2709
MRI-guided histotripsy targeting using MR-thermometry and MR-ARFI1University of Michigan, Ann Arbor, MI, United States, 2Brigham Young University, Provo, UT, United States
Synopsis
Keywords: MR-Guided Focused Ultrasound, MR-Guided Interventions, Focused Ultrasound, Histotripsy
Motivation: Transcranial histotripsy requires pre-therapy targeting to ensure treatment at the intended region of interest. MR-ARFI and MR-Thermometry are used for targeting HIFU treatments, but are not tested for targeting of transcranial histotripsy treatments since they use different ultrasound treatment parameters.
Goal(s): We evaluate the accuracy of MR-thermometry and MR-ARFI for targeting histotripsy treatments in ex-vivo tissues.
Approach: Low intensity MR-thermometry and MR-ARFI were done prior to histotripsy treatment on bovine brain tissues. The lesion location was compared with the peak temperature/displacement to quantify targeting error.
Results: Both MR-thermometry and MR-ARFI can perform accurate targeting of histotripsy treatments with mean errors of 2mm.
Impact: Transcranial histotripsy is a promising non-invasive treatment method that requires pre-treatment targeting to ensure treatment delivery at the desired location. We showed that both low temperature MR-thermometry and MR-ARFI can be used to accurately estimate histotripsy treatment location.
Introduction
Histotripsy is a non-invasive, focus ultrasound (FUS) treatment method that uses ultrasound cavitation to mechanically destroy soft tissues [1]. It has shown potential in treating a variety of tissue types and is FDA-approved for treating liver tumors. Transcranial MRI-guided histotripsy (tcMRgHt) has been investigated to treat the ex-vivo and in-vivo brain tissues, without causing significant skull heating [2,3]. Precise pre-treatment targeting is