2708
Cardiac MR-thermometry with integrated catheter drift detection for guidance of ventricular tachycardia ablation1King's College London, London, United Kingdom, 2MR Research Collaborations, Siemens Healthcare Limited, Camberley, United Kingdom, 3MR Physics, Guy’s and St.Thomas’ NHS Foundation Trust, London, United Kingdom, 4School of Engineering, Pontificia Universidad Católica de Chile, Santiago, Chile, 5Institute for Biological and Medical Engineering, Pontificia Universidad Católica de Chile, Santiago, Chile
Synopsis
Keywords: MR-Guided Interventions, Interventional Devices, Active Tracking
Motivation: MR-thermometry is a promising approach for real-time monitoring of lesion formation during MRI-guided cardiac ablation. However, ablation catheters can potentially drift during ablation and lead to inaccurate lesion formation.
Goal(s): To develop a cardiac MR-thermometry sequence with integrated catheter drift detection.
Approach: Continuous active tracking modules were added between the cardiac triggered acquisitions of a cardiac MR-thermometry sequence. Low-pass temporal filtering of the active tracking signal was then applied to remove cardiac and respiratory components and estimate catheter drift. This approach was evaluated in a phantom.
Results: This study showed that catheter drift detection is possible within active tracking in an MR-thermometry sequence.
Impact: This study demonstrates the potential for simultaneous catheter drift detection and cardiac MR-thermometry, which may improve the safety of the procedure and the accuracy of lesion formation. Further evaluation in-vivo is now warranted.
Introduction
Real-time MR-thermometry shows promise for the guidance of cardiac ablation procedures1,2. Active ablation catheters, containing tracking coils, are currently used for these procedures3. During ablation in the heart, the catheter location is subject to cardiac and respiratory motion and can potentially move/drift during the procedure, resulting in inaccurate lesion formations. Very few studies have investigated the impact of catheter drift4, which is difficult to identify during cardiac MR-thermometry. In this study, we sought to develop a catheter drift detection technique within a cardiac MR-thermometry sequence for real-time simultaneous assessment of catheter drift and lesion formation.Methods
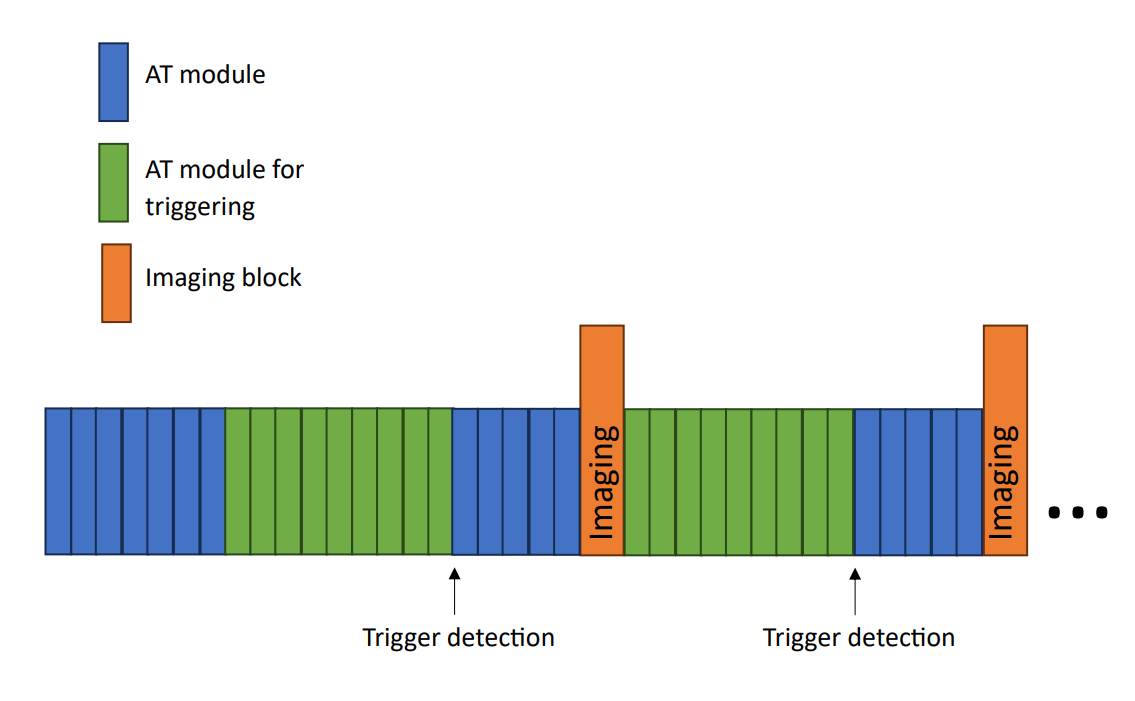
Proposed approachA continuous acquisition of active tracking (AT) modules was added to a cardiac EPI MR-thermometry sequence, as previously demonstrated5 and shown in Figure 1. This allows AT modules to be acquired repeatedly at a sampling rate of 24ms (42Hz) to measure the catheter position. The temporal evolution of the AT signal was used for two purposes. First, it was employed to detect a robust cardiac trigger for the MR-thermometry acquisition using band-pass filtering to isolate the cardiac motion component of the temporal AT signal (minimum frequency of 0.67Hz and maximum frequency of 2.5Hz), as previously demonstrated5. Second, low-pass filtering of the temporal AT signal was applied to remove both cardiac and respiratory motion components and to isolate the potential catheter drift. This was done using a lowpass finite impulse response filter, designed in MATLAB (v2021a, The MathWorks, Nantucket, MI) with a cutoff frequency of 0.05Hz and filter order of 400.
