2761
Non-contrast assessment of pulmonary perfusion using pulsed arterial spin labeling on a 0.55T scanner1National Institutes of Health, Bethesda, MD, United States
Synopsis
Keywords: Lung, Lung, Mid-field
Motivation: Pulmonary perfusion imaging requires ionizing radiation (CT) or gadolinium-based contrast agents (MR) and therefore cannot be used on all patients.
Goal(s): We propose an easy-to-prescribe non-contrast pulmonary perfusion imaging method to improve the diagnosis and monitoring of pulmonary hypertension.
Approach: We designed a free-breathing arterial spin labeling imaging sequence that is compatible with whole-lung coverage at 0.55T. We demonstrate this method in healthy volunteers and a swine model.
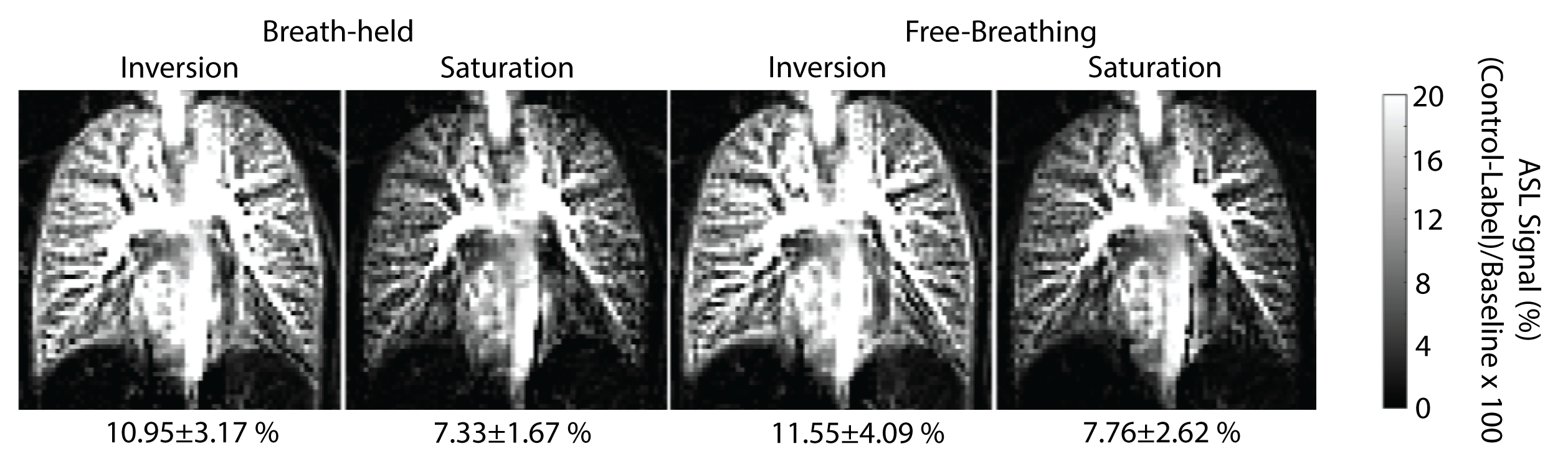
Results: We measured 11.55±4.09% and 7.76±2.62% ASL signals using inversion and saturation labeling which was comparable between breath-held and free-breathing scans. Perfusion defects were clearly visualized in the swine model.
Impact: Our method should enable qualitative assessment of non-contrast pulmonary perfusion in patients who are contraindicated for gadolinium-based contrasts or who need frequent monitoring of pulmonary perfusion. Our method would contribute to enabling contrast-free comprehensive pulmonary exams at 0.55T.