important to retain high treatment accuracy. MR-thermometry and MR-acoustic radiation force imaging (MR-ARFI) have been used in pre-treatment targeting for high-intensity focused ultrasound (HIFU) thermal therapy [4]. In this work, we will examine and compare the accuracy of using MR-thermometry [4,6] and MR-ARFI [5] for pre-treatment targeting for histotripsy in ex-vivo bovine brain tissue. MR-thermometry, MR-ARFI, and HIFU thermal therapy use long ultrasound pulses (millisecond-length or longer) at low-mid ultrasound pressure with linear ultrasound propagation. In comparison, histotripsy uses microsecond-length pulses at very high ultrasound pressure with nonlinear propagation. Therefore, using MR-thermometry and MR-ARFI for pre-treatment targeting requires modification of the ultrasound source and examines the targeting inaccuracy that may be induced by nonlinear ultrasound propagation.Methods
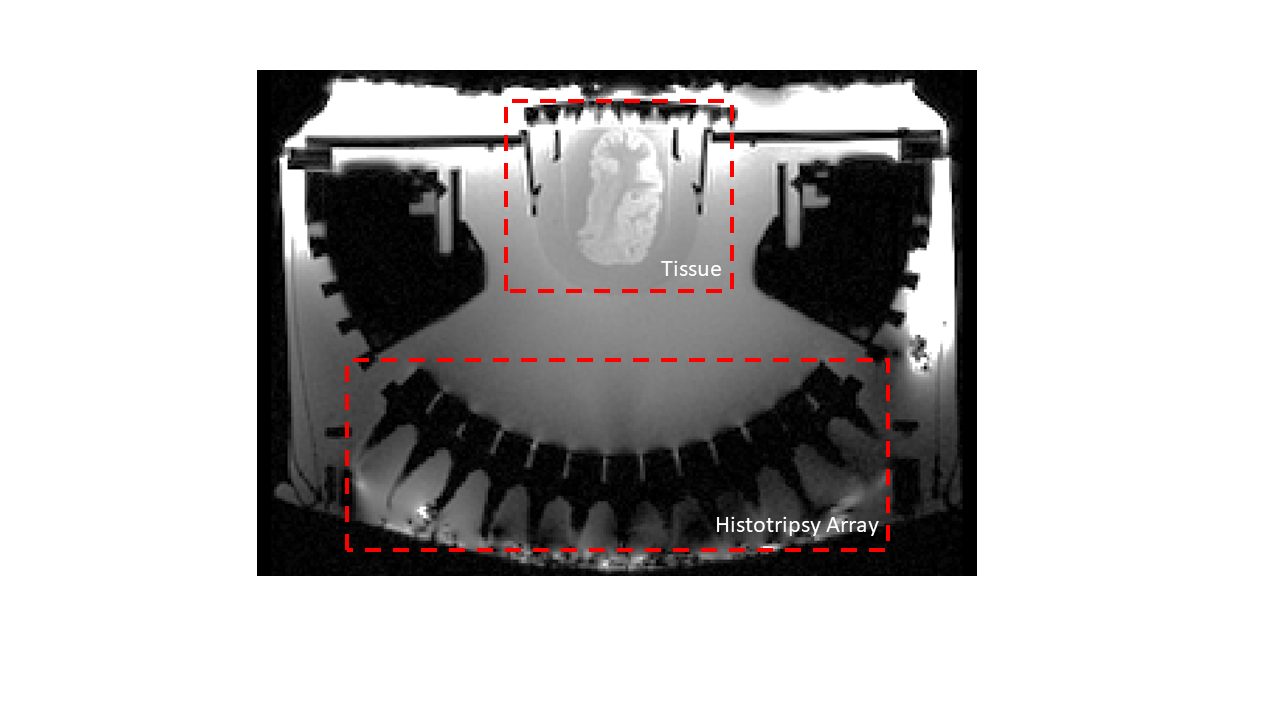
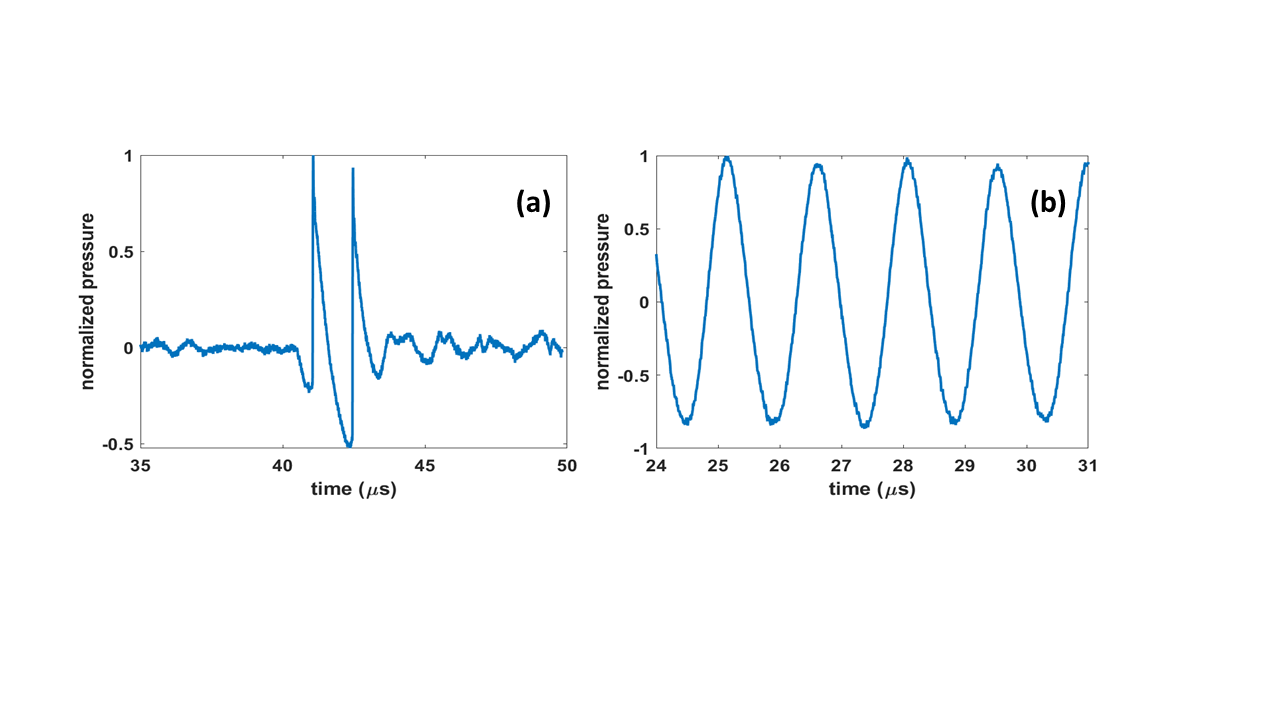
All experiments used a 700 kHz, 128-element MR-compatible histotripsy array (f-number:0.73, FWHM:2x2x7mm3, Figure 1) to treat ex-vivo bovine brains. The array was placed in a 3T human MRI scanner (GE UHP scanner), and 21-channel GE AIR coils were used for receiving MR signals. For each tissue sample, pre-treatment MR-Thermometry and MR-ARFI images were acquired. Then, a volume histotripsy lesion was generated centered at the array focus which was visualized on diffusion-weighted images (DWI). Targeting accuracy was measured by the difference between the centroid of the pre-treatment MR-thermometry/MR-ARFI image and the centroid of the histotripsy lesion on post-treatment DWI. Low-temperature heating, acoustic radiation force, and histotripsy pulses were produced using the same ultrasound transducer and driver. For MR-thermometry/MR-ARFI, a