2711
Correction of LIFU Intensity Using MR Acoustic Radiation Force Imaging (ARFI): Improved Correlations with Treatment Outcomes1University of Maryland School of Medicine, Baltimore, MD, United States
Synopsis
Keywords: MR-Guided Focused Ultrasound, Focused Ultrasound
Motivation: The effectiveness of low-intensity focused ultrasound (LIFU) for neuromodulation may be compromised by inaccuracies in target localization and variable energy deposition caused by skull characteristics.
Goal(s): We aimed to improve the estimation of LIFU pressure using MR-acoustic radiation force imaging (ARFI) and test whether the adjusted LIFU intensity correlates with treatment outcomes in a behavioral economic task using sucrose pellets.
Approach: Eight female rats underwent LIFU targeting the nucleus accumbens (NAc) bilaterally with three different pressures. MR-ARFI confirmed the targeting and corrected the intensities during LIFU treatments.
Results: Improved correlations between behavioral outcomes and ARFI-adjusted LIFU intensity were observed.
Impact: Our preliminary findings demonstrate the beneficial effects for using MRI-ARFI not only to verify the FUS target location but also to refine LIFU intensities in neuromodulation procedures.
INTRODUCTION
Low intensity focused ultrasound (LIFU) is an emerging technique that can non-invasively modulate deep brain regions1-3, and may become a useful adjunct therapy for various neuropsychiatric disorders4-6. However, variations in skull density, thickness, and shape, and variations in transducer placement can induce focused ultrasound (FUS) aberrations and ultimately cause inaccurate localization of the target focal point and attenuation in energy deposition7.MR acoustic radiation force imaging (ARFI)8-10 uses a bipolar gradient to detect microscopic movements caused by deposited ultrasound energy. ARFI is typically used to confirm the location of the focal point of a FUS beam, but the phase change induced also provides an estimate of the tissue displacement and ultimately the acoustic intensity delivered at the target.
