2725
Whole Brain Coverage Multi-Target Framework for Benchmarking RF Arrays Tailored for Thermal Magnetic Resonance of Glioblastoma Multiforme1Berlin Ultrahigh Field Facility (B.U.F.F.), Max-Delbrück Center for Molecular Medicine in the Helmholtz Association, Berlin, Germany, 2FG Theoretische Elektrotechnik, Technische Universität Berlin, Berlin, Germany, 3a joint cooperation between the Charité Medical Faculty and the Max-Delbrück Center for Molecular Medicine, Berlin, Germany, 4MRI.TOOLS GmbH, Berlin, Germany
Synopsis
Keywords: Interventional Devices, Simulations, Brain Tumor, UHF-MRI, Thermal Therapy, Multi-Target Evaluation
Motivation: Thermal Magnetic Resonance (ThermalMR) adds a thermal intervention dimension to MRI by focusing E-fields in the target region (TR). Today’s assessment of RF applicators uses TRs covering a few specific but arbitrary locations in the brain. This approach does not represent the full clinical picture.
Goal(s): This work introduces a multi-target evaluation (MTE) framework and expands RF applicator evaluation to whole brain coverage.
Approach: MTE using EMF simulations for a helmet and for an annular RF applicator.
Results: Our MTE approach provides a technical foundation for the development and objective evaluation of RF applicators tailored for ThermalMR.
Impact: MTE provides a technical foundation for objective RF applicator evaluation using whole brain coverage instead of a few specific but arbitrary target locations. Our framework presents a springboard for RF applicator design and for ThermalMR-based therapy of glioblastoma multiforme.
Introduction
Adding a thermal intervention dimension to MRI is conceptually appealing for local thermal therapy as an adjuvant to cancer chemo- and radiotherapy1. Thermal Magnetic Resonance (ThermalMR) exploits localized RF power deposition to induce targeted heating in tissue2. Ultrahigh field (UHF) MRI is an excellent fit for ThermalMR. It offers enhanced localized temperature manipulation as it operates at shorter wavelengths compared to MRI at lower fields. Assessment of RF building blocks and ThermalMR RF applicators commonly use target volume locations covering a few very specific but arbitrary areas of the brain. To address this shortcoming this work introduces a multi-target evaluation (MTE) framework for RF applicator evaluation. The MTE approach expands the evaluation from a limited number of arbitrary tumor locations in the brain which do not represent the full clinical picture to whole brain coverage. For this purpose, we conducted numerical simulations moving a target region (TR) across the entire brain.Methods
Electromagnetic field (EMF) simulations were performed in CST Microwave Studio (CST Studio Suite 2020, Dassault Systèmes) at 297.2 MHz. 3-6 The maximum Specific Absorption Rate (SAR) in a target region (TR) was benchmarked for two RF array configurations, each assembled from ten bbSGBT building blocks: 1. a 10-channel TX array using a symmetric annular array (AA) arrangement; 2. a helmet array (HA) configuration with 8 channels arranged in a symmetric annular array plus two channels placed perpendicular above the head (Figure1a). EMF simulations (f=297 MHz) were performed using the head of the human voxel model Duke.7 SAR10g was determined according to the IEEE/IEC standard 62704-1. First, we targeted four cuboid target regions (Figure1b, green line:SARavg > 40W/kg, red line: safe margin zone, SAR10g,max<40 W/kg) mimicking glioblastoma multiforme. For a more comprehensive assessment of the RF applicators, we expanded the evaluation from four arbitrary tumor locations to whole brain coverage using the MTE framework (Figure1b). For this purpose, numerical simulations moving hypothetical TRs across the entire brain (Figure1b) were conducted (step size=7mm, total number of locations=26*27=702 using 4 TR sizes. For both approaches, constructive E-field interference in the TR was achieved with an MVFS-focusing method8. Target coverage (TC) was used as a metric for the quality of RF heating. TC defined as the volume percentage that is covered by 25%, 50%, and 75% of the maximum SAR10g over 40 W/kg as a .Results
Figure 2 shows MTE results obtained for the entire brain using four different TR sizes. For the top and lower areas of the brain, the HA yielded a larger maximum SAR10g(SAR10g,max) than the AA. Figure2 demonstrates that a larger maximum and mean SAR10g(SAR10g,mean) can be reached for the larger TRs. The success score is presented in Figure2b which shows 20.3%, 40%, 56%, and 46.1% higher scores using the HA versus the AA.Figure3b-d illustrates the metric TCxx which describes the volume that covers xx% (xx=25, 50, and 75) of the maximum SAR10g inside the TR. For the large TR, TCxxs provided by the AA were superior to the HA counterparts for the top regions of the brain. For lower and deep-lying regions of the brain, the HA showed higher TCxxs than the AA. For middle brain regions both RF applicators showed similar uniform SAR10g distribution in the TRs. For smaller TRs, the HA was superior to the AA for all brain regions.