continuous wave (100% duty cycle) of 30s/20ms was used with a peak negative pressure of ~4-5 MPa (Figure 2). Proton resonance frequency MR-thermometry was performed using a 3D RF-spoiled gradient recalled echo (GRE) scan. The scan parameters were TE/TR: 33ms/39ms and the temporal resolution was 4.68 seconds. MR-ARFI scan was done using a spin-echo pulse sequence, with a pair of bipolar gradients of area 24 G·ms/cm along the array’s longitudinal axis on either side of the rephasor pulse (US on time: 20ms/TR). The scan parameters were TE/TR:38ms/500ms with 1-minute/ARFI-image. Both MR-thermometry and MR-ARFI used a 15-stack of spirals acquisition with FOV:40x40x4.5cm, matrix:256x256x15. B0 informed CG-SENSE was used for reconstructing images for both methods using a field map and sensitivity map acquired from a separate scan. Histotripsy was applied using 1.5 cycle pulses at an estimated peak negative pressure of 120MPa, <0.1% duty cycle, and 0.5x0.5x5mm spacing with a 10x10x5 treatment point grid. Histotripsy-generated lesions were imaged using a DWI scan (b=0,1000s/mm2) with echo-planar imaging (EPI) readout. FSL toolbox’s topup was used for distortion correction by using two scans with opposite phase encoding directions.Results
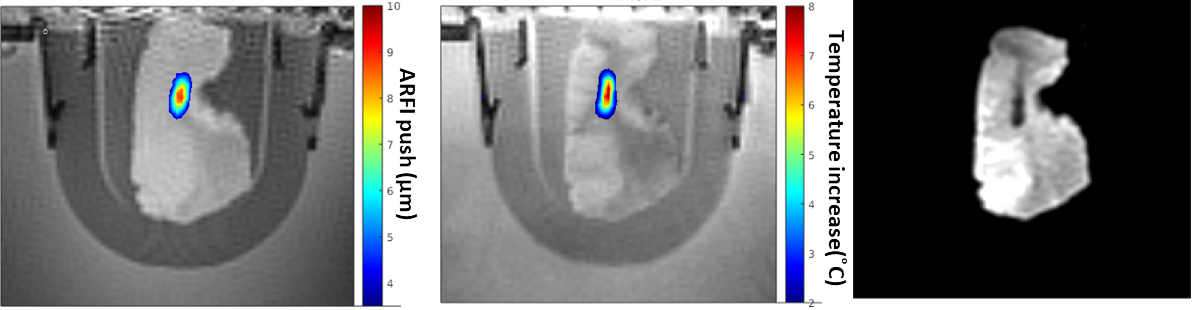
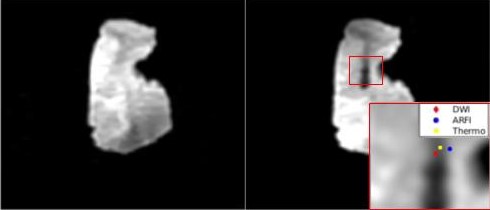
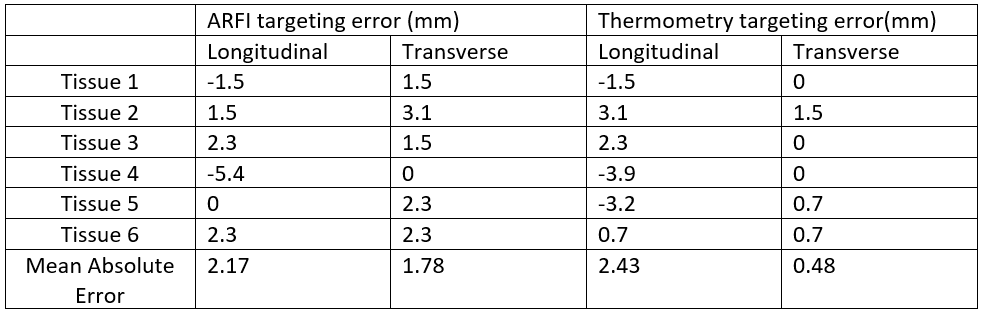
The ultrasound focus was visualized on all MR-thermometry, MR-ARFI, and DWI images (Figure 3). Both MR-thermometry and MR-ARFI displayed a well-confined focal region. The mean targeting error for MR-ARFI/MR-thermometry was 1.78/0.48mm in the transverse axis and 2.17/2.43mm in the longitudinal axis (Figure 4, Table 1). Since the FWHM of the array is elongated along the longitudinal axis, the lesions appeared stretched along that dimension, making it harder to estimate the histotripsy focus.Discussion and Conclusion