Recent work showed that LIFU targeting the nucleus accumbens (NAc), the reward center of the brain, may reduce craving in individuals with substance use disorders5,6. This study aims to: 1) show how MR-ARFI can be used to calibrate the FUS intensity in LIFU experiments; 2) determine whether the adjusted FUS intensity correlates with LIFU treatment outcomes in a food reward rat model. We hypothesized that the MR-ARFI-adjusted FUS intensity will show better inverse correlation with the amount of food consumption after LIFU inhibition of bilateral NAc.
METHODS
Animal Model and Behavioral StudiesEight Sprague-Dawley rats (8-week-old females) were trained to stable behavior and tested in a behavioral economic task using sucrose pellets. The task employed increasing fixed ratio requirements across bins within a session. Lever presses and pellets earned were recorded for each bin.
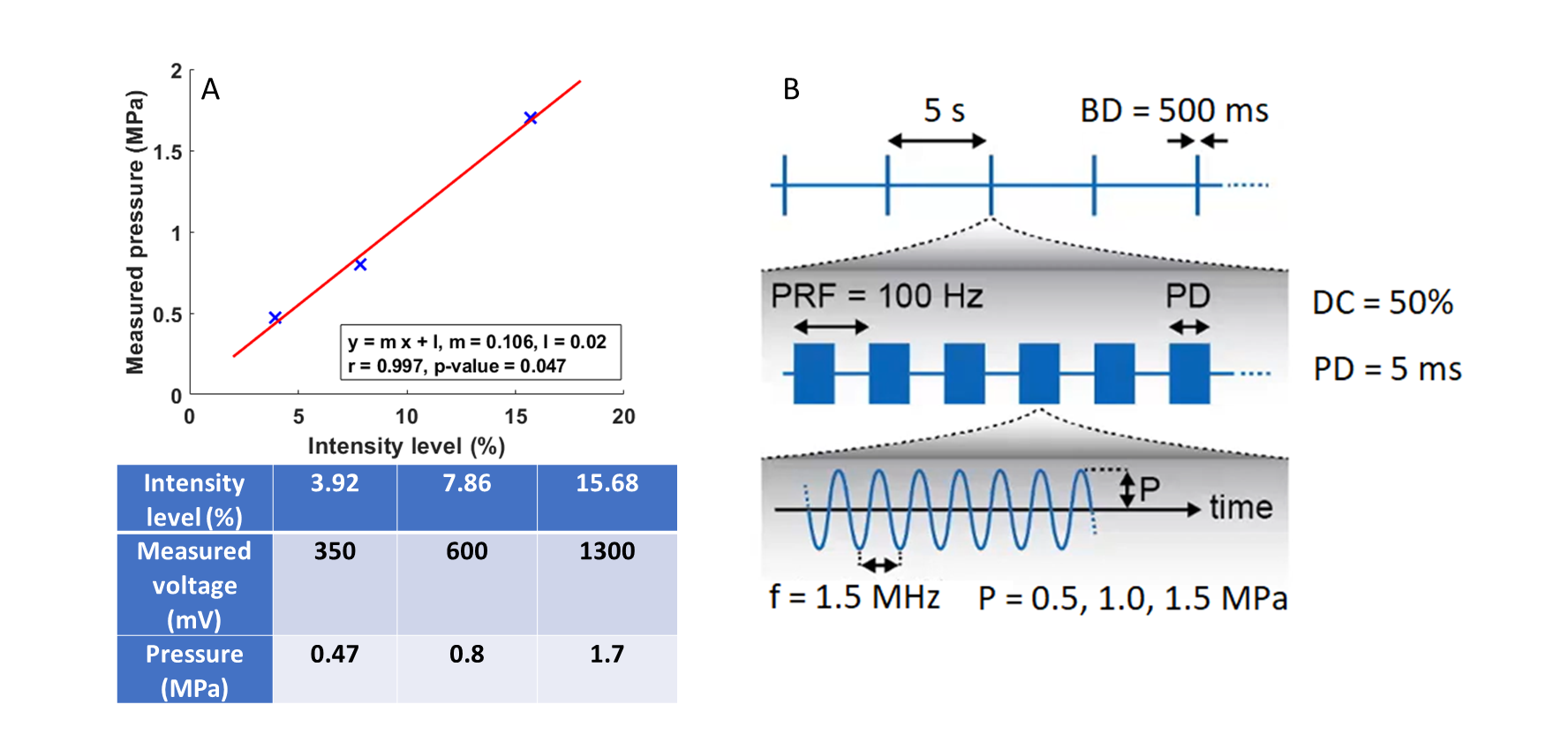
To suppress neural activity in the NAc, LIFU treatments targeting the NAc bilaterally were administered at pressures of 0.5, 1, or 1.5 MPa (calibrated in a phantom with a hydrophone, Figure 1A). The LIFU treatment scheme is illustrated in Figure 1B. On Day 1, 4 rats that were anesthetized for MRI-guided-ARFI-LIFU-treatments were each paired with another rat that had the same duration of anesthesia. On Day 2, one week later, those that had anesthesia only on Day 1 received the MR-guided-ARFI-LIFU, while those that received MRI-guided-ARFI-LIFU previously had anesthesia only. Food consumption measurements were conducted two hours after the MR-guided LIFU treatments or anesthesia only.
MR-Guided ARFI-LIFU
A 7T small animal MRI scanner (Bruker, Germany) equipped with an MR-compatible 1.5MHz MR-guided FUS system (Image Guided Therapy, Pessac, France) was used. This system has an 8-element annular array of FUS transducers and a single loop transmit-receive RF coil.
