2685
Clinical Imaging of Patients with Spinal Hardware at 0.55T: Diagnostic Feasibility and Metallic Artifact Comparison to 1.5/3T1Department of Radiology, University of Michigan, Ann Arbor, MI, United States
Synopsis
Keywords: Low-Field MRI, Low-Field MRI, Hardware, Spine
Motivation: MR image quality concerns due to metallic implants may be addressed by preferentially scanning on 0.55T units.
Goal(s): To assess image quality, metallic artifacts, and diagnostic agreement secondary to spinal hardware at 0.55T compared to higher-field imaging.
Approach: Two blinded neuroradiologists independently reviewed 20 0.55T studies and 10 paired high-field studies. Diagnostic efficacy of 0.55T scans was assessed via pick-list, and image quality and metal artifact reduction were assigned scaled ratings.
Results: 0.55T produced studies with high diagnostic efficacy (16/20 studies had complete or near-complete agreement) and equivalent or improved image quality compared to higher-field images.
Impact: Commercial 0.55T MRI systems may improve the appearance of artifacts caused by spinal hardware compared to higher fields, and can be used in routine clinical practice without compromising image quality or diagnostic efficacy.
Introduction
MRI in patients with metallic implants is a challenge in clinical practice, as imaging on 1.5/3T systems can lead to disruptive susceptibility artifacts1 and heating of the implants2. Recently, a commercial 0.55T MRI system has been introduced with the goal of reducing operating costs3 and improving patient-comfort due to reduced acoustic noise and a larger bore size4. Because of the direct relationship between artifact from metal (signal loss, pileup, image distortion) and magnetic field strength5, imaging patients with metallic implants on a commercial 0.55T MRI system may be beneficial. The purpose of this study is to assess the diagnostic efficacy of post-surgical spinal imaging at 0.55T and compare the image quality to paired high-field scans.Methods
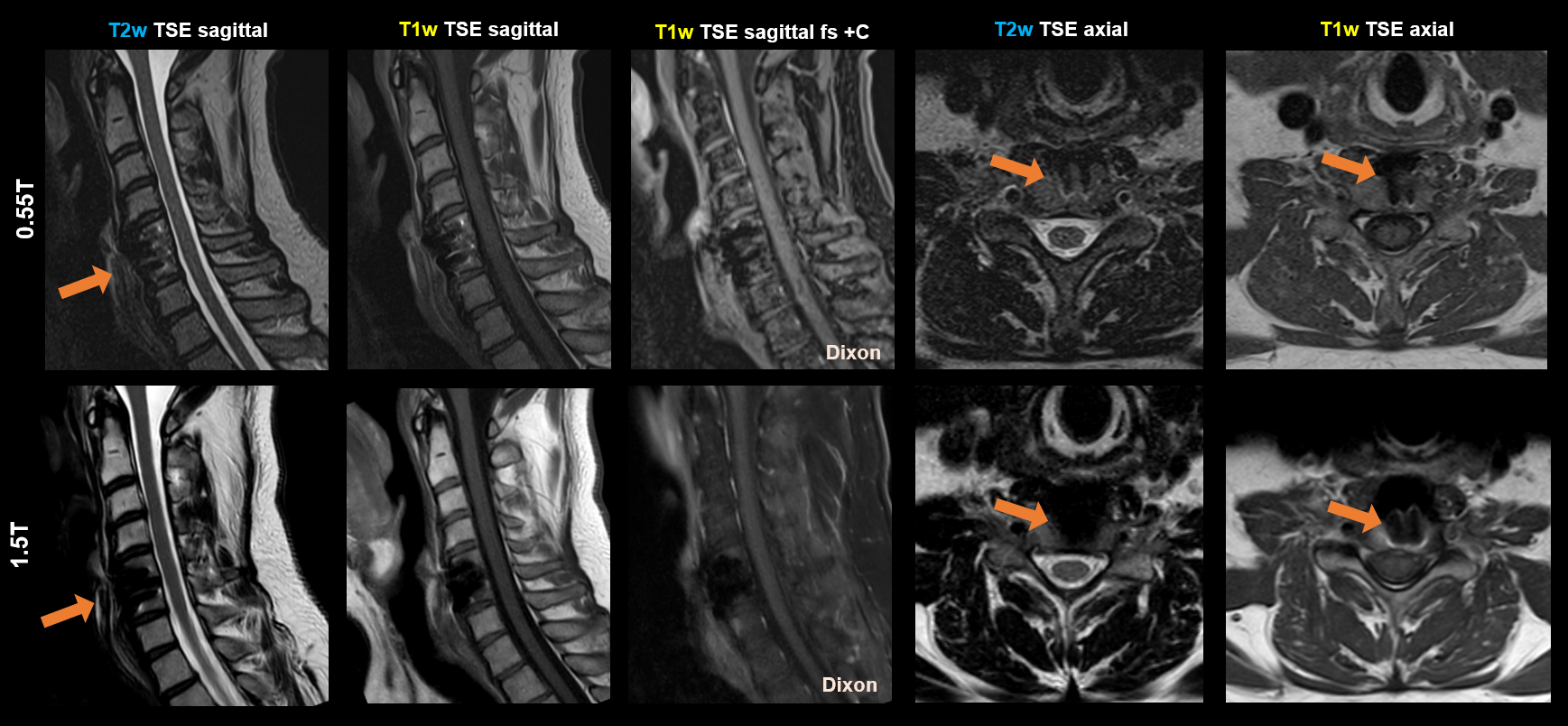
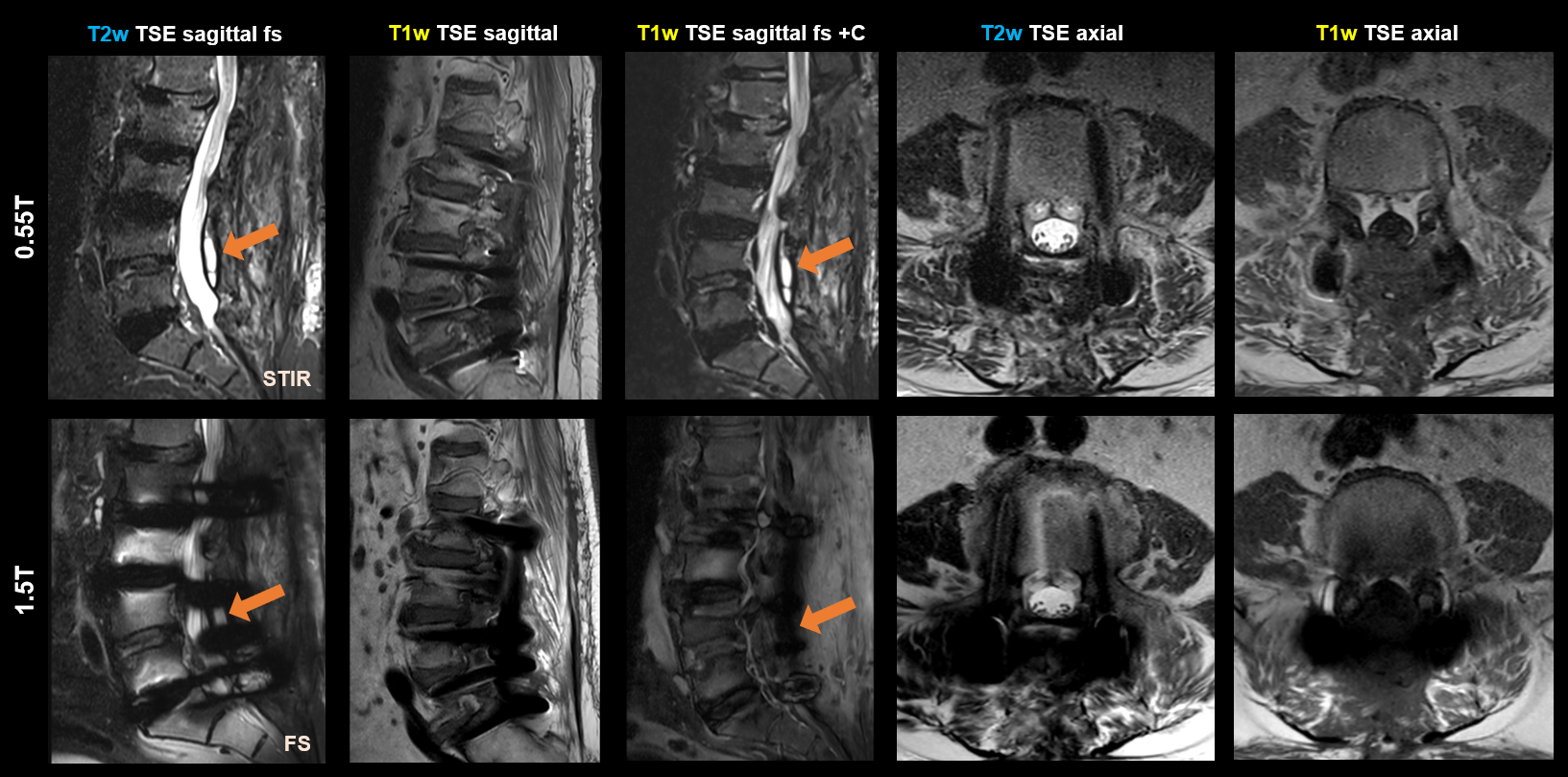
Retrospective assessment was performed for 20 patients with spinal hardware who underwent MRI imaging at 0.55T between 12/17/2021-10/4/2023; 10 were found to have a previously acquired high-field (1.5T or 3T) scan with the hardware in-situ. Limited sequences which appeared in both 0.55T and high-field exams were selected for review, specifically sagittal and axial T1w TSE, sagittal T1w TSE with fat suppression post-contrast, sagittal and axial T2w