2751
FID-navigated motion correction for post-contrast T1w-imaging of kidneys1Radiology, Boston Children's Hospital and Harvard Medical School, Boston, MA, United States, 2Siemens Medical Solutions USA, Inc., Boston, MA, United States, 3Advanced Clinical Imaging Technology, Siemens Healthineers International AG, Lausanne, Switzerland, 4Department of Radiology, Lausanne University Hospital and University of Lausanne, Laussane, Switzerland, 5LTS5, École Polytechnique Fédérale de Lausanne (EPFL), Laussane, Switzerland
Synopsis
Keywords: Kidney, Motion Correction
Motivation: Post-contrast T1-weighted imaging is vital for diagnosing renal MRI by assessing vasculature, finding vascular abnormalities, and evaluating kidney function. However, breathing motion degrades image quality, which is problematic since breath-holding is difficult for some patients, especially children.
Goal(s): There is an urgent need for motion-robust renal imaging for breath-holding challenged patients.
Approach: In this study, we demonstrated the effectiveness of FIDnavs in correcting motion-related artifacts in clinical post-contrast T1w-imaging of kidneys. We evaluated our pipeline on 5 pediatric patients, both retrospectively and prospectively, using FIDnav-based motion correction (MoCo).
Results: Utilizing FIDnavs for MoCo, reduced motion artifacts and blurring in post-contrast T1w-imaging.
Impact: Use of FID-navigated motion correction for post-contrast T1w-imaging of kidneys can reduce motion artifacts and minimize the scan time by eliminating the need of gating. However, the calibration step required for prospective motion correction should be eased for pediatric patients.
Introduction
Post-contrast T1-weighted imaging is crucial in renal MRI to assess vasculature, vascular abnormalities, and kidney function1,2. However, heavy breathing motion negatively impacts image quality3, especially in breath-holding challenged patients like children. Radial acquisition helps reduce motion artifacts but remains affected by deep breathing in certain patients4-7. Gating is commonly employed to overcome problems related to motion, which prolongs the scan time. Motion correction (MoCo) techniques like XD-GRASP use the k-space-center navigator to bin data into respiratory phases, enabling motion-robust image reconstruction8. However, the k-space-center approach has limitations due to factors like gradient delays, causing trajectory errors9-11. We propose using free induction decay navigators (FIDnavs) for XD-GRASP instead, providing a respiratory trajectory without these limitations12. Previously, FIDnavs have shown promise for prospective MoCo in kidney imaging13. Here, we demonstrate FIDnavs' effectiveness in correcting motion artifacts in post-contrast pediatric renal T1-weighted imaging, evaluating retrospectively and prospectively on 5 patients. FIDnavs offer advantages including reduced spin-history effects and immediate image availability without post-processing. This study shows FIDnavs' potential adaption to clinical abdominal MRI exams for motion-robust imaging.Methods
FIDnavs with their own non-selective RF pulses were inserted into a golden angle-ordered radial stack-of-stars research application sequence. FIDnavs (ADC duration=0.4ms, TE=2 ms) were acquired once in each partition (or equivalently once in each rotation angle). FIDnavs inserted sequences were added to MRI protocols of five patients (2 female,3 male,age=16.2±2.6 years), who are undergoing a contrast-enhanced MRI exam, imaged at 3T Prisma/Skyra scanners (Siemens Healthineers, Erlangen, Germany), following written, informed consent.Retrospective MoCo: All patients were asked to perform free breathing during the FIDnav-navigated radial imaging. FIDnavs were captured in the same scan for each patient. After the scan, FIDnavs were extracted from the raw data. XD-GRASP reconstructions were performed by binning into five motion states based on FIDnavs. Furthermore, binning based on k-space-center navigator has been performed to compare with the performance of binning based on FIDnavs.
Prospective MoCo: For two of the patients who could follow breathing instructions, a short calibration scan was acquired to find linear motion model parameters converting FIDnavs measurements into kidney displacement. In the calibration scan, patients were asked to perform inhaling/exhaling alternatively every 5 seconds in total for 25 seconds. The computed model parameters were used for prospectively correcting kidney motion due to respiration in real-time by steering the imaging volume.