Background
Mid-field (0.55T) MRI systems have the potential to improve the accessibility of high-quality structural and functional lung imaging (1). Pulmonary perfusion imaging is an important biomarker that can be clinically used for the diagnosis and monitoring of pulmonary hypertension, specifically chronic thromboembolic pulmonary hypertension (CTEPH). CTEPH can lead to right heart failure, if left untreated, but early diagnosis of CTEPH is challenging because it is diagnosed using SPECT or CT imaging, both of which use ionizing radiation. Recently, gadolinium-based MRI lung perfusion methods have been proposed for imaging pulmonary embolism and CTEPH (2). However, there are potential risks associated with gadolinium-based contrast, and contrast perfusion is harder to “add-on” to clinical protocols. We believe that non-contrast pulmonary perfusion imaging on 0.55T systems can improve early screening and monitoring of CTEPH (2). Existing non-contrast pulmonary perfusion methods are either single slice or require careful planning of complex geometries for labeling making complete lung coverage challenging (3). In this work, we present a non-contrast free-breathing pulmonary perfusion imaging method that’s relatively easy to use and compatible with whole-lung coverage. We also demonstrate the method in healthy-volunteers and a large animal model of perfusion defect.Methods
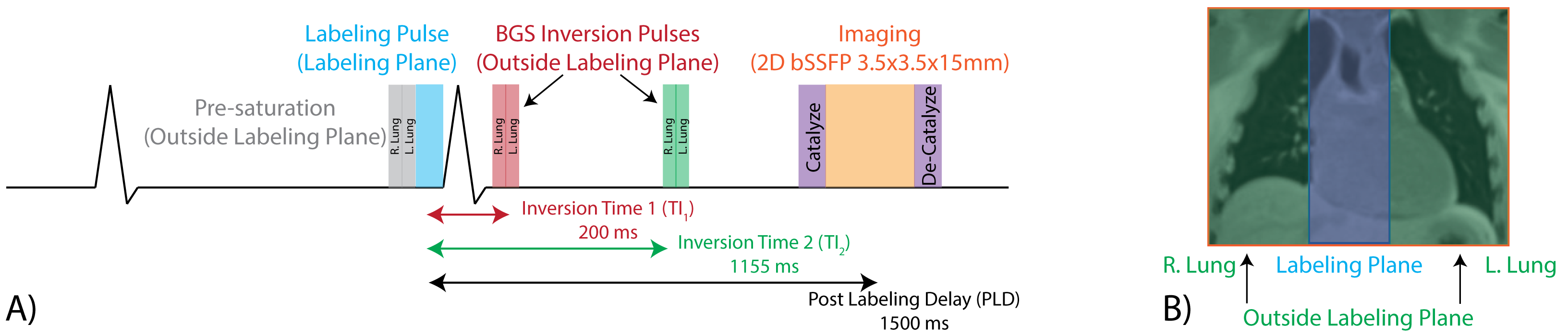
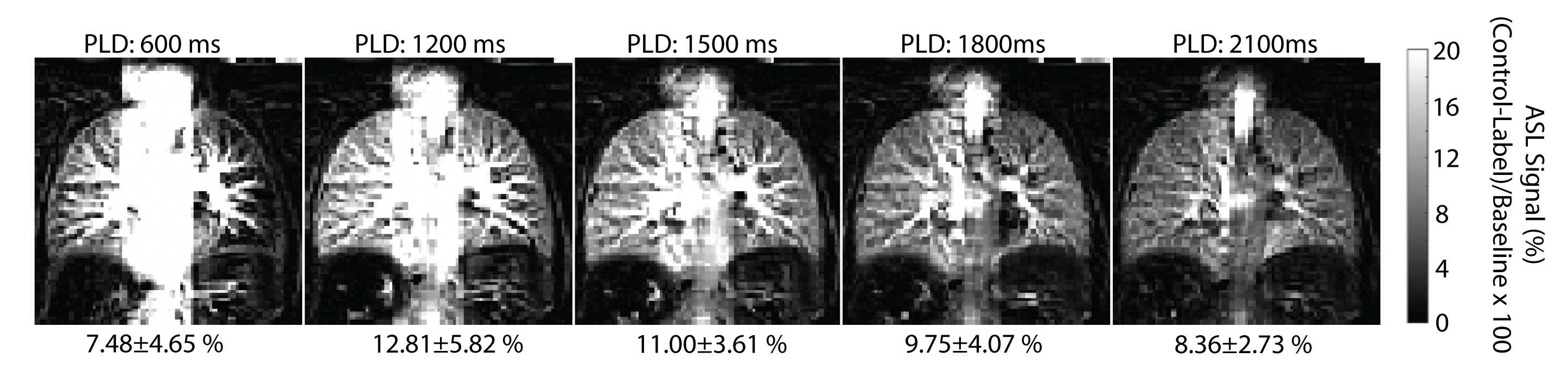
