2719
Improved MRI Guided Interventions at 0.55T: Real-time Interactive Imaging with Deep Learning Reconstruction1Siemens Medical Solutions USA, Inc., Malvern, PA, United States, 2Siemens Healthineers AG, Erlangen, Germany
Synopsis
Keywords: MR-Guided Interventions, MR-Guided Interventions
Motivation: Contemporary low-field MRI systems hold great promise for guiding interventions. However, due to inherently reduced polarization at lower field, it is more challenging to achieve high-spatiotemporal-resolution with sufficient SNR in interactive real-time imaging.
Goal(s): To improve real-time interactive imaging for MRI guided interventions at 0.55T by leveraging deep learning image reconstruction.
Approach: We implemented deep learning image reconstruction for interactive real-time imaging, and compared its performance with conventional parallel imaging reconstruction and compressed-sensing on a biopsy phantom and a healthy volunteer.
Results: Deep learning image reconstruction allows for accelerated interactive real-time imaging, achieving image quality that compared favorably with conventional reconstructions and compressed-sensing.
Impact: The proposed method has the potential to further empower 0.55T MRI as a viable interventional guidance platform by leveraging deep learning image reconstruction in accelerated interactive real-time imaging.
INTRODUCTION
Contemporary low-field MRI systems hold great promise for guiding interventions, primarily owing to reduced device heating, lower susceptibility artifacts, and better bore access1,2. However, due to inherently reduced polarization at lower field, it is more challenging to achieve high spatiotemporal resolution with sufficient SNR in interactive real-time imaging, a workhorse for guiding interventions. In recent years, Deep Learning (DL) has set a new level for image quality achievable with MR reconstruction3,4, which facilitates highly accelerated data acquisition and enhanced SNR through efficient denoising. These advantages, in particular, carry significant potential for low-field MR-guided