Imaging Parameters: The total scan time was 2.5 minutes for the FIDnav-inserted golden angle-ordered radial stack-of-stars sequence. Imaging parameters were TE/TR/FA = 1.49/4ms/9˚, 32 coronal oblique slices with slice Partial Fourier=6/8, voxel size=1.2x1.2x3mm3 and 1326 radial spokes. Note that one of the patients was imaged in the axial plane and others were imaged in the coronal-oblique plane (parallel to the longitudinal axis of the kidneys).
Results
In our retrospective MoCo experiments, XD-GRASP successfully generated motion-robust images using both the k-space-center and FID navigators in 4 out of 5 subjects. However, XD-GRASP with the k-space-center navigator performed poorly for subject #2 (Figure 1). Retrospective MoCo reconstruction significantly improved image quality compared to reconstruction without motion correction, as shown in Figure 2. Figure 3 compares the end-of-expiration states of FID-navigated XD-GRASP MoCo reconstructions for all 5 subjects with reconstructed images without motion correction, revealing motion artifacts caused by free-breathing. Additionally, Figure 4 presents the outcomes of our prospective MoCo experiments, comparing images reconstructed with prospective MoCo to those without MoCo, along with the end-expiration states of retrospective MoCo for two subjects.Discussion and Conclusion
XD-GRASP reconstruction yielded motion-robust images for both the k-space-center and FID navigators in four out of five subjects. However, XD-GRASP with the k-space-center navigator showed suboptimal performance for one subject (Figure 1). FID-navigated XD-GRASP MoCo successfully reconstructed motion-robust images, effectively addressing motion artifacts caused by breathing (Figure 3). Both of the proposed retrospective and prospective MoCo techniques, utilizing FIDnavs, reduced motion artifacts and blurring (Figure 4). Despite previous success in achieving motion-free images with FID-navigated prospective MoCo in adult subjects13, residual motion artifacts remain in the current implementation when applied to pediatric patients. This can be attributed to challenges in accurately calibrating FIDnav measurements to kidney displacement, especially considering the difficulties pediatric patients face in following breathing instructions during the short calibration scan. Hence, further simplifying the calibration scan process is necessary to enhance its applicability to pediatric patients. Once overcoming the problems mentioned above in prospective MoCo, it is expected to be advantageous over retrospective MoCo, especially in the cases of irregular breathing, shorter scans or the presence of spin-history effects13.Acknowledgements
This work was supported partially by the National Institute of Diabetic and Digestive and Kidney Diseases (NIDDK), National Institute of Biomedical Imaging and Bioengineering (NIBIB), National Institute of Neurological Disorders and Stroke (NINDS) and National Library of Medicine (NLM) of the National Institutes of Health under award numbers R01DK125561, R21DK123569, R21EB029627, R01NS121657, R01LM013608, S10OD0250111.References
- Grattan-Smith, J. Damien, and Richard A. Jones. "MR urography in children." Pediatric Radiology 36 (2006): 1119-1132.
- S. Kurugol et al., “Feed and Wrap Magnetic Resonance Urography Provides Anatomic and Functional Imaging in Infants Without Anesthesia,” J.Pediatr. Urol., 2019.
- Chavhan, Govind B., Paul S. Babyn, and Shreyas S. Vasanawala. "Abdominal MR imaging in children: motion compensation, sequence optimization, and protocol organization." Radiographics 33.3 (2013): 703-719.
- Feng L, Axel L, Chandarana H, Block KT, Sodickson DK, Otazo R. XD-GRASP: golden-angle radial MRI with reconstruction ofextramotion-state dimensions using compressed sensing. Magn Reson Med. 2016;75:775-788.
- Cruz G, Atkinson D, Buerger C, Schaeffter T, Prieto C. Accelerated motion corrected three-dimensional abdominal MRI using total variation regularized SENSE reconstruction. Magn Reson Med. 2016;75:1484-1498.
