2729
Towards Automated Deep Learning based MR-only Radiation Therapy Planning in <5mins MR Scan Time1GE HealthCare, Munich, Germany, 2University of Zurich, Zurich, Switzerland, 3GE HealthCare, Budapest, Hungary, 4Department of Radiation Oncology, Erasmus MC Cancer Institute, Rotterdam, Netherlands, 5Department of Radiology and Nuclear Medicine, Erasmus MC, Rotterdam, Netherlands, 6Department of Imaging Physics, TU Delft, Delft, Netherlands
Synopsis
Keywords: MR-Guided Radiotherapy, Radiotherapy, Deep Learning, MR-only, Radiation Therapy Planning
Motivation: Deep Learning (DL) is an enabling technology for MR-only Radiation Therapy Planning in terms of 1) MR to synthetic CT conversion and 2) automated Organ-At-Risk (OAR) segmentation.
Goal(s): To investigate the feasibility of DL based MR-only RT planning using accelerated MR protocols with <5mins scan time (not including tumor depiction).
Approach: Quantitative evaluation of synthetic CTs in terms of mean absolute error (MAE) and OAR segmentations in terms of Likert Score analysis.
Results: Preliminary results demonstrate the feasibility of DL-based MR-only RT in <5min scan time with only minor degradation of synthetic CT and OAR segmentation quality.
Impact: Deep Learning is an enabling technology for MR-only Radiation Therapy Planning. Here we demonstrate its capabilities for 1) synthetic CT conversion and 2) Organ-At-Risk (OAR) segmentation in <5min MR scan time.
Introduction
Its exquisite soft tissue contrast favors MRI for Radiation Therapy (RT) planning, where accurate delineation of the tumor target and surrounding organs at risk (OARs) is essential. However, MRI does not provide electron density information required for accurate dose calculation, which typically requires an extra planning CT (thereby also requiring an extra patient visit, and causing additional cost, complexity, and radiation burden). In ongoing developments towards MR-only RT planning (i.e., no extra planning CT) Deep Learning (DL) plays a fundamental role by enabling 1) the conversion of MR into synthetic CT images (as required for dose calculation), 2) the automated segmentation of OARs (thereby shortening laborious manual segmentation), and 3) improving MR imaging performance (in terms of speed and image quality) using novel DL-based image reconstruction methods1,2,3.In this abstract, we investigate DL-based MR-only RT planning for head&neck in terms of synthetic CT conversion and OAR segmentation. Additionally, we investigate acceleration methods to shorten the required MR scan time by almost a factor of ~x3 from 6mins12sec to 2mins14sec taking advantage of DL-based image reconstruction. Short scan time is especially important for RT planning in the head&neck region from a patient acceptance perspective, since the MR imaging occurs in fixation (using a thermoplastic facial mask) to assure consistent positioning during imaging and treatment.
Methods
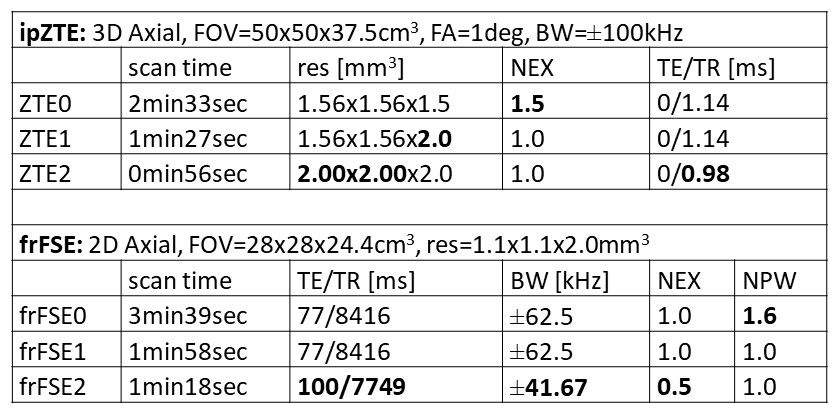
The DL-based MR-only RT planning for head&neck contains 1) a 3D in-phase Zero TE (ipZTE) acquisition as input for the synthetic CT conversion and 2) a 2D multi-slice fast-recovery fast spin echo (frFSE) acquisition as input for the OAR segmentation. For each sequence, the default protocol plus two accelerated variants were tested with protocol parameters summarized in Tab. 1.Synthetic CT images were derived from ipZTE MR images using a 2D multi-task UNet convolutional neural network (CNN)4. Automated segmentations of 27 OAR structures were derived from the 2D FSE images using a combination of 2D and 3D UNet CNNs2.