Boxplots (Figure 4a) obtained for whole brain coverage using 702 TRs demonstrate that the highest maximum SAR10g (73 W/kg) and SAR10g,mean(111 W/kg) is obtained by the HA although their interquartile range is very close (SAR10g,mean: 11 W/kg (HA) and 7 W/kg (AA), SAR10g,max: 18 W/kg (HA), 19 W/Kg (AA)) (Figure 4a). Figure4b shows higher TC25 for the AA vs. the HA. For TC50 and TC75 the HA outperformed the AA.
Discussion and Conclusion
ThermalMR integrates RF-induced heating, in vivo MR thermometry, and anatomical and functional imaging in a single multi-purpose RF applicator. Benchmarking of ThermalMR applicators is challenging so far. To address this challenge we developed and implemented the MTE approach. We examined the applicability of the MTE approach in a case study, which involved two RF applicators: a HA and an AA. Our case study demonstrates that the HA RF applicator facilitates a ~20% improvement of maximum SAR10g in the TR, with enhanced target coverage compared to the AA. To conclude, our work provides a technical foundation for objective RF applicator evaluation using whole brain coverage instead of a few specific but arbitrary target locations. This achievement presents a springboard for RF applicator design and for ThermalMR-based therapy of brain tumors.Acknowledgements
This project received funding from the European Research Council (ERC) under the European Union's Horizon 2020 research and innovation program under grant agreement No 743077 (ThermalMR) and from the Innovative Training Network (ITN) H2020-MSCA-ITN-2020-955625 of the Marie Skłodowska-Curie Actions of the European Union.References
1. Wust, P., et al. Hyperthermia in combined treatment of cancer. The lancet oncology 3, 487-497 (2002).
2. Oberacker, E., et al. Patient-Specific Planning for Thermal Magnetic Resonance of Glioblastoma Multiforme. Cancers 13(2021).
3. Oberacker, E., et al. Radiofrequency applicator concepts for thermal magnetic resonance of brain tumors at 297 MHz (7.0 Tesla). International journal of hyperthermia : the official journal of European Society for Hyperthermic Oncology, North American Hyperthermia Group 37, 549-563 (2020).
4. Winter, L., et al. Design and evaluation of a hybrid radiofrequency applicator for magnetic resonance imaging and rf induced hyperthermia: electromagnetic field simulations up to 14.0 Tesla and proof-of-concept at 7.0 Tesla. PLoS One 8, e61661 (2013).
5. Eigentler, T.W., et al. Wideband Self-Grounded Bow-Tie Antenna for Thermal MR. NMR in biomedicine 33, e4274 (2020).
6. Han, H., et al. Multi-Channel RF Supervision Module for Thermal Magnetic Resonance Based Cancer Therapy. Cancers 13(2021).
7. Christ, A. The virtual family project-development of anatomical whole-body models of two adults and two children. Proc. 23rd Annual Review of Progress in Applied Computational Electromagnetics (ACES) 2007 (2007).