We scanned 7 healthy volunteers and one pig at 0.55T scanner (prototype MAGNETOM Aera, Siemens Healthcare, Germany). Perfusion was measured with a cardiac-gated background-suppressed pulsed arterial spin labeling sequence (Figure 1), using a transfer-insensitive-labeling (TILT) technique for labeling the blood (4). All the blood going to the lungs was labeled with a labeling pulse using a sagittal 67.5 mm labeling slab placed over the right atrium. This labeling scheme is compatible with multi-slice imaging for complete lung coverage and is easy to prescribe using coronal and axial views.To optimize for the labeling-scheme, data were acquired with post-labeling delays (PLD) of 600 - 2100ms using an inversion-labeling pulse in 3 HVs, to choose the optimal PLD. Then, inversion and saturation labeling were compared, with a PLD of 1500ms in 4 HVs, to measure differences in ASL signal and its stability within and across healthy volunteers. Finally, a breath-held (BH) and free-breathing (FB) acquisition was compared using the measured ASL signal. In 1 of the volunteers, we acquired five slices sequentially using the FB scan to illustrate compatibility with whole lung coverage.
Six and twelve pairs of control and label images were acquired for BH and FB imaging, respectively. Each breath-hold was 3-seconds and a minimum of 6-second wait between subsequent images was used to allow for magnetization recovery. All images were registered using a B-Spline diffeomorphic registration from the ANTs registration toolbox before calculating the ASL signal (5).
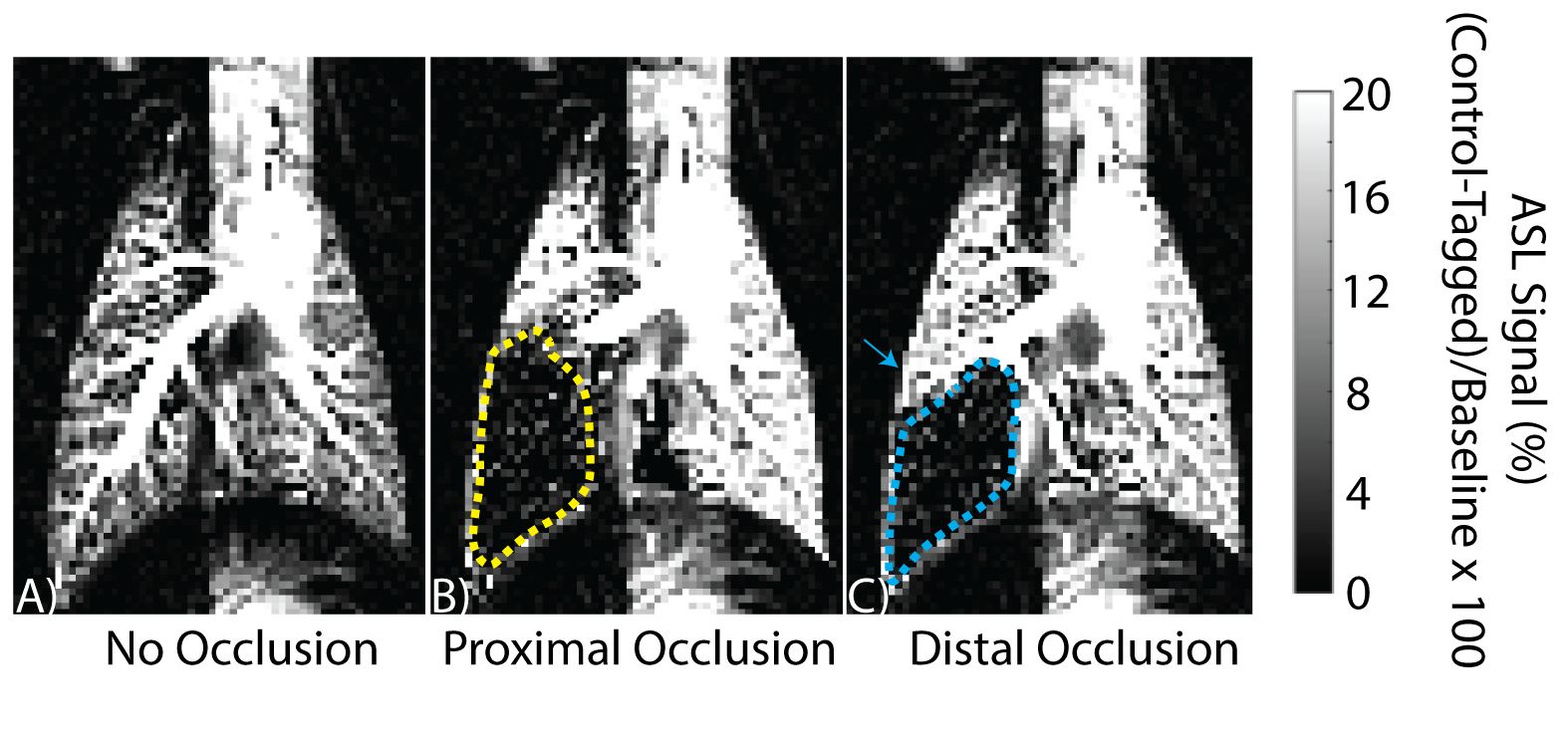
To validate the ability of our technique to detect severe defects, a pig model of pulmonary perfusion defect was made by complete occlusion of the right pulmonary artery at a proximal location and a distal location.
