2716
Systematic Automated Evaluation of Needle Artifacts at 0.55 T, 1.5 T, and 3 T1Siemens Healthineers AG, Erlangen, Germany, 2Faculty of Physics and Astronomy, Ruprecht-Karls-Universität Heidelberg, Heidelberg, Germany
Synopsis
Keywords: MR-Guided Interventions, MR-Guided Interventions, 0.55T
Motivation: Numerous studies have investigated the appearance of MRI-compatible needles for interventional MRI. Needle artifacts were evaluated manually, which is a time-consuming process and prone to inter-reader deviations.
Goal(s): Our goal was to introduce an automated method for evaluating needle artifact diameter, aiming to simplify artifact assessment.
Approach: An automatic evaluation of needle artifacts was implemented and validated by conducting a systematic investigation of needle artifacts in a phantom study.
Results: A comprehensive chart of needle artifact diameter for various image parameters was generated automatically, serving as a tool for needle comparison. The results indicate excellent algorithm reliability.
Impact: The proposed tool allows for a systematic characterization of needle artifact size with high reliability and efficiency, which could be used to guide the correct choice of needle in different use cases (balance between artifact and lesion visibility)
Introduction
In MR-guided needle interventions, the passive needle artifact is used by the interventionalist for guidance. Knowledge of needle artifact size is essential, as it impacts the visually perceived needle size and needle‑to‑target‑distance. Numerous studies1,2 have explored the MRI appearance of MRI-compatible needles, focusing on factors such as sequence type and parameters, needle angle relative to the main magnetic field (B0), field strength, needle type, vendor-specific variations, and more. Traditionally, assessing the diameter of needle artifacts has heavily relied on manual measurements, which are time-consuming and prone to inter-reader deviations. In this work, we introduce an automated method for evaluating needle artifact diameter, aiming to simplify the assessment process and allow for consistent comparison of needles. Using the proposed automated evaluation, we conducted a systematic investigation of needle artifacts in MRI through a comprehensive phantom study, specifically at a field strength of 0.55T.Methods
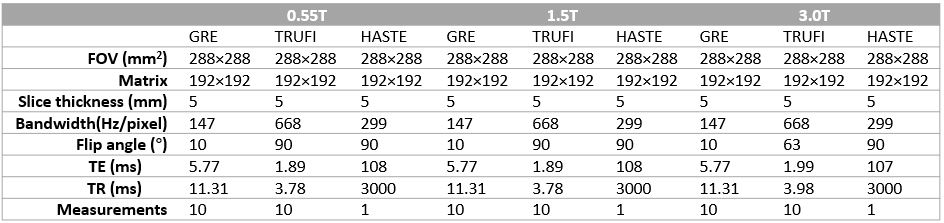
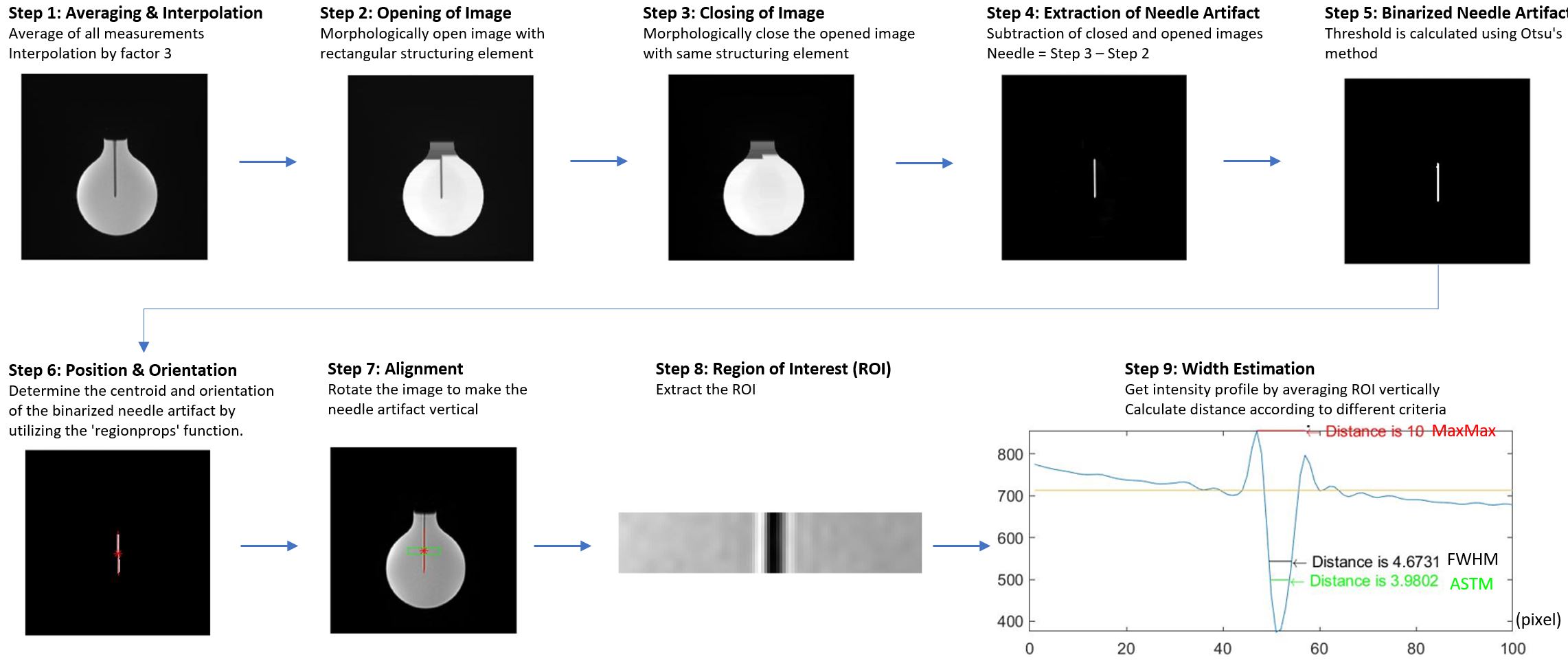