8. Kuehne, A., Oberacker, E., Waiczies, H. & Niendorf, T. Solving the time-and frequency-multiplexed problem of constrained radiofrequency induced hyperthermia. Cancers 12, 1072 (2020)
Figures
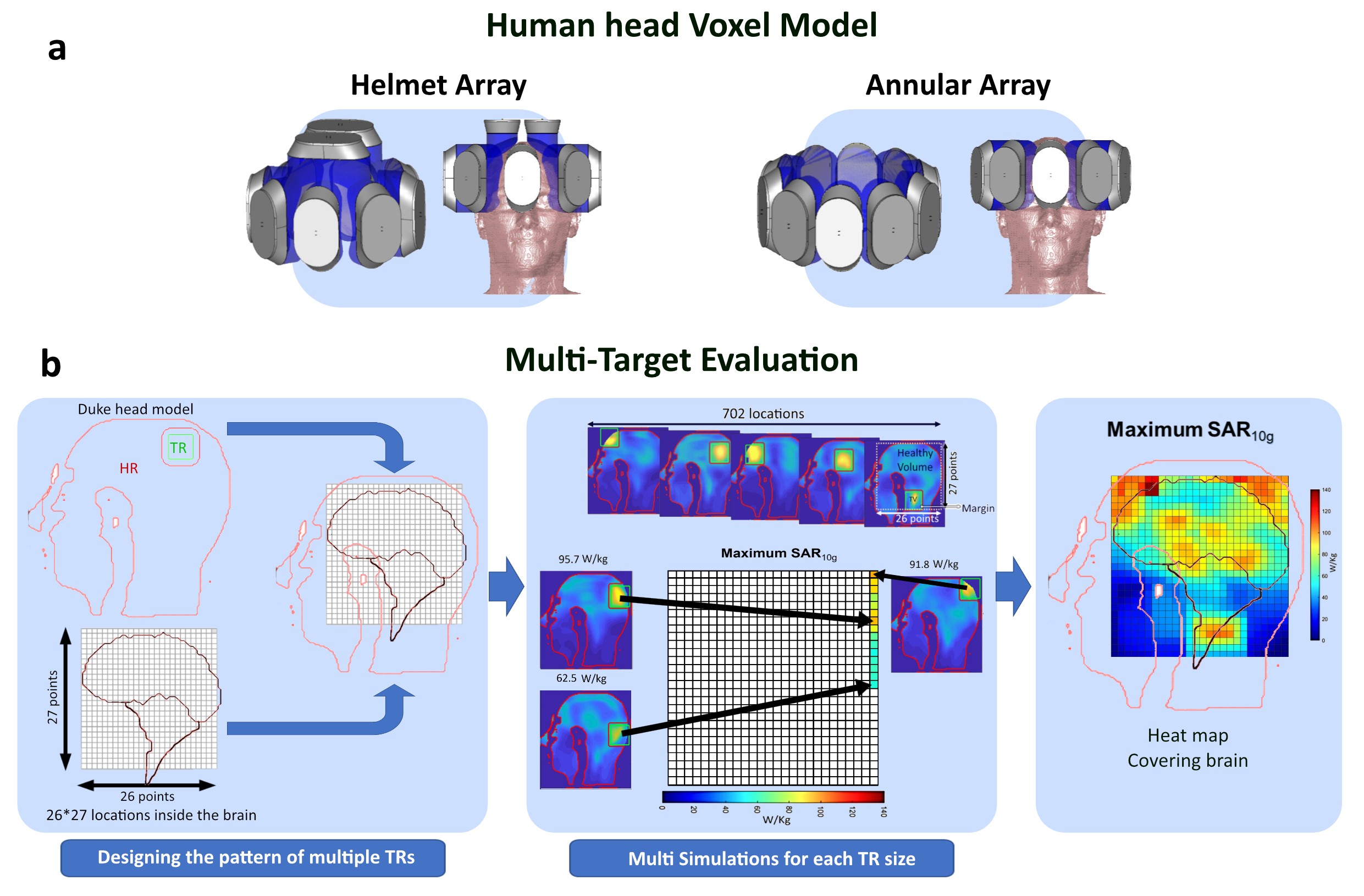
Figure 1. a) Illustration of the HA and AA RF Applicators assembled from 10-bbSGBT on a head of the human voxel model Duke. b) EMF simulations in CST of both RF applicators at 297.2 MHz showing SAR10g distribution in one example TR with a focusing method8 for four sizes of Cuboid TRs: TR1=30.625cm3 (37.5mm) (main target volume(cm3), gap difference(mm)); TR2=15.62cm3 (20mm); TR3=5.62cm3 (20mm); and TR4=0.9cm3(20mm). C) MTE. The simulation results for defined TRs were compared across a rectangular grid (step size=7mm) surrounding the brain to fill the heatmap. Brain outline is depicted.