interventions. In this study, we implemented deep learning based image reconstruction for interactive real-time imaging at 0.55T, and compared its performance with conventional parallel imaging reconstruction and compressed sensing on an abdominal biopsy phantom (with inserted needle) and a healthy volunteer.METHODS
Interactive real-time sequence and advanced image reconstruction:Data were acquired on a 0.55T scanner (MAGNETOM Free.Max, Siemens Healthineers, Erlangen, Germany) with an interactive real-time research application sequence with balanced steady-state free precession (bSSFP) readout. Acceleration was achieved by uniformly undersampling the Cartesian k-space. We compared three different reconstruction methods: conventional GRAPPA, compressed sensing (CS) using FISTA iterative algorithm and Haar wavelet regularization5, and DL reconstruction using an unrolled network with iterative data consistency and CNN-based regularization steps6. All reconstruction algorithms are implemented inline. Both CS and DL reconstructions use GPU to achieve sufficiently low latency.
Abdominal biopsy phantom with needle insertion:
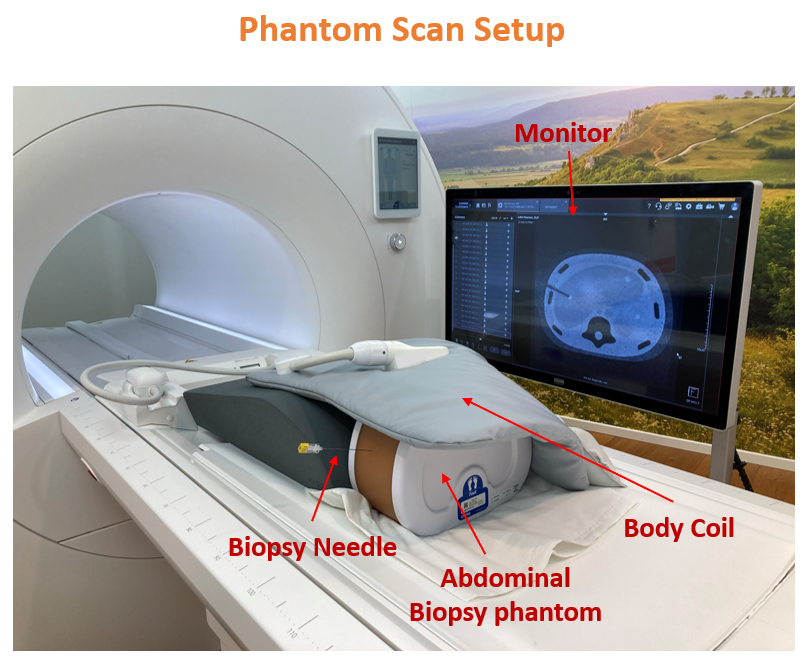
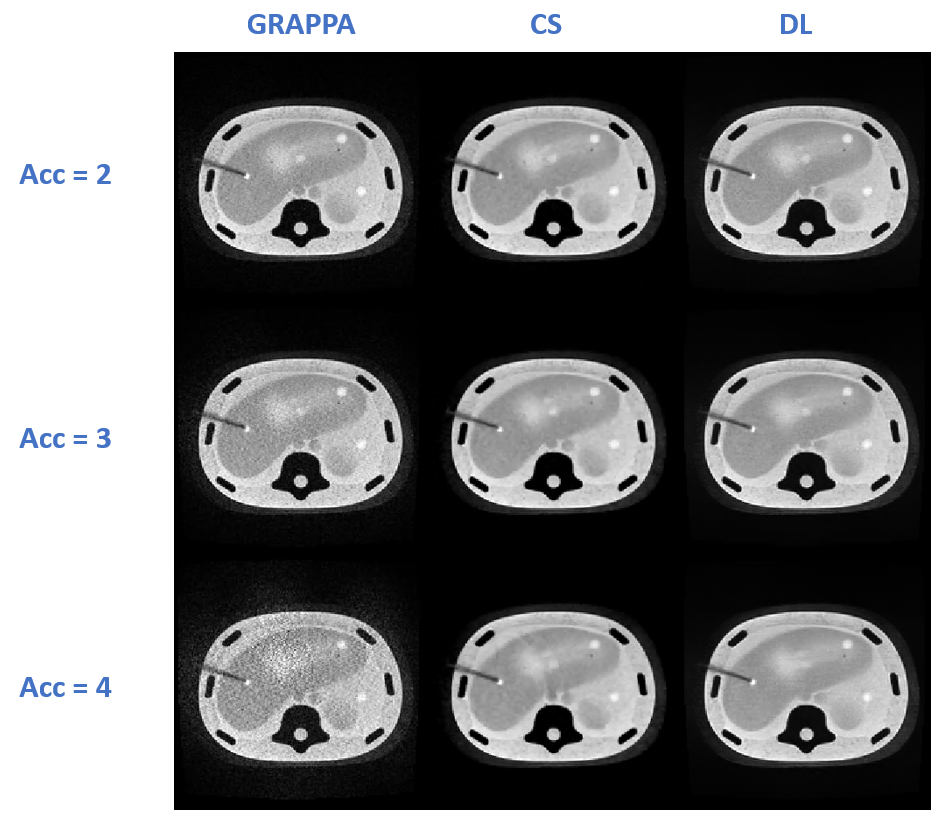
A multi-modality abdominal biopsy phantom (Computerized Imaging Reference Systems, Inc., Norfolk, VA, USA) was used. A flexible six channel surface coil (BioMatrix Contour L) and the built-in nine channel spine coil were used for signal reception (see Figure 1). A biopsy needle (KIM 20/15 ITP, Bochum, Germany) was manually inserted into the phantom to the target lesion. During needle insertions, interactive real-time imaging was performed with acceleration factors of 2, 3 and 4. Each was repeated with reconstruction of GRAPPA, CS and DL. Image parameters: FOV = 300x300mm2; matrix size = 192x192; resolution = 1.56x1.56mm2; thickness = 8mm; TE = 2.67msec; TR = 749/552/450 msec for acceleration factor of 2, 3, and 4, respectively; 24 integrated reference lines; 7/8 partial Fourier; FA = 90°; single slice per measurement; 50 measurements in total.