Experimental evaluation
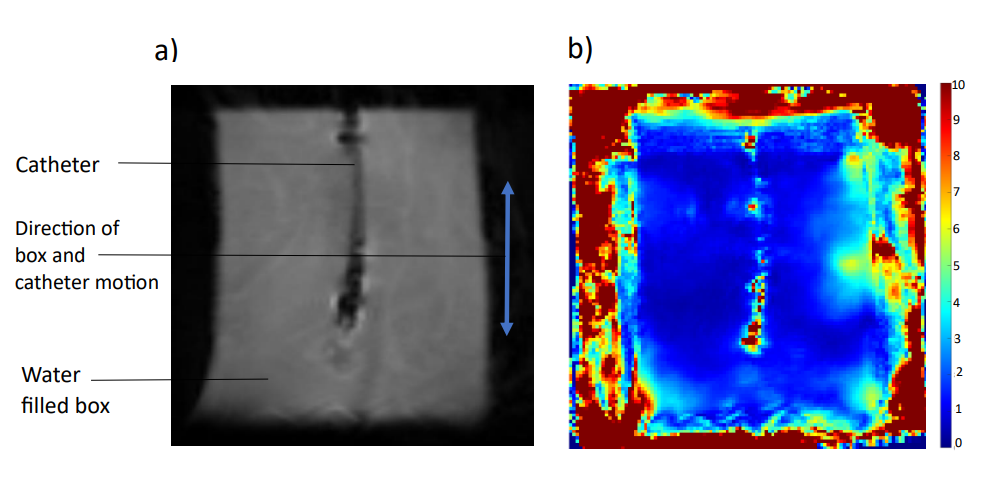
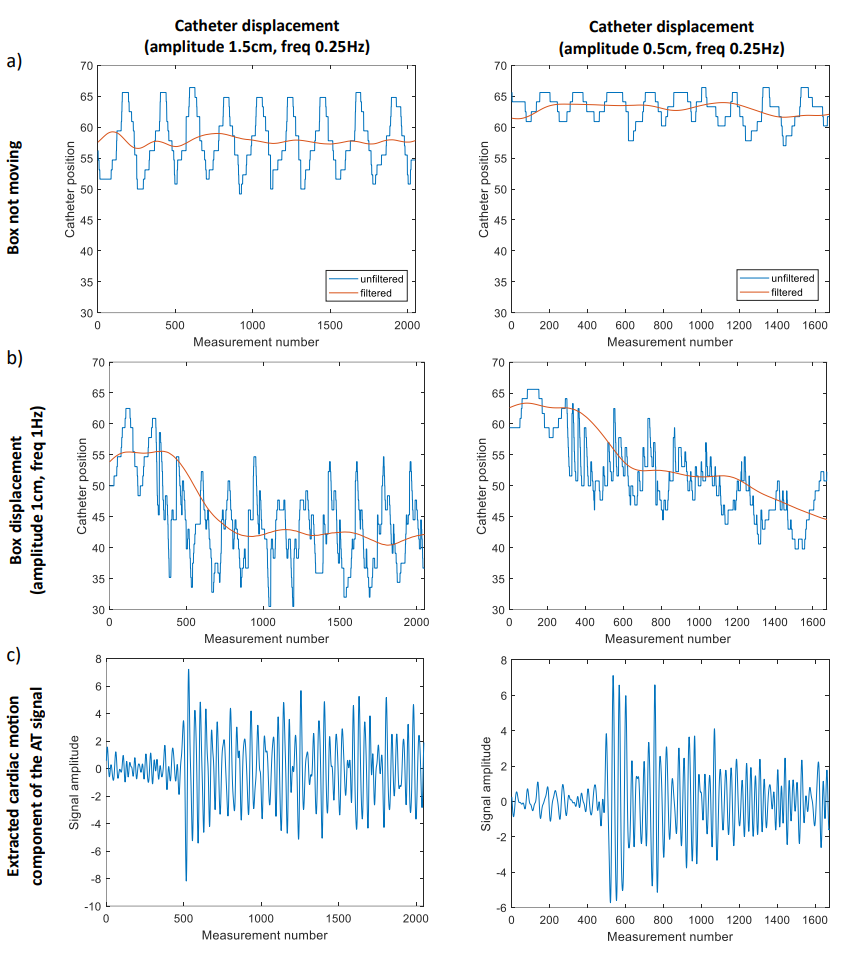
All experiments were performed on a 1.5T scanner (MAGNETOM Aera, Siemens Healthcare, Erlangen Germany). The proposed approach was evaluated in a phantom which was built for these experiments and consisted of a plastic tube with a closed end which was fixed to the bottom of a container filled with water. The catheter (Vision-MR Ablation Catheter, Imricor Medical Systems, Burnsville, MN) was inserted into the tube which restricted its movement to the foot-head direction. The closed end of the tube also ensured that the catheter was returned to the same position after each movement. This phantom set up allowed the catheter to be moved independently from the box. The frequencies at which the catheter and box were moved by were approximated by displacing them continuously by hand in the scanner by a set distance in a known time period. In this study, the catheter was moved at 0.25Hz with an amplitude of 0.5cm (setup #1) and 1.5cm (setup #2) to represent the breathing motion. The box was kept still for the first 20 seconds of each experiment. After that, a permanent foot-head drift combined with a periodic continuous foot-head displacement of 1cm at 1Hz to simulate the cardiac motion was manually applied to the box. Control experiments where the box was stationary for the entire duration of the scan were also carried out.
Results
Figure 2 shows an example of a magnitude image and associated temperature map obtained during the experiments. Figure 3 shows the AT signal acquired during the experiments when the catheter was moved with an amplitude of 1.5cm and 0.5cm (on left and right of Figure3b respectively), together with the corresponding low-filtered signal representing the drift contribution. In both experiments, a drift can be easily identified on the low-pass filtered signals. The cardiac component of the AT signal used for cardiac triggering was also depicted for both experiments (Figure 3c) where noise like signal is observed during the first 20s and is then followed by periodic displacement when the box starts moving to replicate cardiac motion.Discussion