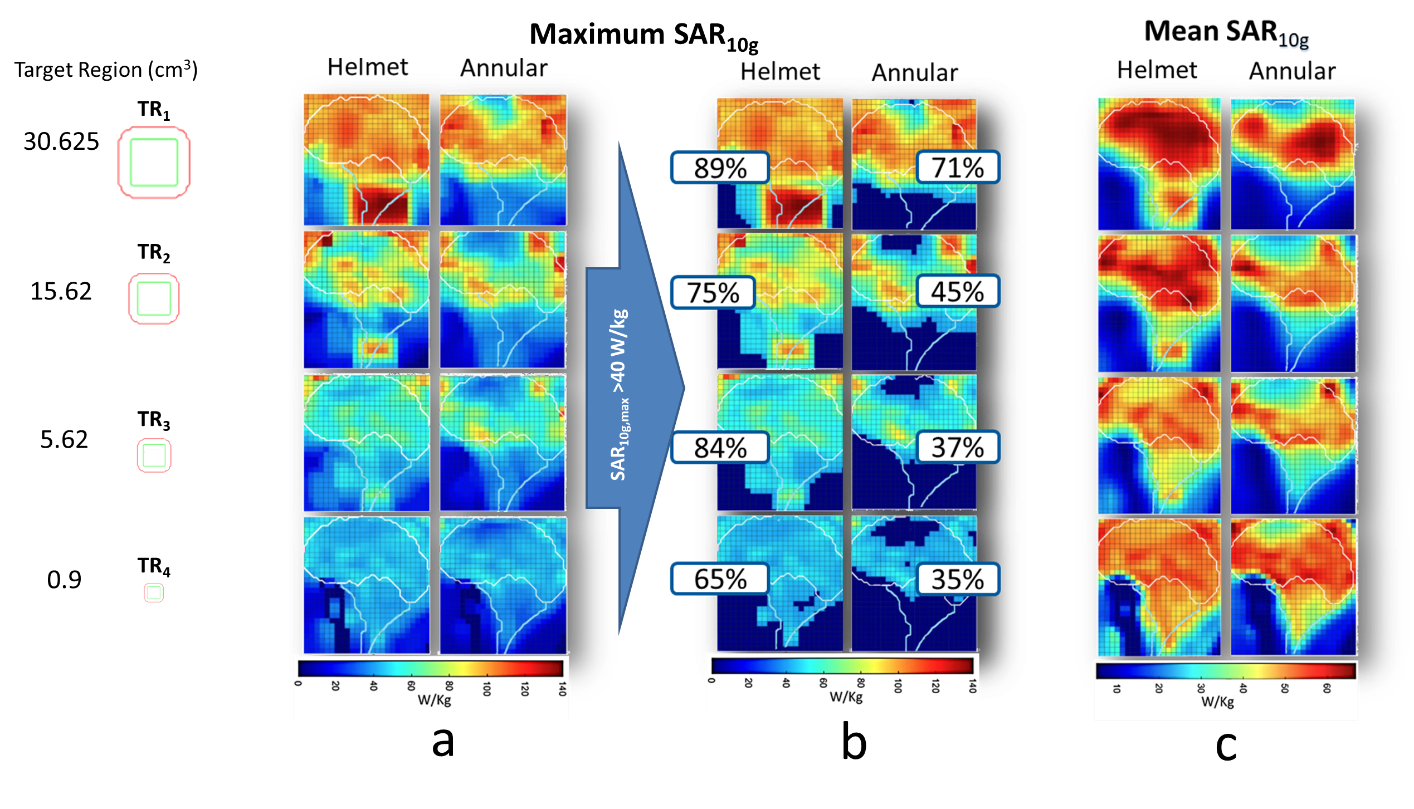
Figure 2. For 4 different sizes of TRs (cm3), heat maps for a) SAR10g,max , b) SAR10g,max>40 w/kg and annotated by success scores showing the percentage of TR locations (voxels) reaching the acceptable SAR10g,max higher than 40w/kg divided by number of total voxels (702), and c) heatmaps of SAR10g,mean. The outline of the brain is depicted in white.