Healthy Volunteer:
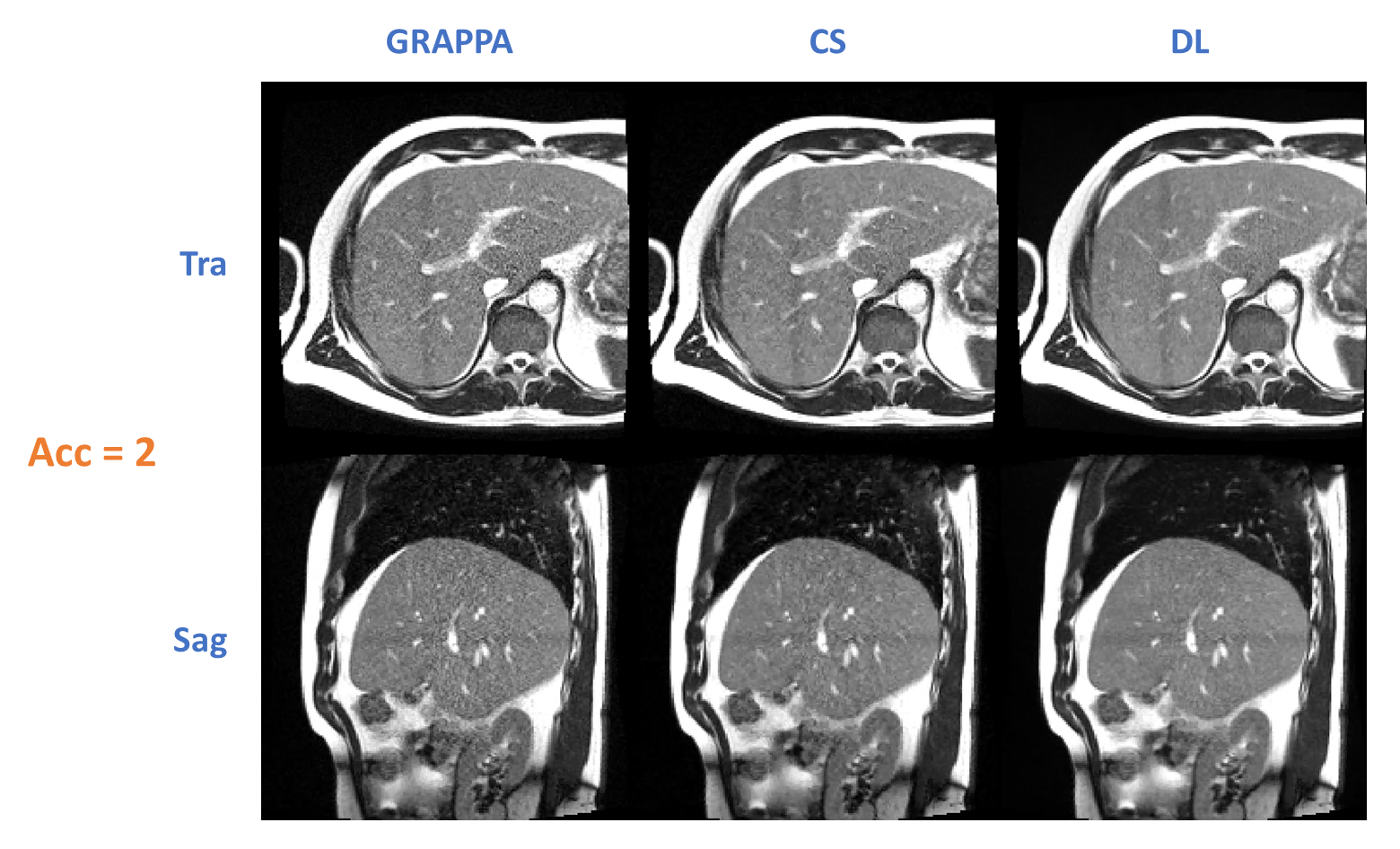
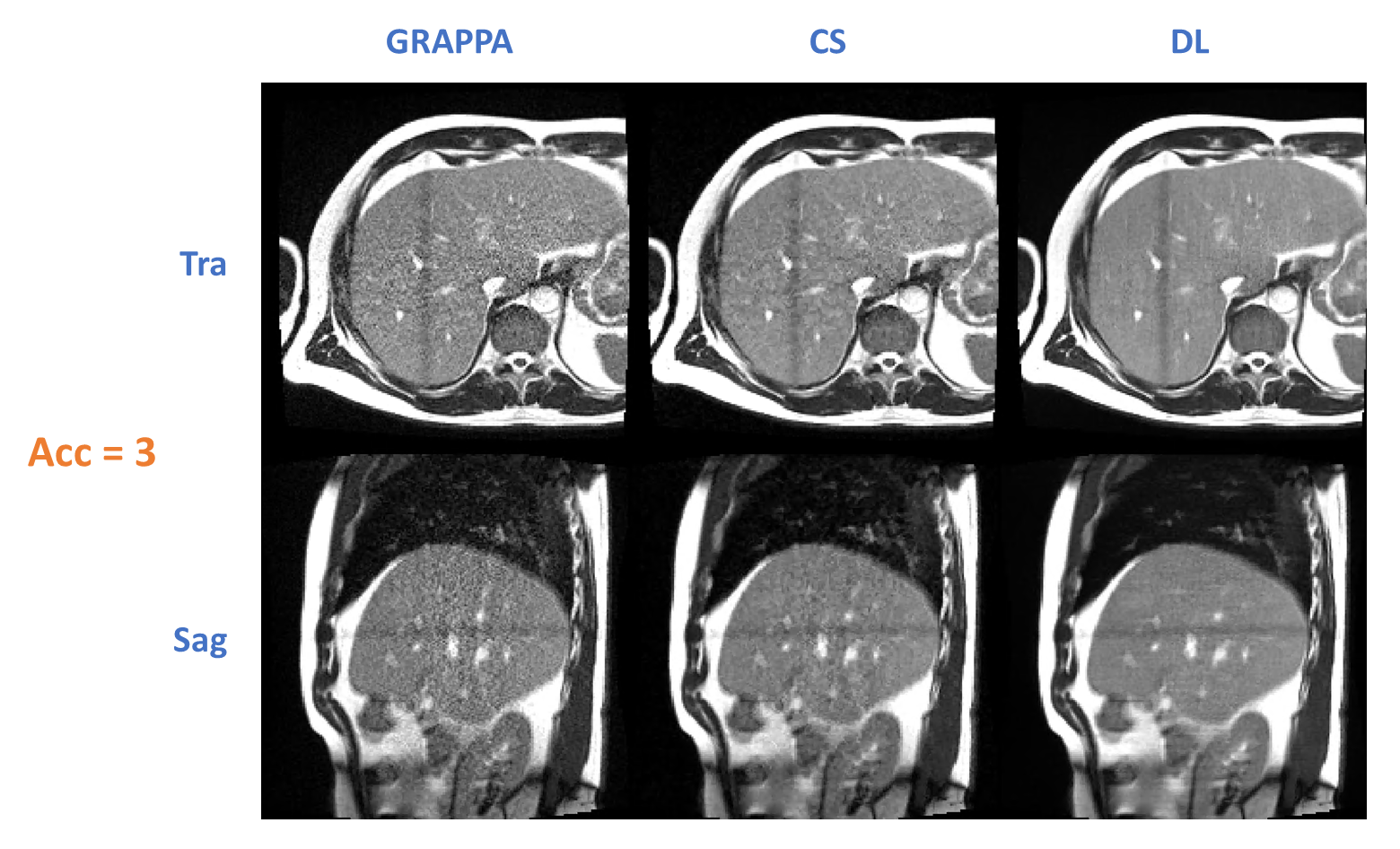
A healthy volunteer was imaged using the same sequence, coil, and reconstruction setup, except two slices (transverse and sagittal) were acquired consecutively per measurement.
RESULTS
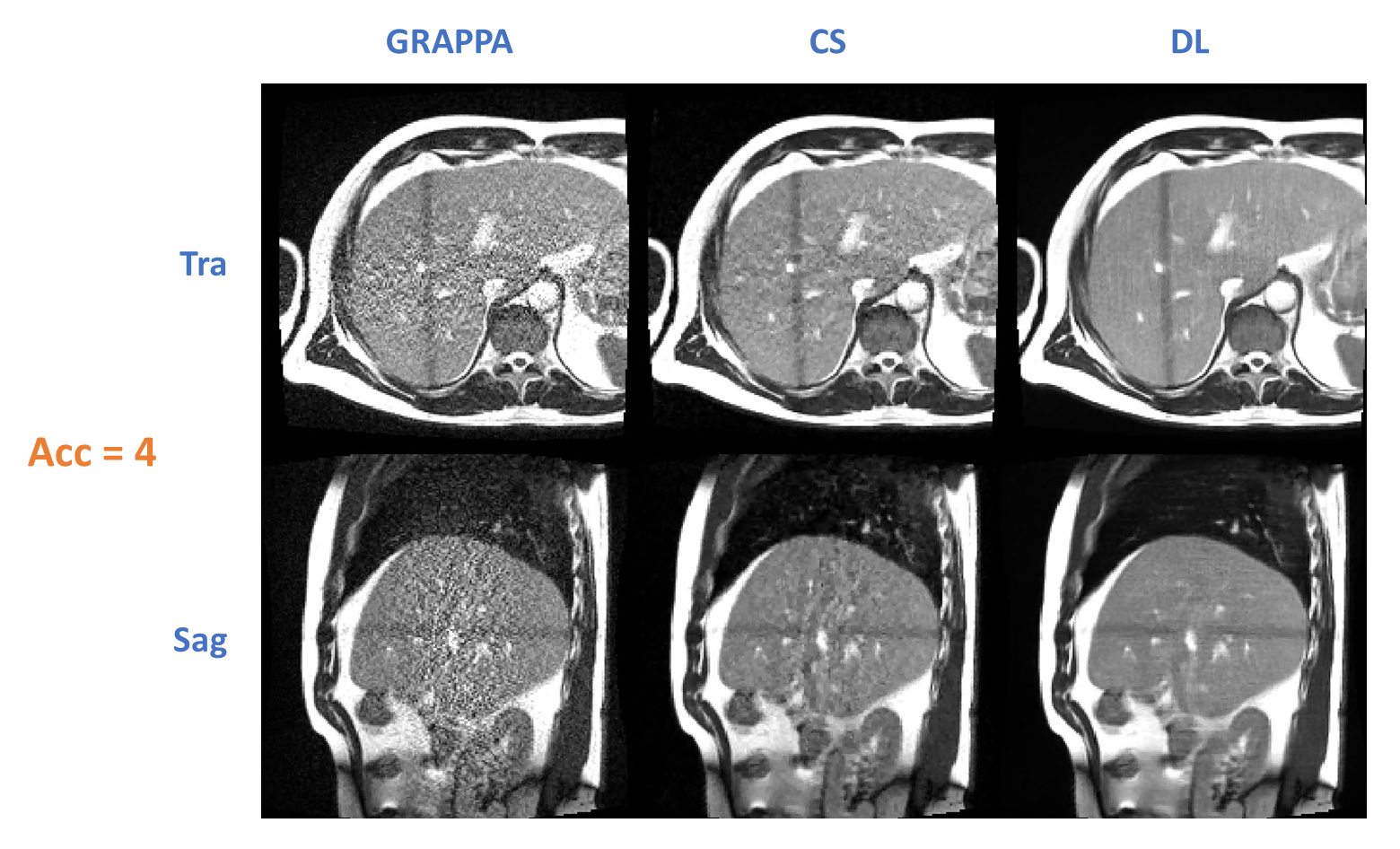
Figure 1 shows the setup of the phantom scan: biopsy needle was inserted into abdominal phantom which is partially covered by the body coil; in-room display supports visualization of real-time images during intervention. Figure 2 shows the images of biopsy phantom (with needle inserted) comparing among GRAPPA, CS, and DL for acceleration of 2, 3, and 4. Both CS and DL visually improved the image quality compared to GRAPPA, especially for acceleration factors 3 and 4. At acceleration factor 4, CS exhibited residual aliasing artifacts, which were further suppressed by DL. Figure 3 to 5 show the images acquired from a volunteer scan comparing among GRAPPA, CS, and