This ethics-approved study contained a total of N=48 oncology patients with head&neck cancers routed for RT treatment. The accelerated ipZTE and FSE protocols were added and tested for the last N=3 patients. The MR-scanning was performed in fixation using a 1.5T GE MR450w scanner with AIR Recon DLTM,6 image reconstruction and a dedicated RT head&neck coil array and flat tabletop (GE HealthCare, Chicago, IL) to accommodate consistent positioning between the imaging and the treatment. Manual tumor delineation was performed based on an extra contrast-enhanced 3D gradient echo sequence including fat-water separation (i.e., LAVA-FLEXTM). For clinical standard of care also a planning CT was acquired.
Results & Discussion
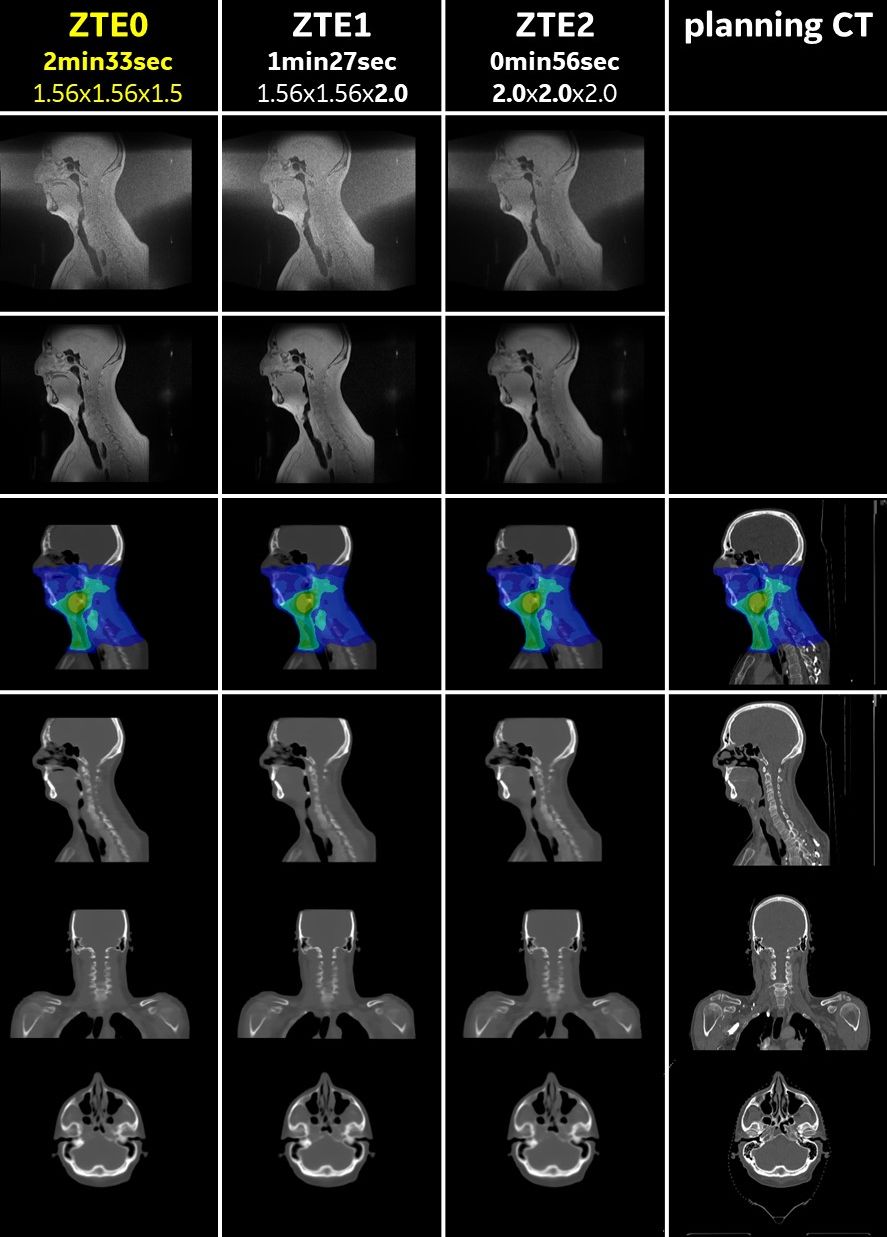
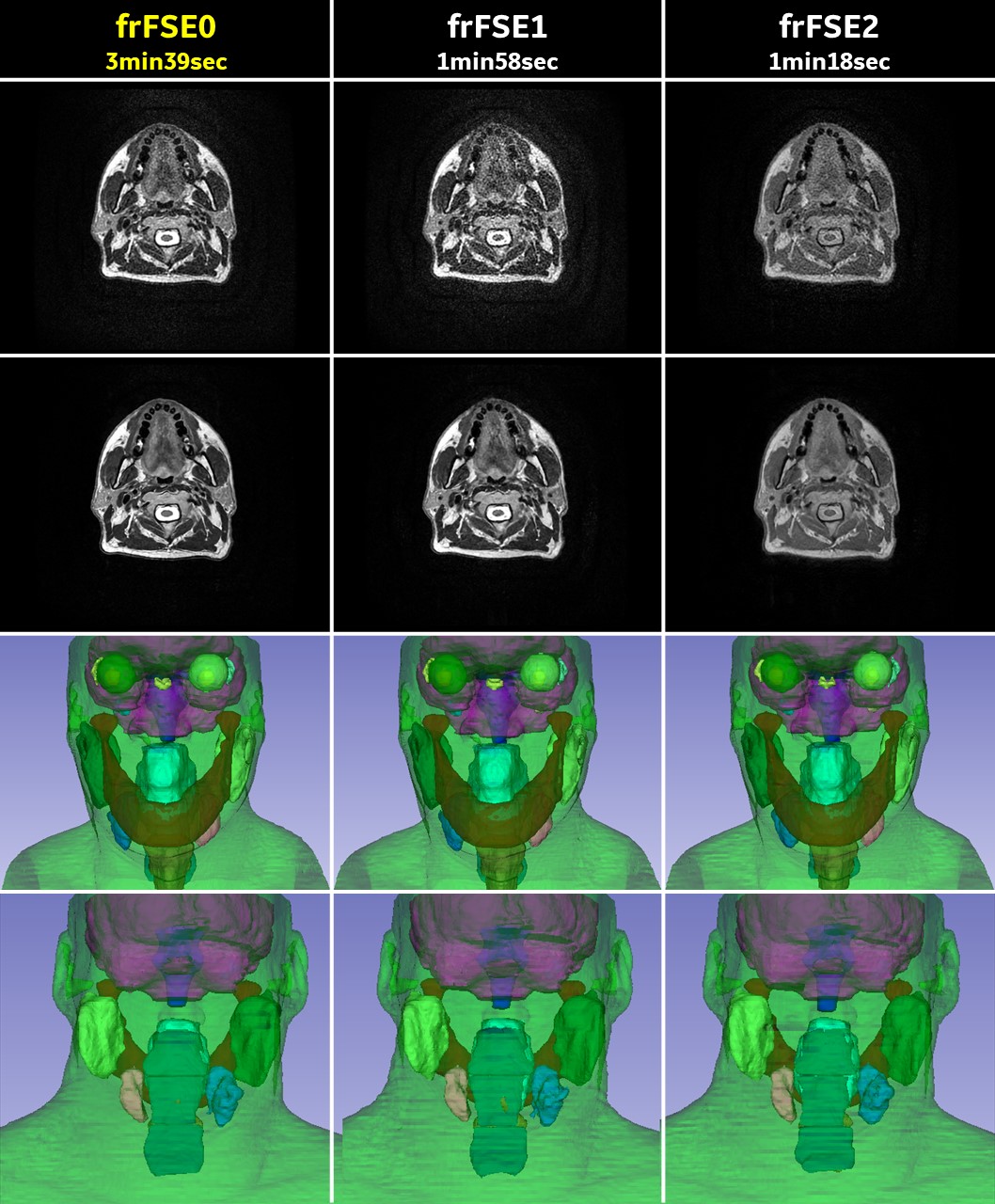
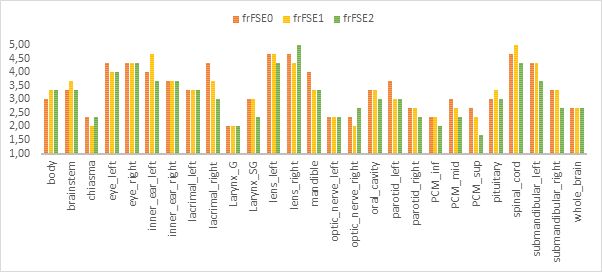
Figure 1 illustrates the synthetic CT images derived from the different ipZTE image inputs for an exemplary patient (#47). The mean-absolute-error (MAE relative to the registered planning CT) was found to be 98.39+/-13.44HU, 99.78+/-12.95HU, and 110.08+/-10.16HU for the ipZTE0, ipZTE1, and ipZTE2 derived synthetic CTs, respectively, with mean dose differences <1Gy for all planning target volumes (PTVs) and surrounding OARs.Figure 2 shows the three different frFSE images using standard reconstruction (top row), DL-enhanced reconstruction (2nd row) and corresponding DL-based automated OAR segmentations illustrated as 3D renderings