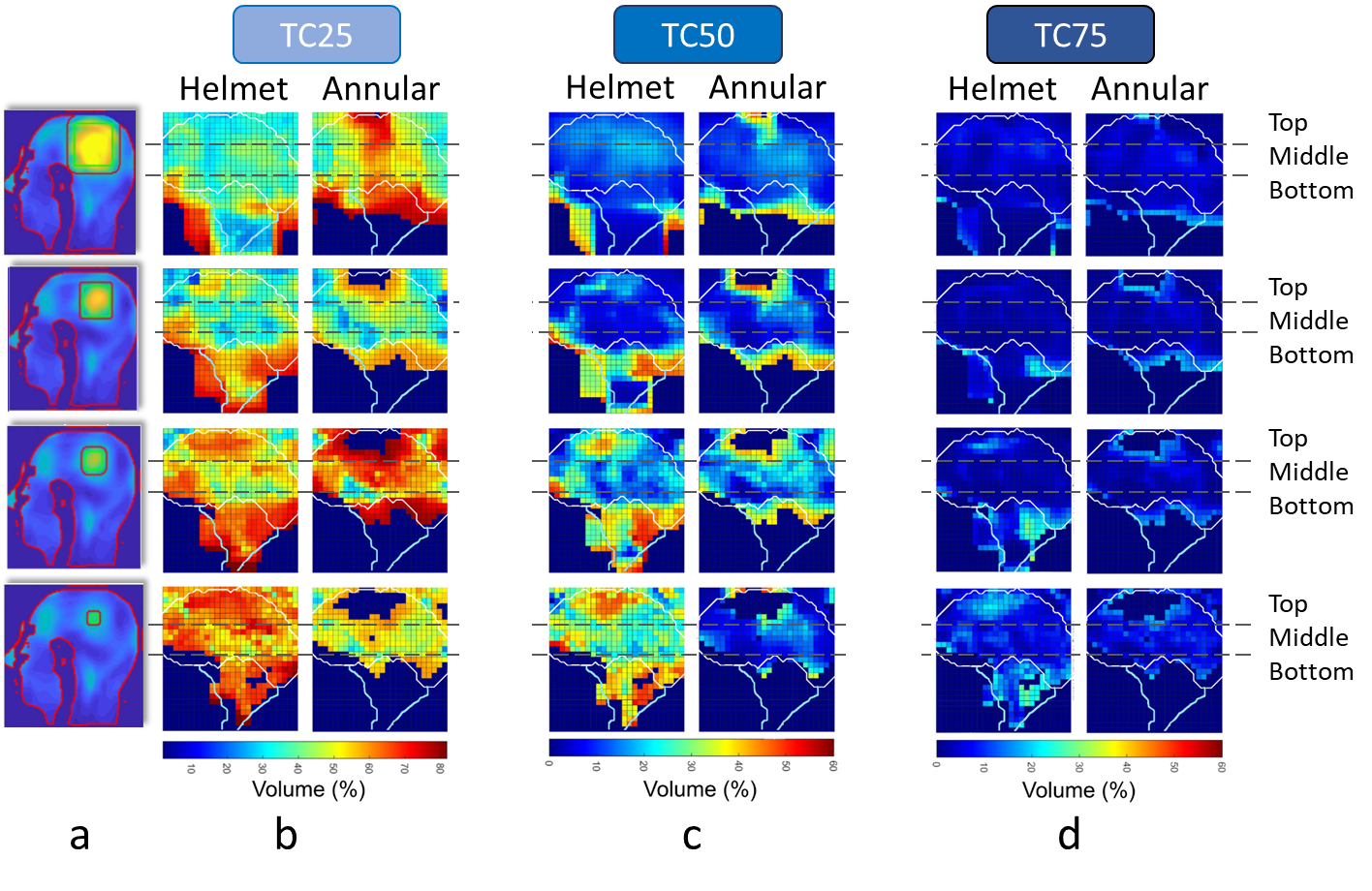
Figure 3. a) SAR10g distribution in four TR sizes by applying the focusing method in one arbitrary location. SAR10g-based Target coverage (TCxx= percent of volume covered by xx% of the maximum SAR10g in the TR) as an indicator of homogeneity using MTE is shown as a) TC25, b) TC50, and c) TC75. The outline of the brain is depicted in white. It is divided by gray dash lines to 3 areas named top, middle, and bottom.