DL for acceleration of 2, 3, and 4. DL showed lower artifact level, reduced noise, and improved delineation of the liver anatomy compared with CS and GRAPPA. Inference time of CS and DL reconstructions was approximately 80msec and 180msec per slice, respectively, and both shorter than the TR.DISCUSSION and CONCLUSION
In our study, we implemented DL image reconstruction to accelerate interactive real-time imaging at 0.55T, which achieved image quality that compared favorably with GRAPPA and CS. With additional acceleration enabled, the proposed method may mitigate the tradeoff among SNR, frame rate, spatial resolution, and slice thickness, and thereby has the potential to further empower 0.55T MRI as a viable interventional guidance platform.Acknowledgements
We thank Heinz-Werner Henke for providing the biopsy needle.References
[1] Campbell-Washburn AE, Ramasawmy R, Restivo MC, et al. Opportunities in Interventional and Diagnostic Imaging by Using High-Performance Low-Field-Strength MRI. Radiology. 2019;293(2):384-393. doi:10.1148/radiol.2019190452
[2] Arnold TC, Freeman CW, Litt B, Stein JM. Low‐field MRI: Clinical promise and challenges. Journal of magnetic resonance imaging. 2023;57(1):25-44. doi:10.1002/jmri.28408
[3] Hammernik K, Klatzer T, Kobler E, et al. Learning a variational network for reconstruction of accelerated MRI data. Magn Reson Med. 2018;79(6):3055-3071. doi:10.1002/mrm.26977
[4] Muckley MJ, Riemenschneider B, Radmanesh A, et al. Results of the 2020 fastMRI Challenge for Machine Learning MR Image Reconstruction. IEEE Trans Med Imaging. 2021;40(9):2306-2317. doi:10.1109/TMI.2021.3075856
[5] Liu J, Rapin JC, et al. Dynamic cardiac MRI reconstruction with weighted redundant Haar wavelets. ISMRM 2012: 4249.
[6] Herrmann J, Koerzdoerfer G, Nickel D, et al. Feasibility and Implementation of a Deep Learning MR Reconstruction for TSE Sequences in Musculoskeletal Imaging. Diagnostics (Basel). 2021;11(8):1484. doi:10.3390/diagnostics11081484
Figures