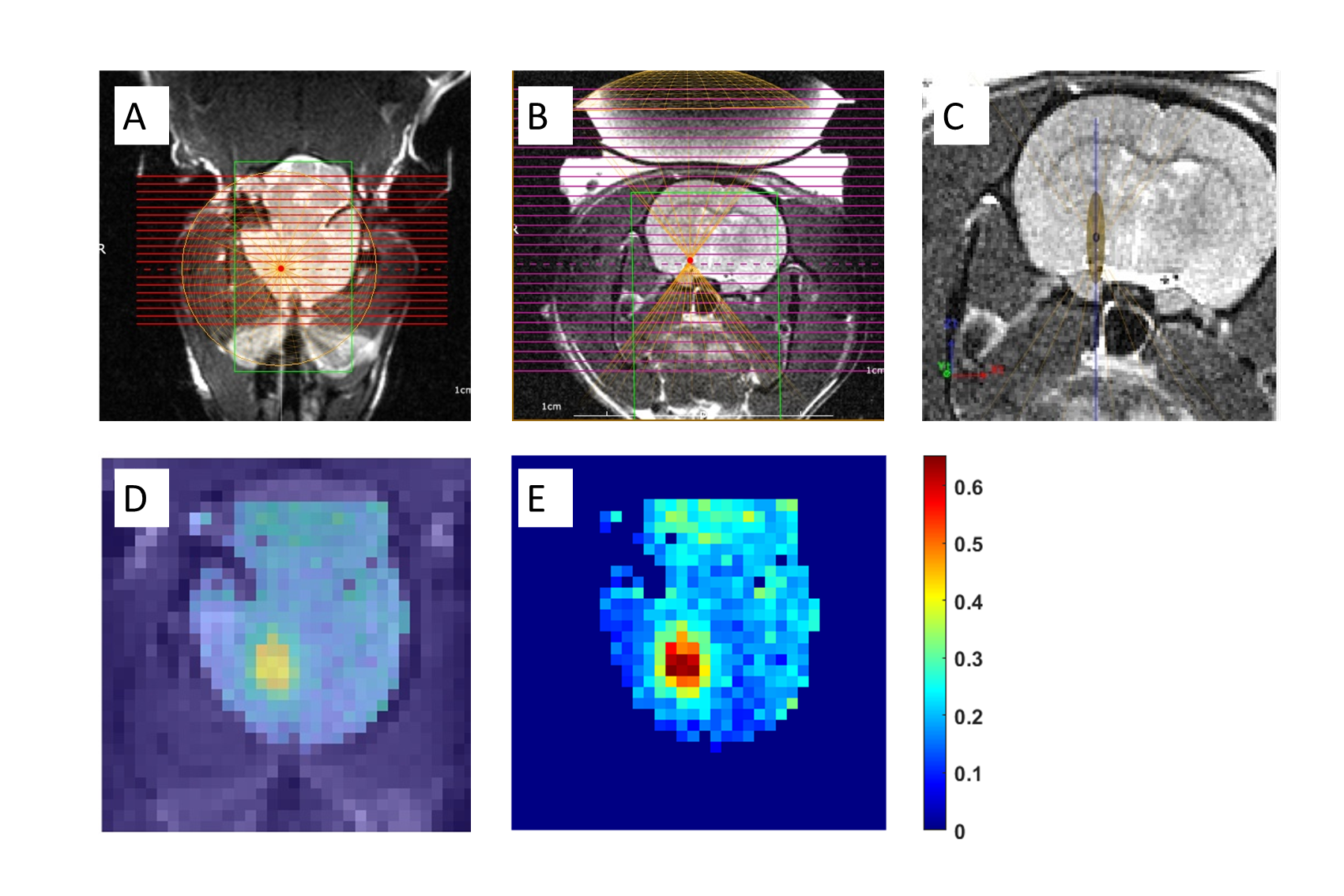
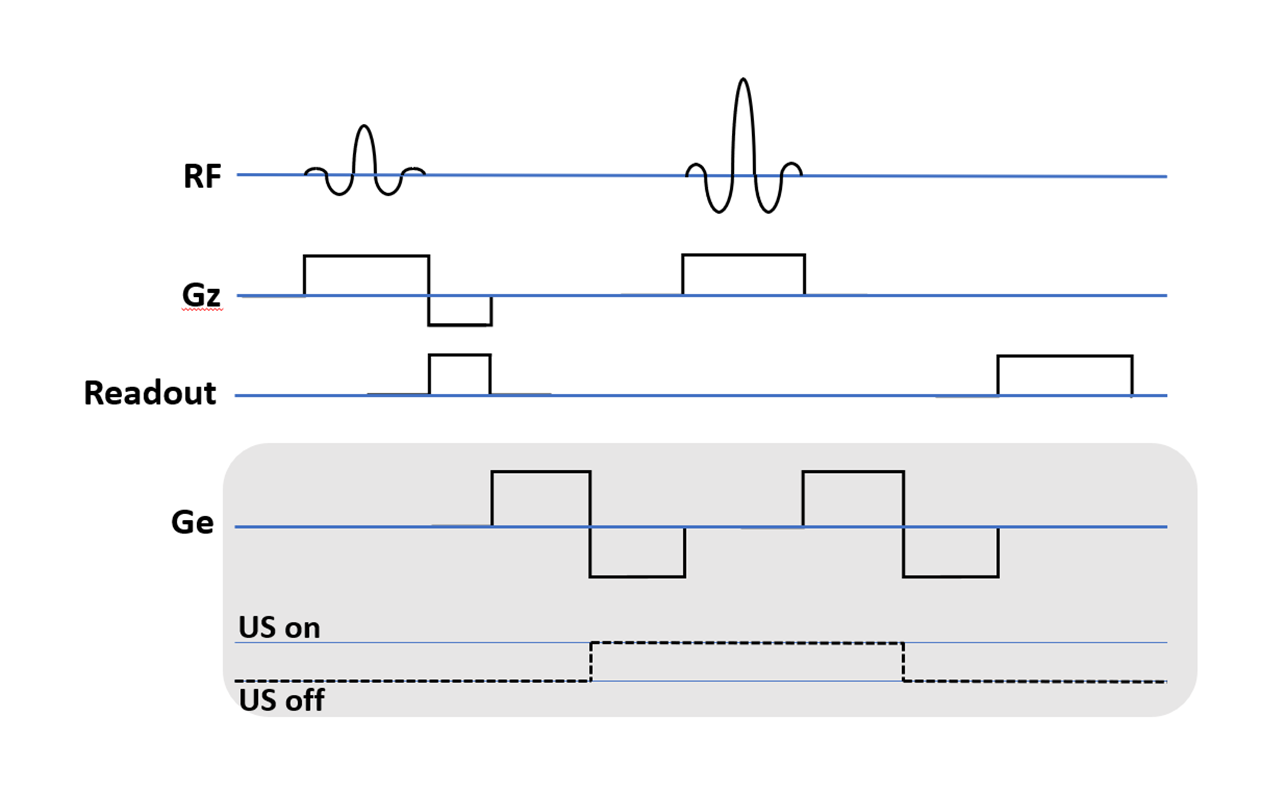
During the MR-ARFI-LIFU, T2-weighted axial and coronal MRI were performed to identify the target regions (Figure 2A-C). Next, MR-ARFI was performed at fixed power to validate the acoustic coupling and focal spot location in the brain (Figure 2D,E). The MR-ARFI sequence diagram and parameters, at fixed FUS power, are shown (Figure 3). Two sets of MRI-ARFI phase images were acquired, one with and one without sonication (reference phase image) and were subtracted to obtain the phase-encoded displacement.
Since the ARFI-FUS power was constant across animals, variations in the ARFI-derived displacement reflect experimental FUS-intensity variations at the focal point. The ARFI-derived displacement values were normalized across the 8 rats to yield $$$D_i$$$ (i=1:8), and used to calculate an adjusted LIFU intensity $$${L^a}_i$$$ for each animal:
$${L^a}_i=D_i{P^t}_i [1]$$
where $$${P^t}_i$$$ is the LIFU pressure set during treatment of the animal (0.5, 1, or 1.5MPa).