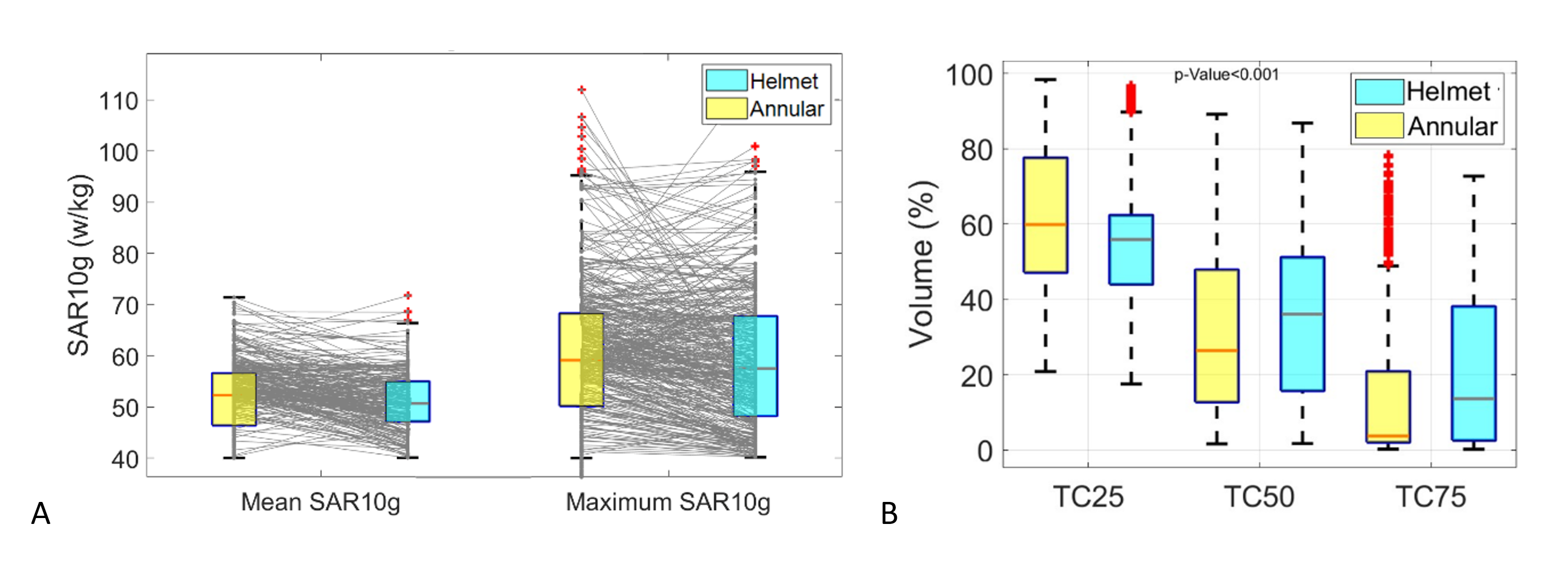
Figure 4. Comparison of Helmet and Annular arrays for TR3 (5.62 cm3) for a) SAR10g,max and SAR10g,mean values including coordinate lines that connect values in HA and AA for the same location, and b) TC25, TC50, and TC75 values.