Results
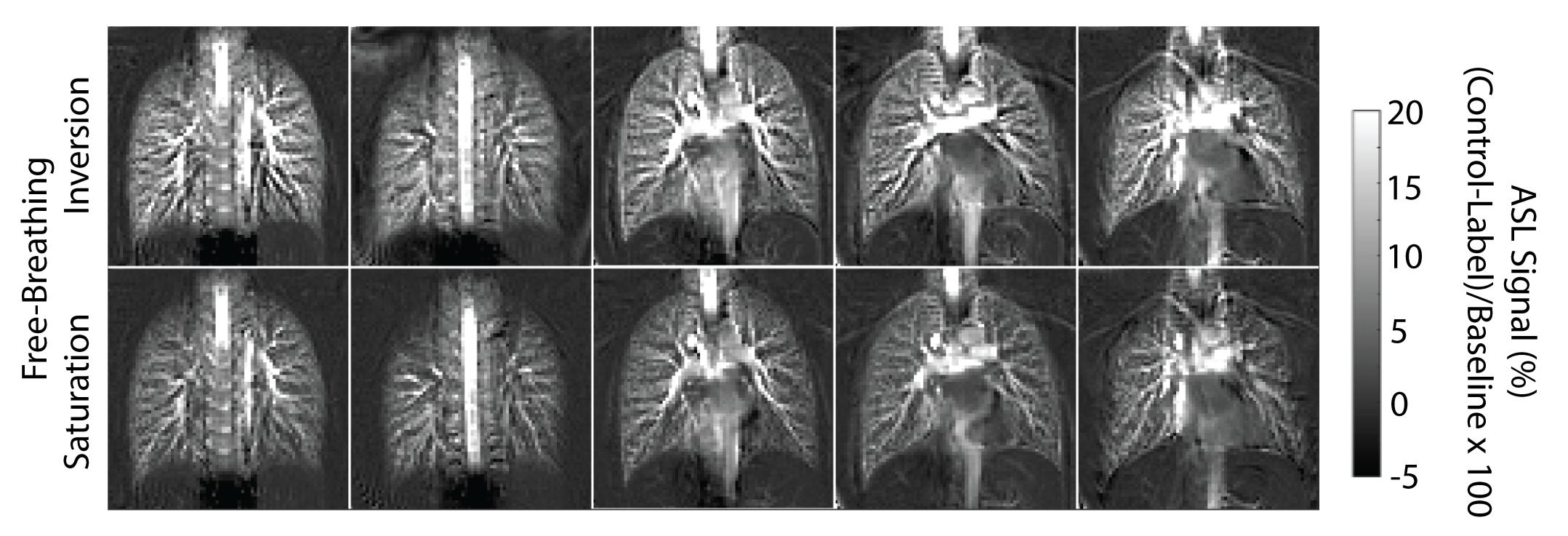
Figure 2 shows the representative pulmonary perfusion images in a healthy volunteer. They show the change in signal with varied post-labeling delays following an inversion pulse label. The ASL signal peaked between PLD 1200ms and 1500ms. This figure also shows a reduction in vessel signal with longer PLDs which may reduce the ASL measurement sensitivity to errors in segmentation if vessels are included in the segmentation masks.Figure 3 shows the comparison of ASL signal between BH and FB scans with saturation and inversion labelling. The figure shows that, as expected, saturation labeling has a lower ASL signal than inversion with almost no difference in signal stability across subjects. It also shows that FB measurements are comparable to BH measurements in terms of ASL signal measured. Figure 4 shows perfusion maps in multiple slices acquired in one HV using the same labeling place for all slices, demonstrating the labeling scheme's compatibility with whole lung coverage.
In the animal model, Figure 5 shows images without an occlusion, with a proximal occlusion and a distal occlusion of the right pulmonary artery. These images validate the ability of our method to detect severe perfusion defects.
Conclusion
We demonstrate a non-contrast pulmonary perfusion imaging method that can detect perfusion defects. Our method is free-breathing, easy to prescribe, and compatible with multi-slice imaging. We show that using an inversion labeling pulse with a PLD of 1500ms allows