2713
Mild hyperthermia induced by MRgHIFU as an adjuvant to radiation therapy in bone metastases: preliminary results of a phase I study1University of Geneva, Faculty of Medicine, Geneva, Switzerland, 2Radio-oncology department, University Hospitals of Geneva, Geneva, Switzerland, 3Radiation Oncology, Oncology Institute of Southern Switzerland, Bellinzona, Switzerland, 4Radiology department, University Hospitals of Geneva, Geneva, Switzerland, 5University Hospitals of Geneva, Geneva, Switzerland
Synopsis
Keywords: MR-Guided Focused Ultrasound, Focused Ultrasound, Hyperthermia, focused ultrasound, bone metastasis
Motivation: Mild hyperthermia (HT) induced by magnetic resonance-guided focused ultrasound (MRgHIFU) before radiation therapy (RT) could act as adjuvant in pain relief for bone metastasis.
Goal(s): This study aims to evaluate the feasibility and safety of MRgHIFU procedure in one patient with a posterior right acetabulum
Approach: The target temperature elevation was 6°C. The targeting and temperature monitoring in near real-time were performed by MRI.
Results: The temperature elevation lasting 30-minutes was 6.01°C on average in bone metastasis. The MR-guidance allowed a safe and successful procedure without adverse events. The 25-minutes between HT end point and RT demonstrated the technical feasibility of the procedure.
Impact: This study is a first step to demonstrate MRgHIFU hyperthermia adjuvant to palliative radiotherapy of bone metastases. The non-invasive, safe and accurate use of focused ultrasound to sensitize tumors opens the way to more efficient application of the radiation dose.
Introduction
Radiation therapy (RT) is one of the most common palliative strategies in the treatment of bone metastases. Several studies have demonstrated that inducing hyperthermia before or after RT increases the effectiveness of the treatment. Hyperthermia can be produced by radiofrequency waves, microwaves, lasers, or high-intensity focused ultrasound (HIFU). HIFU has the advantage of being non-invasive and can be guided in real-time by magnetic resonance (MRgHIFU). We present the first case of a palliative treatment combining mild hyperthermia induced by MRgHIFU and external beam radiation therapy (EBRT) in bone metastases.Material and method
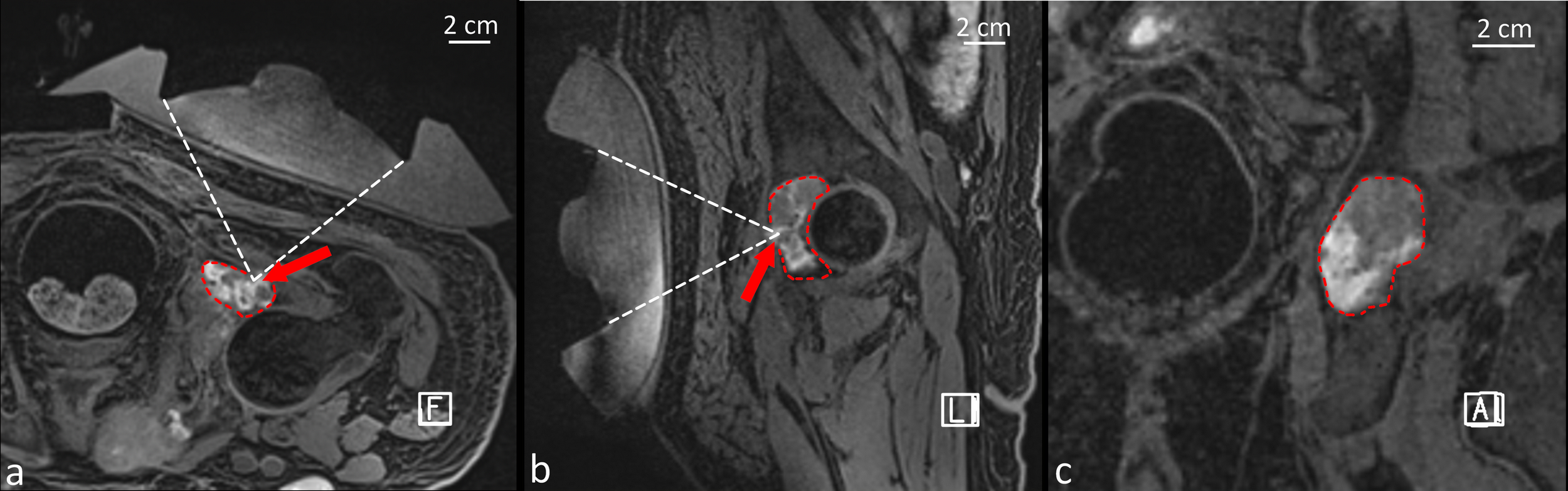