RESULTS
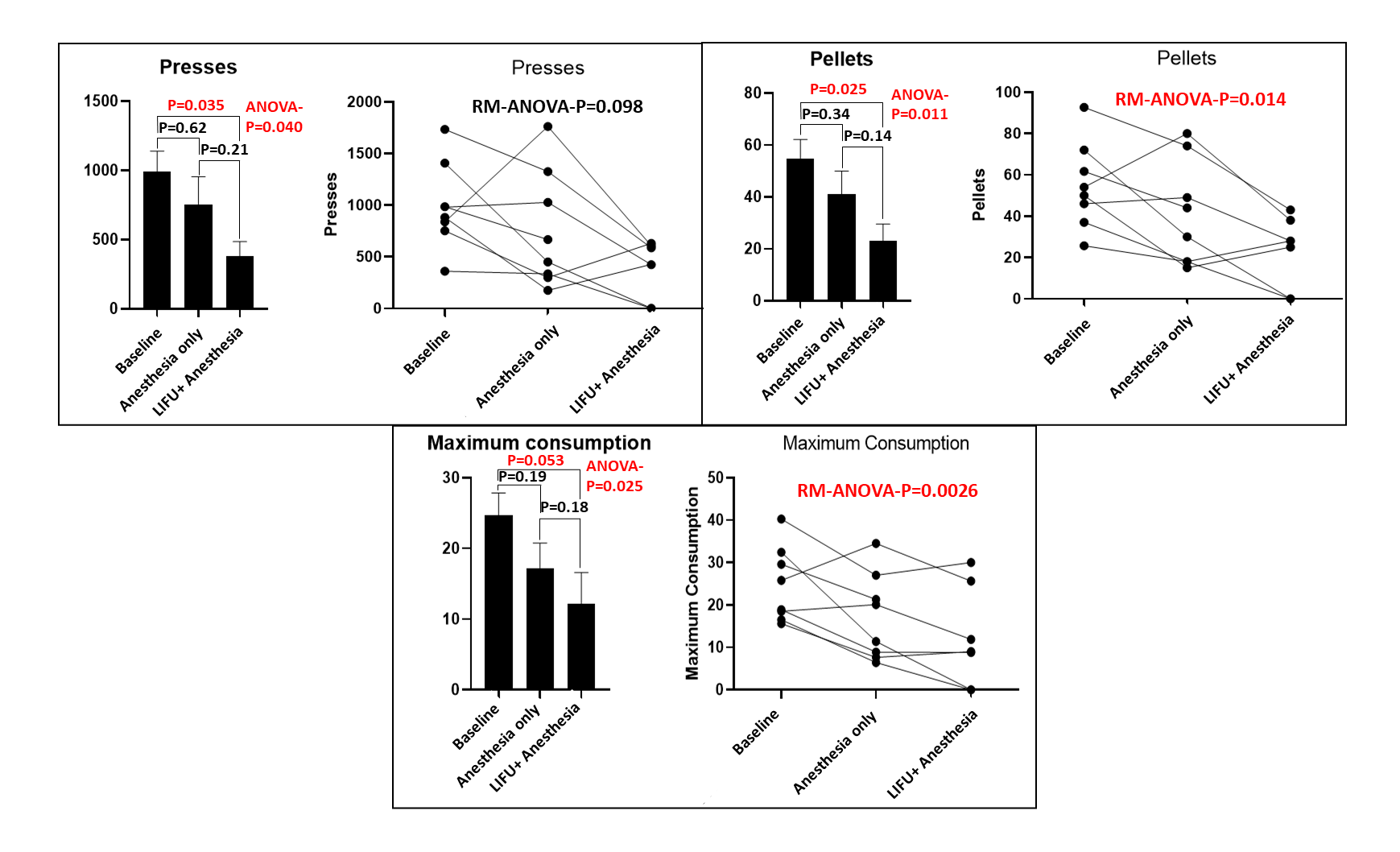
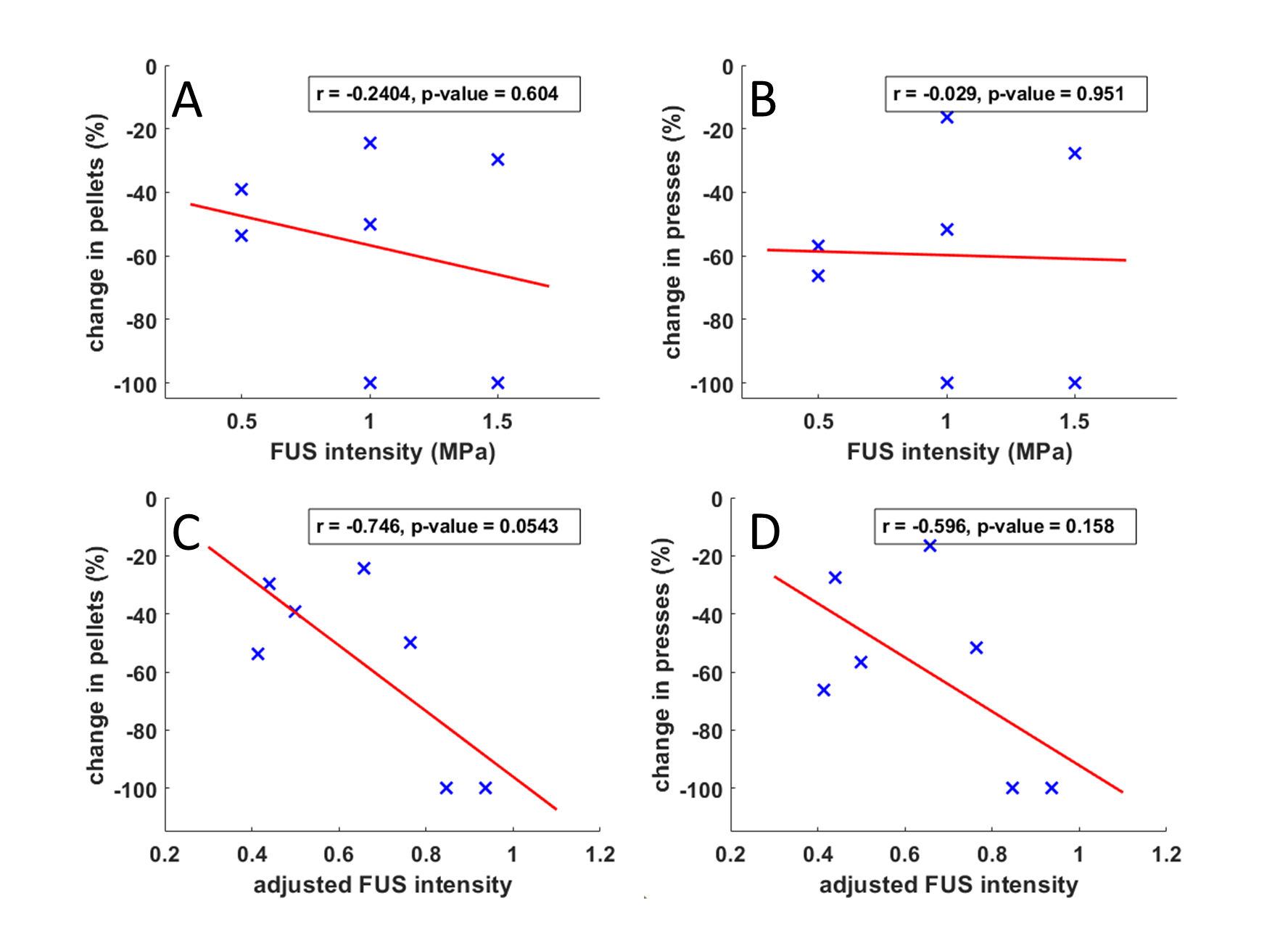
Across the three conditions, significant differences were observed with lever presses, pellets acquired, and maximum consumption (repeated-measure ANOVA-p<0.05). Post-hoc comparisons showed significantly lesser food consumption post-LIFU treatments (p<0.05), but not after anesthesia-only, relative to the baseline (Figure 4).Although ARFI was performed at the same FUS intensity, the measured displacement varied between 0.80 and 2.7 μm. No apparent correlation was found between the administered LIFU dosage and both treatment outcomes (Figure 5A,B). However, when using the adjusted LIFU intensity $$${L^a}_i$$$ (Eq.[1]), correlations emerged between the ARFI-estimated LIFU intensity and treatment outcomes (Figure 5C,D).