TSE, and sagittal T2w TSE with fat suppression. Due to the small sample size in the sagittal T2w TSE fat suppression cohort (n=5), Dixon, short tau inversion recovery (STIR), and frequency-selective fat saturation “fs” sequences were aggregated into one category.All studies were randomized and anonymized to field strength, and two neuroradiologists with 40 (R1) and 6 years (R2) of professional experience independently reviewed the images blinded to patient history. For all 0.55T studies, readers were asked to select diagnoses from a pick-list of conditions including osteomyelitis/discitis, compression fracture, post-operative fluid collection, cord/conus signal abnormality, and osseous metastatic disease. For 0.55T studies with high-field comparisons, readers were asked to rate the limited sequences using a 1-4 Likert scale for overall image quality (IQ) (1=non-diagnostic/unacceptable, 4=excellent) and metal artifact severity (MA) (1=non-diagnostic/severe artifacts, 4=no visible artifacts) for both field strengths.
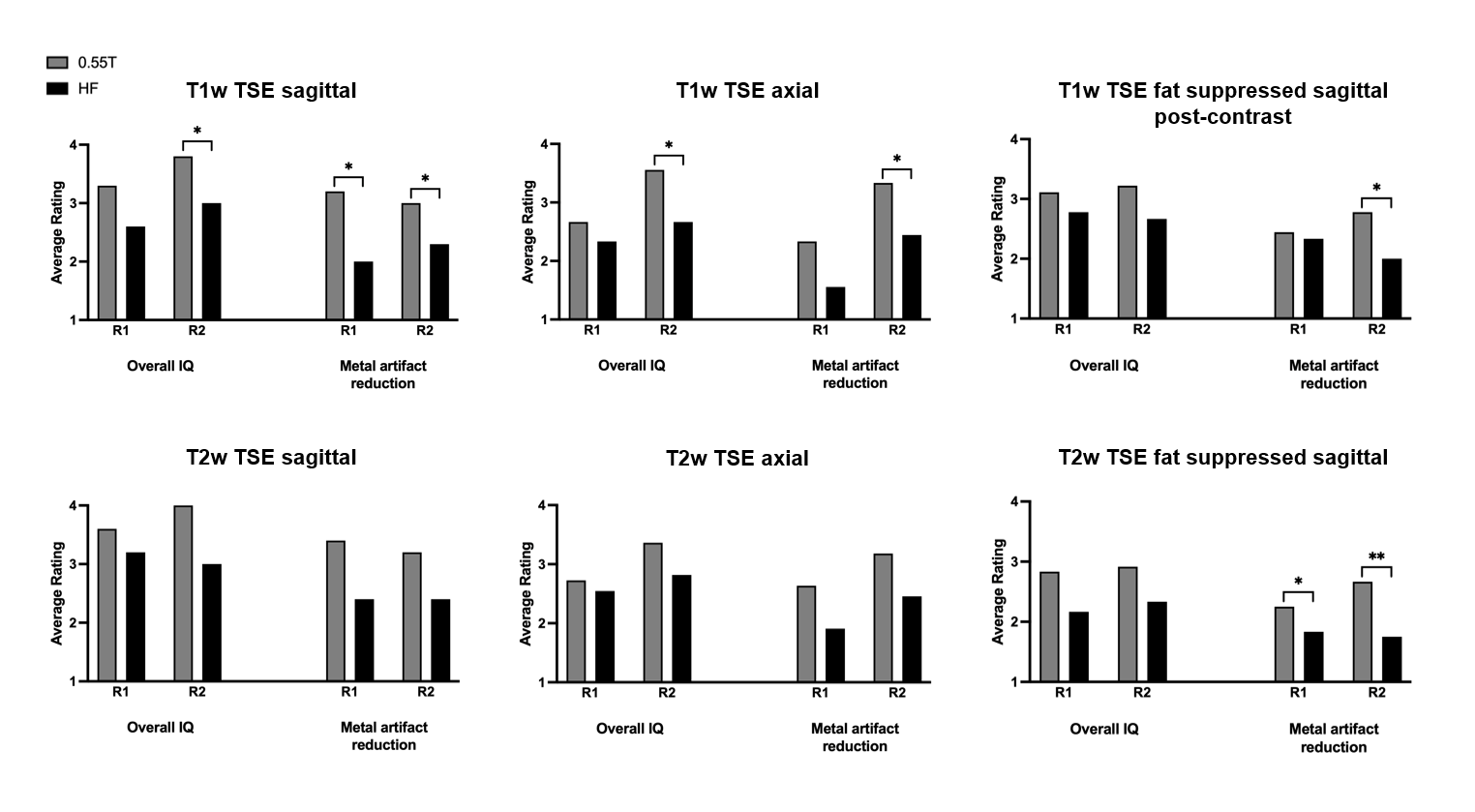
Wilcoxon signed-rank tests were applied to determine differences between the paired 0.55T and high-field ratings for IQ and MA for each sequence. P-value <0.05 was considered statistically significant.