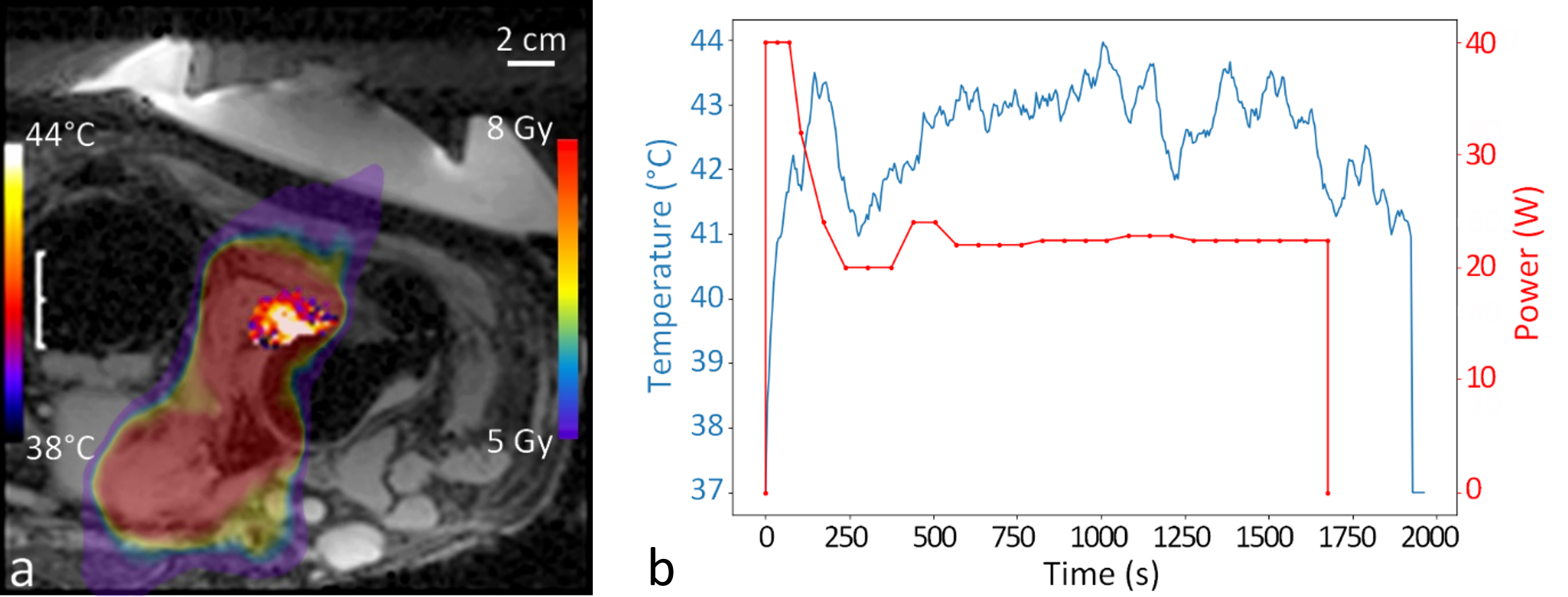
The trial was approved by the national regulatory authorities and is registered with clinicaltrials.gov. The patient signed a written consent. The patient was a 48-year-old man suffering from multimetastatic melanoma with mutated BRAF V600E and a multidisciplinary indication for a palliative course of EBRT. The patient presented a large lytic mass in posterior right acetabulum (4.8cm) associated with cortex discontinuity at 1.4cm of sciatic nerve and 6.4cm of the skin. Karnofsky score was calculated at 60. The patient lied in prone position on the MR table and the transducer was maintained posteriorly in contact with the skin using a mechanical holder. The patient came for simulation and targeting 5 days before the planned treatment to ensure the technical feasibility and intra-operatory compliance with the procedure. The simulation was used to plan the hyperthermia to save time on the day of the intervention and to guarantee the timeline for RT. Focused ultrasound was generated by an MR-compatible phased array transducer operating at 650kHz dedicated to mild hyperthermia (Imasonic, Voray-sur-l’Ognon, France). The natural focus of the transducer is formed at 10-cm depth by 104 hexagonal-shaped elements. The variable sizes and the asymmetric distribution of the element combined with the individual control of each element allow the displacement of the focus in a volume of 10 x 20 x 30mm around the natural focus without the occurrence of significant secondary lobes. The cooling and acoustic coupling were ensured by the circulation of approximately 1L of deionized and degassed water passing through a heat exchanger. Targeting was performed using a 3D high-resolution (HR) T1-weighted sequence acquired with a 12-element spine coil and a flexible 18-channel coil in a 3T MR scanner (Prisma Fit, Siemens, Erlangen, Germany). The parameters of this sequence were: FOV = 400 x 400mm2, TE = 1.32ms, TR = 6ms, spatial resolution = 1.25 x 1.25 x 1.3m3, flip angle = 10°, number of averages = 1. The temperature was monitored by the proton resonance frequency shift (PRFS) method using a GRE-EPI sequence in 3 crossing planes centered on the focus. The parameters of the thermometry sequence were: FOV = 256 x 256mm2, TE = 8.62ms, TR = 