from anterior (3rd row) and posterior (4th row) view. While image appearance is identical for frFSE0 and frFSE1 (left and right), the T2-contrast is notably different for frFSE2 (primarily due to difference in TE and TR). Independent of minor T2-contrast variations (i.e., for frFSE2) the DL-based OAR segmentation output was very similar for all three cases which was was confirmed by the Likert Score analysis summarized in Figure 3 (covering 27 OARs and three patients). Overall, the accelerated protocols resulted in only a relatively minor degradation of the segmentation outcome primarily affecting structures in the neck region which are also difficult to segment using the default frFSE0 protocol.
Conclusions
The obtained results indicate that MR scans for MR-only RT planning in the head & neck (in terms of synthetic CT and OAR segmentation) can be performed in <5min (i.e., 2min14 for the fastest accelerated protocol combination). Further improvements are expected via additional MR protocol optimization and retraining the DL CNNs with corresponding data augmentations. The shorter scan time minimizes motion (e.g., swallowing), improvise improves patient comfort (i.e., shorter MR imaging in fixation), and saves cost.Acknowledgements
This research is part of the Deep MR-only Radiation Therapy activity (project numbers 19037, 20648, and 210995) that has received funding from EIT Health. EIT Health is supported by the European Institute of Innovation and Technology, a body of the European Union that receives support from the Horizon 2020 Research and innovation program.References