This work explores using MR-ARFI and MR-thermometry for pre-treatment targeting of histotripsy in ex-vivo bovine brain tissue. The mean error in the estimated focus for both methods was approximately 2 mm of the histotripsy focus. Since the histotripsy focus is longer in the longitudinal axis due to the low f-number, estimating the focus in that axis is harder and prone to larger errors.Acknowledgements
This work is supported by NIH grant R01EB028309.References
[1] Xu Z, Ludomirsky A, Eun LY, Hall TL, Tran BC, Fowlkes JB, et al. Controlled ultrasound tissue erosion. IEEE Trans Ultrason Ferroelectr Freq Control 2004;51:726–36. https://doi.org/10.1109/tuffc.2004.1304271.
[2] Gerhardson T, Sukovich JR, Pandey AS, Hall TL, Cain CA, Xu Z. Catheter Hydrophone Aberration Correction for Transcranial Histotripsy Treatment of Intracerebral Hemorrhage: Proof-of-Concept. IEEE Trans Ultrason Ferroelectr Freq Control 2017;64:1684–97. https://doi.org/10.1109/TUFFC.2017.2748050.
[3] Lu N, Gupta D, Daou BJ, Fox A, Choi D, Sukovich JR, et al. Transcranial Magnetic Resonance-Guided Histotripsy for Brain Surgery: Pre-clinical Investigation. Ultrasound Med Biol 2022;48:98–110. https://doi.org/10.1016/j.ultrasmedbio.2021.09.008.
[4] Rieke V, Pauly KB. MR thermometry. Journal of Magnetic Resonance Imaging 2008;27:376–90. https://doi.org/10.1002/jmri.21265.
[5] de Bever JT, Odéen H, Hofstetter LW, Parker DL. Simultaneous MR thermometry and acoustic radiation force imaging using interleaved acquisition. Magn Reson Med 2018;79:1515–24. https://doi.org/10.1002/mrm.26827.
[6] Holbrook AB, Santos JM, Kaye E, Rieke V, Pauly KB. Real-time MR thermometry for monitoring HIFU ablations of the liver. Magn Reson Med 2010;63:365–73. https://doi.org/10.1002/mrm.22206.
Figures