us to maximize ASL signal and leaves a slight buffer for changes in pulmonary transit time with lung disease. Future studies will explore the multi-slice application of this technique to patients with CTEPH and other cardiopulmonary diseases.Acknowledgements
This work was supported by the National Heart, Lung, and Blood Institute (NHLBI) Division of Intramural Research (Z01-HL006257, Z01-HL006213). The authors are investigators on a US Government Cooperative Research and Development Agreement (CRADA) with Siemens Healthcare to develop 0.55T MRI.References
1. Campbell-Washburn AE, Ramasawmy R, Restivo MC, et al. Opportunities in interventional and diagnostic imaging by using high-performance low-field-strength MRI. Radiology 2019;293:384–393 doi: 10.1148/radiol.2019190452.
2. Johns CS, Swift AJ, Rajaram S, et al. Lung perfusion: MRI vs. SPECT for screening in suspected chronic thromboembolic pulmonary hypertension. J. Magn. Reson. Imaging 2017;46:1693–1697 doi: 10.1002/jmri.25714.
3. Seith F, Pohmann R, Schwartz M, et al. Imaging Pulmonary Blood Flow Using Pseudocontinuous Arterial Spin Labeling (PCASL) With Balanced Steady-State Free-Precession (bSSFP) Readout at 1.5T. J. Magn. Reson. Imaging 2020;52:1767–1782 doi: 10.1002/jmri.27276.
4. Golay X, Stuber M, Pruessmann KP, Meier D, Boesiger P. Transfer Insensitive Labeling Technique (TILT): Application to Multislice Functional Perfusion Imaging. J. Magn. Reson. Imaging 1999;9:454–461 doi: 10.1002/(SICI)1522-2586(199903)9:3<454::AID-JMRI14>3.0.CO;2-B.
5. Avants B, Tustison N, Song G. Advanced Normalization Tools (ANTS). Insight J. 2009.
Figures