2696
Portable ultra-low-field brain MRI: test-retest reliability and correspondence to high-field MRI1Department of Neuroimaging, King's College London, London, United Kingdom, 2Hyperfine, Inc., Guildford, CT, United States, 3Center for the Developing Brain, King's College London, London, United Kingdom, 4Medical Research Council Center for Neurodevelopmental Disorders, King's College London, London, United Kingdom, 5Department of Forensics and Neurodevelopmental Sciences, King's College London, London, United Kingdom, 6Bill and Melinda Gates Foundation, Seattle, WA, United States, 7Department of Old Age Psychiatry, King's College London, London, United Kingdom
Synopsis
Keywords: Gray Matter, Segmentation, Analysis/Processing, Brain, Data Acquisition, Validation
Motivation: Ultra-low-field MRI scanners offer a cost-effective and portable alternative to high-field neuroimaging.
Goal(s): To quantify between-scanner test-retest reliability of 64mT brain scans, and their correspondence to 3T MRI.
Approach: We scanned 23 healthy participants on two Hyperfine 64mT scanners and a GE 3T scanner using T1w and T2w scans at multiple resolutions. We segmented images into 98 structures and estimated their volumes.
Results: We demonstrate excellent reliability of volumetric estimates from ultra-low-field MRI, and high correspondence to high-field scans. The highest reliability and high-field correspondence was obtained using T2w ultra-low-field scans, super-resolved by combining three orthogonal acquisitions with low through-plane resolution.
Impact: Measures of brain volume from Hyperfine portable ultra-low-field MRI scans show excellent test-retest reliability across scanners, and excellent correspondence to similar estimates from high-field MRI. This enables quantitative analysis of cost-effective and portable neuroimaging in various contexts, including low-resource environments.
Introduction
