjects after oral glucose and placebo
All measure points for all ten subjects are shown for the days when subjects were given a glucose rich drink (A) or water as a placebo (B) after baseline flow measures. Flow measures for the four vessels are shown for all ten subjects.