Figure 1 illustrates the phantom3 with a needle holder device. The study was performed using four different commercially available MRI-compatible needles (KIM puncture needles 16G, 20G; BIM biopsy needles 16G, 18G; ITP, Bochum, Germany) on three MR scanners (0.55T MAGNETOM Free.Max, 1.5T MAGNETOM Sola, 3.0T MAGNETOM Vida, Siemens Healthineers AG, Erlangen, Germany). The needle angles relative to B0 were set to 30°,60°, and 90°, and various real-time pulse sequences (GRE, TRUFI, HASTE) were employed with the frequency encoding direction both parallel and perpendicular to the needle. The protocol parameters were summarized in Table 1. They were maintained consistent across different field strength. To assess the robustness of the algorithm, each scan was repeated five times, with a small random in-plane field-of-view (FOV) shift for each repetition.Figure 2 depicts the proposed workflow for detecting and quantifying needle artifact. The automatic evaluation algorithm and data analysis were implemented in Matlab (The MathWorks, Inc., Natick, MA, USA). Multiple images were acquired using real-time sequences to achieve a dynamic steady state. The final measurements were utilized for evaluating the needle artifact diameter, whereas the entire set of measurements was averaged to aid in needle artifact detection and to determine the centroid and orientation of the needle artifact.
The artifact diameter was assessed using intensity profiles with three different criteria:
1) According to the American Society for Testing and Materials (ASTM) standards4, an artefact was defined as the region deviating ±30 % from the median signal intensity around the needle.
2) The full-width half-minimum (FWHM) of the intensity profile was used to determine the artifact diameter.
3) For HASTE images, when the frequency encoding axis was perpendicular to the needle, the intensity profiles were distorted. The inner (pure signal void) artifact was still calculated using ASTM and FWHM. Additionally, the outer (increased signal) artifact was determined as the distance between the two maxima (MaxMax) within the intensity profile5.
Results
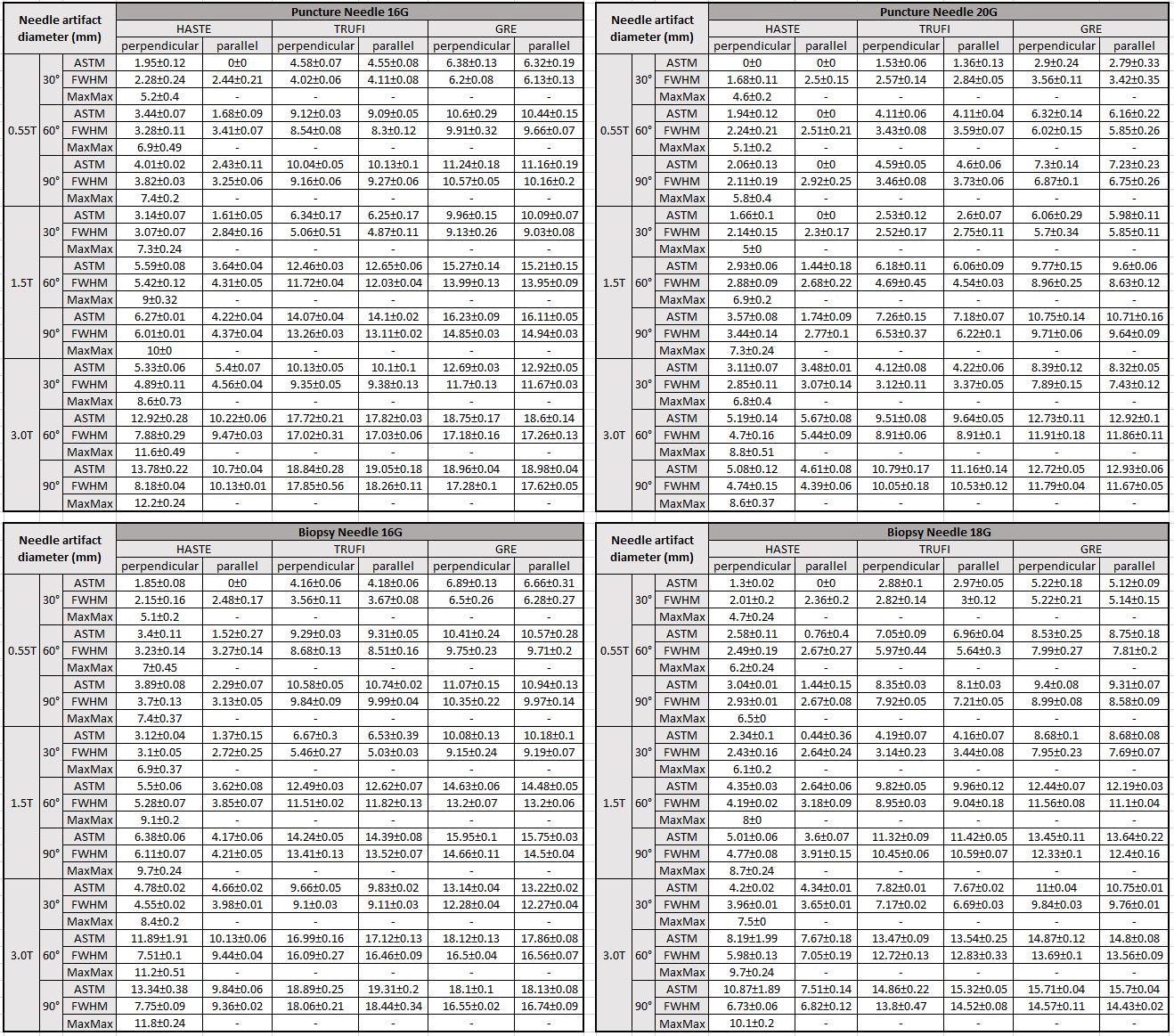
Table 2 presents the mean values and standard deviations of artifact diameters obtained from five repetitions. It shows a gradual reduction in artifact diameter as the field strength decreases, indicating a notable reduction in needle artifact at 0.55T. Additionally, there were observed distinctions in artifact diameters among various needle sizes (16G, 18G, and 20G), while showing the similarity between the 16G puncture needle and the 16G biopsy needle. Notably, as per ASTM criteria, certain artifact diameters are recorded as 0 in specific instances, particularly when using the HASTE sequence with frequency encoding parallel to the needle and a low needle angulation. However, when using FWHM, it consistently provides a value.Discussion