DISCUSSION
LIFU intensity measured with ARFI deviated substantially from intended values. We found improved correlations between behavioral outcome measures with the corrected acoustic pressure determined using ARFI. These preliminary findings suggest NAc LIFU reduces food motivation, while residual effects of anesthesia at 2 hours post treatment cannot be ruled out. Limitations include: 1) lack of a control group receiving sham LIFU treatments or LIFU in an active control brain region unrelated to reward-seeking behavior; 2) Further work will determine the recovery period required to normalize the behavior after ARFI-LIFU treatments.CONCLUSION
This study highlights the benefits of using ARFI not only to verify the FUS target location, but also to refine the accuracy of LIFU intensities in neuromodulation procedures.Acknowledgements
This work was supported by grants from the Focus Ultrasound Foundation Grant (to L.C.) and the National Institute on Drug Abuse (DP1DA053719 to L.C.)References
- Arulpragasam AR, van't Wout-Frank M, Barredo J, et al. Low intensity focused ultrasound for non-invasive and reversible deep brain neuromodulation—a paradigm shift in psychiatric research. Front Psychol. 2022;13:825802.
- Folloni D, Verhagen L, Mars RB, et al. Manipulation of subcortical and deep cortical activity in the primate brain using transcranial focused ultrasound stimulation. Neuron. 2019;101(6):1109-1116.
- Yüksel MM, Sun S, Latchoumane C, et al. Low-intensity focused ultrasound neuromodulation for stroke recovery: A novel deep brain stimulation approach for neurorehabilitation?. IEEE OJEMB. 2023.
- Krishna V, Sammatino F, Rezai A. A Review of the Current Therapies, Challenges, and Future Directions of Transcranial Focused Ultrasound Technology: Advances in Diagnosis and Treatment. JAMA Neurol. 2018;75(2):246-254.
- Mahoney JJ, Thompson-Lake DG, Ranjan M, et al. Low-Intensity Focused Ultrasound Targeting the Bilateral Nucleus Accumbens as a Potential Treatment for Substance Use Disorder: A First-in-Human Report. Biol Psychiatry. 2023;94(11):e41-43.
- Mahoney J, Haut MW, Carpenter J, et al. Low-intensity focused ultrasound targeting the nucleus accumbens as a potential treatment for substance use disorder: safety and feasibility clinical trial. Front Psychol. 2023;14:1211566.
- Kyriakou A, Neufeld E, Werner B, et al. A review of numerical and experimental compensation techniques for skull-induced phase aberrations in transcranial focused ultrasound. Int J Hyperth. 2014;30(1):36-46.
- Larrat B, Pernot M, Aubry JF, et al. MR-guided transcranial brain HIFU in small animal models. Phys Med Biol. 2009;55(2):365-388.
- Chen J, Watkins R, Pauly KB. Optimization of encoding gradients for MR‐ARFI. Magn Reason Med. 2010;63(4):1050-1058.
- Gaur P, Casey KM, Kubanek J, et al. Histologic safety of transcranial focused ultrasound neuromodulation and magnetic resonance acoustic radiation force imaging in rhesus macaques and sheep. Brain Stimul. 2020;13(3):804-814.
Figures