Ultra-low-field magnetic resonance imaging (MRI) scanners, such as the 64mT Hyperfine Swoop, promise to revolutionise medical (neuro)imaging 1. The Hyperfine scanner runs using a standard electrical socket, without cryogenics or shielding; as a result, scans incur only a fraction of the cost of a high-field scan. The system is portable, enabling scanning at the bedside, and in low and middle income countries with limited access to MRI. However, it is unclear whether ultra-low-field brain scans can be used to reliably extract quantitative estimates of tissue volume, and to what extent these measurements correspond to state-of-the-art estimates from high-field MRI.Methods
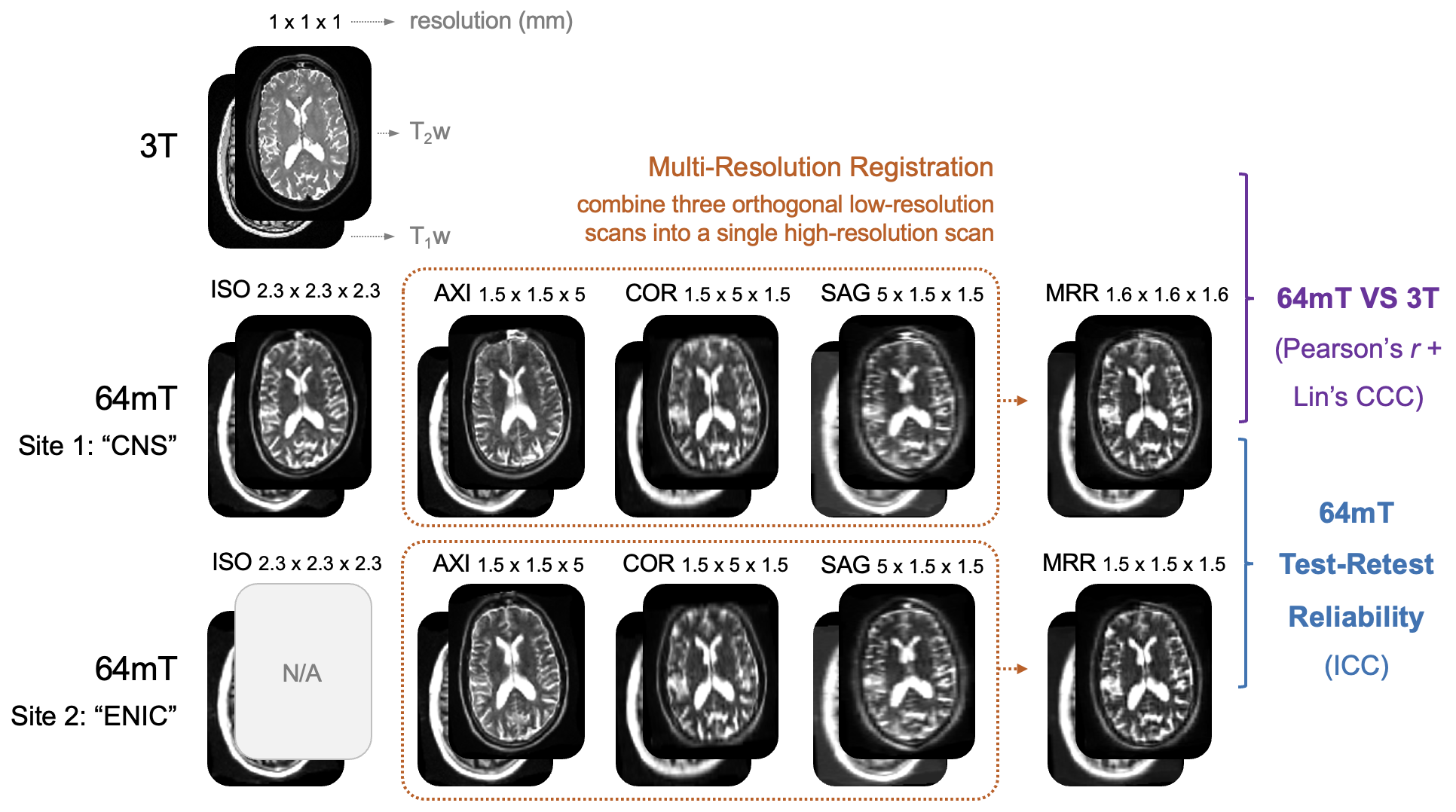
We recruited 23 healthy adult participants, with 2/3 male and 2/3 female participants across each of five age-defined strata: 20–29, 30-39, 40-49, 50-59 and 60-69 years old. Participants were scanned on a 3T high-field MRI scanner (GE Premier) and two identical portable 64mT ultra-low-field MRI scanners (Hyperfine Swoop) located at different sites, using T1w and T2w scans. High-field scans were acquired at 1x1x1 mm resolution, while ultra-low-field scans were acquired both using non-isotropic product sequences (T1w: 1.6x1.6x5 mm / T2w: 1.5x1.5x5 mm, with high resolution within the axial, sagittal or coronal plane), and a custom isotropic sequence (2.3x2.3x2.3 mm). We used multi-resolution registration (MRR) to super-resolve the three orthogonal non-isotropic ultra-low-field scans into a single higher-resolution (T1w: 1.6x1.6x1.6 mm / T2w: 1.5x1.5x1.5 mm) ultra-low-field scan 2 (Fig. 1).We then used SynthSeg+ 3 to automatically segment each scan into a total of 98 structures (including parcellation of cortical and subcortical grey matter, white matter and cerebrospinal fluid), and estimate their volumes. We assessed the test-retest reliability of volume estimates using ICC(3,1) (the one-way random effects model for the consistency of single measurements 4), hereafter referred to as ICC. We assessed the correspondence of tissue volume estimates from ultra-low-field and high-field scans using both Pearson’s r – to quantify linear correlation; and Lin’s Concordance Correlation Coefficient (CCC) – to quantify exact agreement, or alignment with the “y=x” identity line. We repeated all analyses on both T1w and T2w scans, across ultra-low-field resolutions; i.e. axial / sagittal / coronal / isotropic / MRR.