In this comprehensive phantom study, we have conducted 1080 measurements (216 configurations, 5 repetitions per configuration). The results indicate excellent algorithm reliability, as 99.4% of the calculated diameters show a deviation of less than 0.5 pixels.Needles were initially systematically tested at a 0.55T field strength, along with comparisons at 1.5T and 3T. The anticipated reduction in needle artifact at 0.55T was observed. This aids clinicians familiar with needle appearance at 1.5T and 3.0T systems in assessing the feasibility of using these needles at 0.55T.
In HASTE acquisitions with phase encoding in parallel to the needle axis, some ASTM results indicate a diameter of 0mm, since the signal reduction is below the ASTM threshold. However, characterization with the FWHM criterium was still feasible.
Conclusion
The proposed tool enabled a systematic assessment of needle artifact diameters using three criteria with high reliability and efficiency. Especially at a field strength of 0.55T, availability of literature data on artifact diameters for various needles is limited. Our automated artifact evaluation tool enables easy and fast needle characterization and, therefore, facilitates data collection on interventional devices at 0.55T.Acknowledgements
We thank Heinz-Werner Henke (ITP) for providing the needles.References
1.Penzkofer T., Peykan N., Schmidt K., et al. How MRI Compatible is ‘‘MRI Compatible’’? A Systematic Comparison of Artifacts Caused by Biopsy Needles at 3.0 and 1.5 T. Cardiovasc Intervent Radiol. 2013;36:1646-1657.
2.Schmidt V.F., Arnone F., Dietrich O., et al. Artifact reduction of coaxial needles in magnetic resonance imaging‑guided abdominal interventions at 1.5 T: a phantom study. Scientific Reports. 2021; 11:22963
3.Uhlig R. Deep Learning based Passive Needle Tracking for MR-Guided Percutaneous Interventions Optimized with Synthetic Data. Master’s Thesis, University of Erlangen, 2020.
4.ASTM Committee. Standard test method for evaluation of MR image artifacts from passive implants. 2013; F2119-07.
5.Ladd M.E., Erhart P., Debatin J.F., et al. Biopsy Needle Susceptibility Artifacts. MRM. 1996;36:646-651.
Figures