- Jonsson, J., Nyholm, T., & Söderkvist, K. (2019). The rationale for MR-only treatment planning for external radiotherapy. Clinical and translational radiation oncology, 18, 60-65.
- Goodburn, R. J., Philippens, M. E., Lefebvre, T. L., Khalifa, A., Bruijnen, T., Freedman, J. N., ... & Gurney‐Champion, O. J. (2022). The future of MRI in radiation therapy: Challenges and opportunities for the MR community. Magnetic resonance in medicine, 88(6), 2592-2608.
- Spadea, M. F., Maspero, M., Zaffino, P., & Seco, J. (2021). Deep learning based synthetic‐CT generation in radiotherapy and PET: a review. Medical physics, 48(11), 6537-6566.
- Kaushik, S. S., Bylund, M., Cozzini, C., Shanbhag, D., Petit, S. F., Wyatt, J. J., ... & Menze, B. (2023). Region of interest focused MRI to synthetic CT translation using regression and segmentation multi-task network. Physics in Medicine & Biology, 68(19), 195003.
- Kolozsvari, B., Czipczer, V., Deák-Karancsi, B., Capala, M. E., Pearson, R. A., Borzási, E., ... & Ruskó, L. Comprehensive deep learning-based framework for automatic organs-at-risk segmentation in head-and-neck and pelvis for MR-guided radiation therapy planning. Frontiers in Physics, 11, 1236792.
- Lebel, R. M. (2020). Performance characterization of a novel deep learning-based MR image reconstruction pipeline. arXiv preprint arXiv:2008.06559.
Figures