Results
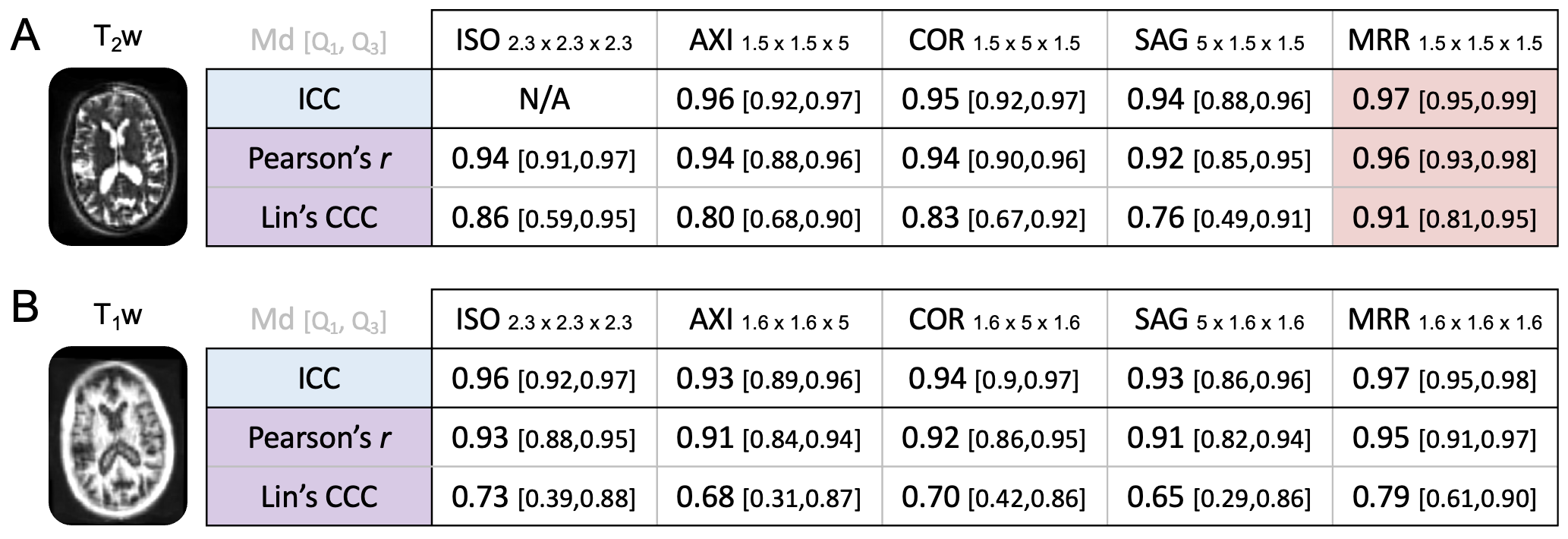
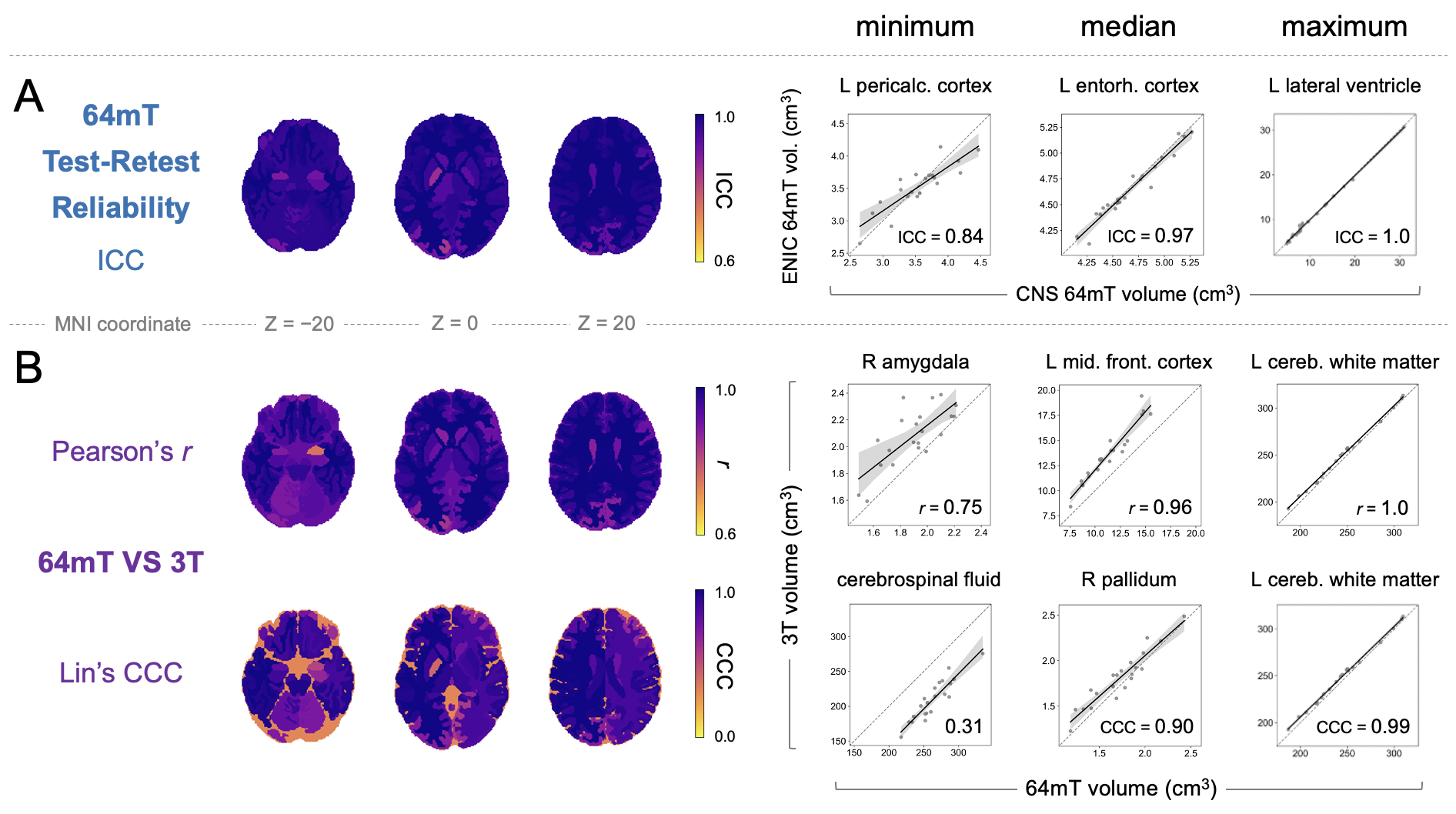
We report summary statistics as Median [first, third quartile] across 98 segmentation labels (regions), or Md [Q1,Q3] (Fig. 2).Both T1w and T2w ultra-low-field scans showed high between-scanner test-retest reliability, across scan resolutions (Fig. 2, Fig. 3A). The highest test-retest reliability was shown by quantifying volume using T2w ultra-low-field scans super-resolved using MRR (ICC Md [Q1,Q3] = 0.97 [0.95,0.99]; Fig. 2A). Reliability of volumes extracted from non-isotropic ultra-low-field T2w scans was marginally lower (Md ICC = 0.94-0.96). Volume estimates from MRR-super-resolved ultra-low-field T1w scans showed similarly high reliability to T2w scans. Reliability of ultra-low-field T1w scans acquired at 2.3mm isotropic resolution was marginally lower, followed by non-isotropic scans.