- Cheng JY, Alley MT, Cunningham CH, Vasanawala SS, Pauly JM, Lustig M. Nonrigid motion correction in 3D using autofocusing with localized linear translations. Magn Reson Med.2012;68:1785-1797.
- Coll-Font J, Afacan O, Chow JS, et al. Bulk motion-compensated DCE-MRI for functional imaging of kidneys in newborns. JMagn Reson Imaging. 2020;52:207–216.
- Feng, Li, et al. "XD-GRASP: golden-angle radial MRI with reconstruction of extra motion-state dimensions using compressed sensing." Magnetic resonance in medicine 75.2 (2016): 775-788.
- Brau ACS, Brittain JH. Generalized self-navigated motion detection technique: Preliminary investigation in abdominal imaging. Magn Reson Med. 2006;55(2):263-270.
- Kober T, Marques JP, Gruetter R, Krueger G. Head motion detection using FID navigators. Magn Reson Med. 2011;66(1):135-143.
- Wallace TE, Afacan O, Waszak M, Kober T, Warfield SK. Head motion measurement and correction using FID navigators. Magnetic Resonance in Medicine. 2019;81(1):258-274.
- Ariyurek C, Wallace TE, Kober T, Kurugol S, Afacan O. Comparison of k-space center, FID and Pilot Tone navigators in abdominal motion tracking for optimal XD-GRASP reconstruction In: Proceedings of the 31st Annual Meeting of ISMRM, Toronto, ON, Canada, 2023. p. 0348.
- Ariyurek C, Wallace TE, Kober T, Kurugol S, Afacan O. Prospective motion correction in kidney MRI using FID navigators. Magn Reson Med. 2023;89:276-285
Figures
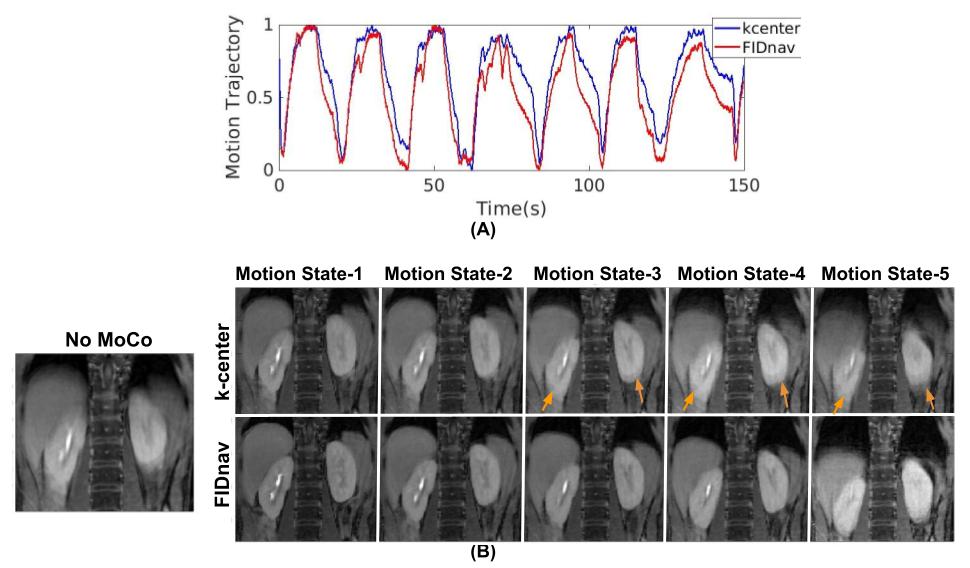
Figure 1: For Subject #2, (A) motion trajectories extracted from k-space-center and FID navigators, (B) comparison of no motion correction (‘no MoCo’)’, k-space-center and FID-navigated XD-GRASP for five motion states. Severe motion artifacts are observed in the images without motion correction (‘no MoCo’). Motion-robust images of kidneys are obtained by employing FID-navigated XD-GRASP. In contrast, blurring and motion artifacts are present with k-space-center-navigated XD-GRASP (orange arrows).