Catheter drift detection within an MR-thermometry sequence is possible and was successfully demonstrated in phantom experiments. Its in-vivo feasibility and accuracy during an ablation remains to be investigated. In this simulated environment, the drift was only detected in one orientation as the cardiac and respiratory motion were both applied in the foot-head direction. Filtering on a composite metric representing the 3D displacement5 may therefore be needed in vivo where catheter drift may occur in any dimension. Additionally, there is a delay that is induced by the filter which may cause a latency in detecting the catheter drift in real time and could be compensated with more advanced filtering strategies.Conclusion
The proposed MR-thermometry approach shows promise for simultaneous lesion assessment and detection of the catheter drift in the presence of respiratory and cardiac motion. Further studies evaluating the in vivo capabilities of this technique are now warranted.Acknowledgements
This work was supported by the Innovate UK grant (68539), the Engineering and Physical Sciences Research Council (EPSRC) grant (EP/R010935/1), the British Heart foundation (BHF) grants (PG/19/11/34243 and PG/21/10539), the Wellcome EPSRC Centre for Medical Engineering at Kings College London (WT 203148/Z/16/Z), the National Institute for Health Research (NIHR) Biomedical Research Centre based at Guy’s and St Thomas’ NHS Foundation Trust and King’s College London. The views expressed are those of the authors and not necessarily those of the NHS, the NIHR or the Department of Health.References
1. Denis de Senneville B, Roujol S, Jais P, Moonen C, Herigault G and Quesson B. Feasibility of fast MR-thermometry during cardiac radiofrequency ablation. NMR Biomed (2012) 25:556-62
2. Toupin S, Bour P, Lepetit-Coiffe M, Ozenne V, Denis de Senneville B, Schneider R et al. Feasibility of real-time MR thermal dose mapping for predicting radiofrequency ablation outcome in the myocardium in vivo. J Cardiovas Magn Reson (2017) 19:14
3. Bock, M., et al. Active catheter tracking using parallel MRI and real-time image reconstruction. Magn Reason Med (2006) 55(6): p1454-9.
4. W. Ullah, R. J. Hunter, V. Baker, M. B. Dhinoja, S. Sporton, M. J. Earley, et al. Factors affecting catheter contact in the human left atrium and their impact on ablation efficacy. J Cardiovasc Electrophysiol (2015) 26(2): p129-36. Accession Number: 25213917 DOI: 10.1111/jce.12542
5. Mooiweer, R., et al. Active Tracking-based cardiac triggering for MR-thermometry during radiofrequency ablation therapy in the left ventricle. (2022) Front Cardiovasc Med 9: 971869.
Figures