Volumes extracted from ultra-low-field scans showed excellent correspondence to high-field counterparts across participants (as quantified by Pearson’s r) but also slight systematic offsets in volume measurements (as quantified by Lin’s CCC) (Fig. 2, Fig. 3B). The highest correspondence to high-field was shown by ultra-low-field T2w scans super-resolved using MRR, including both high linear correlation (Pearson’s r Md [Q1,Q3] = 0.96 [0.93,0.98]) and agreement (Lin’s CCC Md [Q1,Q3] = 0.91 [0.81,0.95]) (Fig. 2A). Correspondence of 2.3mm isotropic ultra-low-field T2w scans to high-field counterparts was marginally lower (Md Pearson's r = 0.94; Lin's CCC = 0.86), followed by non-isotropic scans (Md Pearson’s r = 0.92-0.94; Lin’s CCC = 0.76-0.83). MRR-super-resolved T1w scans showed marginally lower linear correlation to high-field data than T2w scans (Pearson’s r Md [Q1,Q3] = 0.95 [0.91,0.97]) as well as lower agreement (Lin’s CCC Md [Q1,Q3] = 0.79 [0.61,0.90]). Reliability of T1w scans acquired at 2.3mm isotropic resolution was lower, followed by non-isotropic scans.
Discussion
Test-retest reliability of volumetric estimates from ultra-low-field scans MRI and correspondence to high-field counterparts was higher for T2w scans than T1w scans, and highest for scans super-resolved using multi-resolution registration 2. T1w sequence parameters used at 64mT resulted in non-zero cerebrospinal fluid (CSF) signal and partial-volume signal voids at tissue interfaces, possibly explaining lower correspondence to high-field; updated parameters now yield T1w with nulled CSF signal, which may produce more consistent results. Our results pave the way for further quantitative analyses of portable ultra-low-field neuroimaging scans, including for the modelling of individual deviations from the norm 5,6 or estimation of biomarkers of brain health such as brain age 7, across development 8 and disease 9.Conclusion
Volumetric estimates from Hyperfine ultra-low-field MRI scans show excellent test-retest reliability, and correspondence to similar estimates from high-field MRI.Acknowledgements
We thank all participants for taking part in this study. This project was supported the National Institutes of Health Research Biomedical Research Council, and by the Bill and Melinda Gates Foundation - through the Ultra-Low Neuroimaging in the Young (UNITY) consortium.References
1. Arnold, T. C., Freeman, C. W., Litt, B., & Stein, J. M. (2023). Low-field MRI: Clinical promise and challenges. Journal of Magnetic Resonance Imaging, 57(1), 25–44.
2. Deoni SCL, O’Muircheartaigh J, Ljungberg E, et al. (2022). Simultaneous high-resolution T2 -weighted imaging and quantitative T2 mapping at low magnetic field strengths using a multiple TE and multi-orientation acquisition approach. Magnetic Resonance in Medicine, 88(3), 1273–1281.
3. Billot B, Magdamo C, Cheng Y, et al. (2023). Robust machine learning segmentation for large-scale analysis of heterogeneous clinical brain MRI datasets. Proceedings of the National Academy of Sciences, 120(9), e2216399120.
4. Chen G, Taylor PA, Haller SP, et al. (2018). Intraclass correlation: Improved modeling approaches and applications for neuroimaging. Human Brain Mapping, 39(3), 1187–1206.
5. Bethlehem RAI, Seidlitz J, White SR, et al. (2022). Brain charts for the human lifespan. Nature, 604(7906), Article 7906.
6. Rutherford S, Kia SM, Wolfers T, et al. (2022). The normative modeling framework for computational psychiatry. Nature Protocols, 17(7), Article 7.
7. Cole JH & Franke K (2017). Predicting Age Using Neuroimaging: Innovative Brain Ageing Biomarkers. Trends in Neurosciences, 40(12), 681–690.
8. Deoni SCL, Bruchhage MMK, Beauchemin J, et al. (2021). Accessible pediatric neuroimaging using a low field strength MRI scanner. NeuroImage, 238, 118273.
9. Venkataraman A, Marshall C, & Rittman T (2023). Automated brain image analysis in dementia using artificial intelligence: A roadmap for the development of clinical tools. OSF Preprints.
Figures