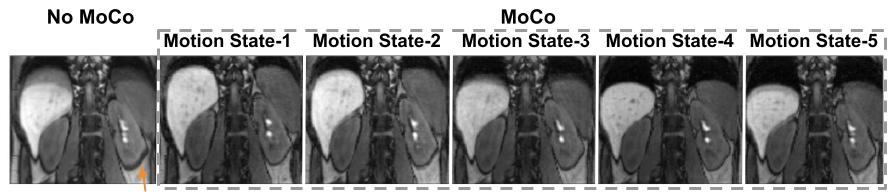
Figure 2: For a representative subject, FID-navigated XD-GRASP reconstructions for five motion states are compared with the reconstructed image without motion correction (‘no MoCo’). It is observed that FID-navigated XD-GRASP reconstruction successfully resolves motion into states. On the other hand, motion artifacts are present in the image reconstructed MoCo (‘no Moco’), shown by the orange arrow.
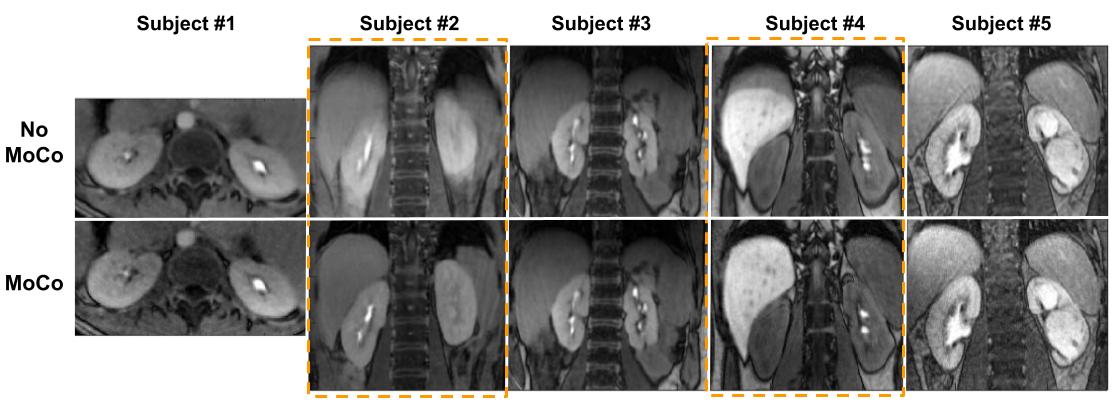
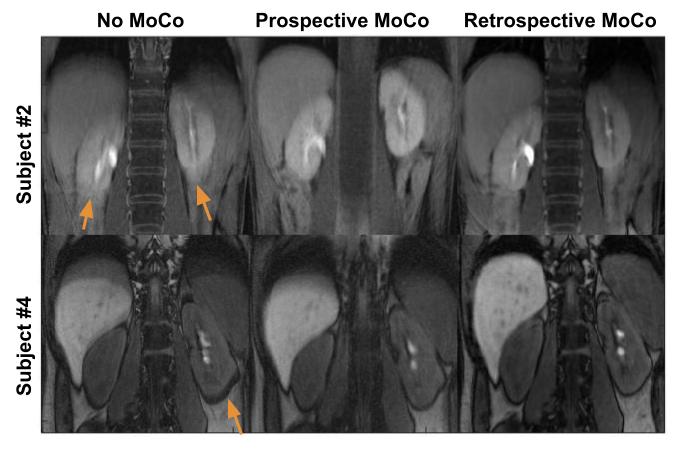
Figure 4: Our proposed FIDnav-based prospective and retrospective MoCo post-contrast T1w images are compared to images reconstructed with those without MoCo. Here, retrospective MoCo images represent the end-expiration states of FIDnav-based XD-GRASP MoCo images. Both the proposed prospective and retrospective FIDnav-based MoCo techniques reduce the motion artifacts present in images reconstructed without motion correction (‘No MoCo’) which are highlighted by the orange arrows.