50ms, spatial resolution = 2 x 2 x 5m3, temporal resolution = 4.5s, flip angle = 15°, number of averages = 1. MR images were reconstructed in real-time and magnitude images were merged with temperature maps for near real-time temperature monitoring. At the end of the sonication, the T1-weighted MR sequence used for targeting was acquired again. The target temperature elevation for mild hyperthermia was 6°C for at least 30 minutes. The HIFU beam targeted the cortical break (Figure 1) to benefit from the acoustic oven effect [1], enhancing the spatial homogeneity of the temperature. The delivered power ranging 19-39W was manually adjusted by the interventional radiologist every 30 or 60 seconds with a 100% duty cycle. A moving 15-point average filter was applied during post-processing for noise reduction. For the radiation therapy, the planning target volume was delineated on a simulation scan and included the radiologically visible bone metastasis with a 7-mm isotropic margin. Just after the hyperthermia, the patient received a single 8 Gy fraction of palliative EBRT using a volumetric modulated arc therapy (VMAT) technique.Results
The simulation session lasted 120 minutes and the hyperthermia session lasted 90 minutes in total. The energy delivered in total was 105.6 kJ, for an average power of 22.5W and a sonication duration of 30 minutes and 54 seconds. The time interval between the end of the hyperthermia and the EBRT was 25 minutes. The technical feasibility and workflow were demonstrated in this first patient. No pain or adverse events were reported by the patient. The average temperature in the steady state after was 6.01°C ± 0.38°C over a region of 1.8 x 1.4 x 1.2 cm3.Conclusion
We report the first adjuvant hyperthermia induced by MRgHIFU before RT in one bone metastasis. The intervention was safe, successful and without adverse events which confirms its technical feasibility.Acknowledgements
No acknowledgement found.References
[1] Guillemin PC, Gui L, Lorton O, Zilli T, Crowe LA, Desgranges S, Montet X, Terraz S, Miralbell R, Salomir R, Boudabbous S. Mild hyperthermia by MR-guided focused ultrasound in an ex vivo model of osteolytic bone tumour: optimization of the spatio-temporal control of the delivered temperature. J Transl Med. 2019 Oct 24;17(1):350.Figures