Results
There was complete agreement in 6/20 cases and near-complete agreement in 10/20 cases where agreement was present on the primary diagnosis, but one reader selected one or more additional diagnoses. Non-agreement occurred in 4/20 cases, 3 of which were disagreements on the degree of degenerative stenosis. For IQ and MA ratings, all sequences at 0.55T were statistically comparable or better than high-field.For reader 1 (R1), overall IQ and MA scores between low- and high-field images were not statistically significant for most sequences, specifically sagittal T1w TSE (IQ p= 0.0625), axial T1w TSE (IQ p=0.6562, MA p=0.125), fat-suppressed sagittal T1w TSE post-contrast (IQ p=0.625, MA p>0.999), sagittal T2w TSE (IQ p=0.500, MA p=0.250), axial T2w TSE (IQ p=0.513, MA p=0.0938), and fat-suppressed sagittal T2w TSE (IQ p=0.513, MA p=0.3125). The exception was an improved MA score for sagittal T1w TSE images at 0.55T compared to high-field (MA p=0.0234).
For reader 2 (R2), the 0.55T scans had significantly higher IQ and MA scores than high-field for sagittal T1w TSE (IQ p=0.0312, MA p=0.0312), axial T1w TSE (IQ p=0.0312, MA p=0.0156), and fat-suppressed sagittal T2w TSE (IQ p=0.0312, MA p=0.0039). Scores for were similar for IQ and MA between 0.55T and high-field for sagittal T2w TSE (IQ p=0.125, MA p=0.250), and axial T2w TSE (IQ p=0.0625, MA p=0.0547). For fat-suppressed sagittal T1w TSE post-contrast, IQ was scored similarly (p=0.0625), but MA was improved at 0.55T compared to high-field (p=0.0391).
Discussion
Despite inherently lower SNR of 0.55T systems, our results found high diagnostic agreement in assessment of routine spinal pathology between two readers of different experience levels. This suggests that commercial 0.55T systems can be reliably used in routine imaging of patients with spinal hardware.All sequences assessed at 0.55T were found to be similar or superior to high-field systems in the presence of hardware based on overall image quality and impact of metallic artifact. No 0.55T sequences were rated significantly worse than at higher field. This work suggests imaging of spinal hardware at 0.55T may be advantageous to imaging at higher field strengths. Further work includes optimization of the sequences for MA reduction, stratification based on material and extent of hardware, and incorporation of additional readers.
Conclusion
Imaging of patients with spinal hardware on a commercial 0.55T MRI system results in equivalent or higher image quality, and equivalent or reduced metal artifacts compared to higher-field systems without compromising diagnostic efficacy.Acknowledgements
No acknowledgement found.References
1Jungmann, Pia M., et al. "Advances in MRI around metal." Journal of magnetic resonance imaging 46.4 (2017): 972-991.
2Winter, Lukas, et al. "MRI‐related heating of implants and devices: a review." Journal of Magnetic Resonance Imaging 53.6 (2021): 1646-1665.
3Vosshenrich, Jan, et al. "Economic aspects of low-field magnetic resonance imaging: Acquisition, installation, and maintenance costs of 0.55 T systems." Der Radiologe 62.5 (2022): 400-404.
4Rusche, Thilo, et al. "More Space, Less Noise—New-generation Low-Field Magnetic Resonance Imaging Systems Can Improve Patient Comfort: A Prospective 0.55 T–1.5 T-Scanner Comparison." Journal of Clinical Medicine 11.22 (2022): 6705.
5Lee, Elizabeth M., et al. "Improving MR image quality in patients with metallic implants." Radiographics 41.4 (2021): E126-E137.
Figures