2673
Quantitative and Qualitative Correlation of 0.55T MRI to CT for Normal Anatomic Structures and Common Pulmonary Pathologies1School Of Medicine, University of California, San Francisco, San Francisco, CA, United States, 2Department of Radiology & Biomedical Imaging, University of California, San Francisco, San Francisco, CA, United States, 3College of Medicine, University of South Alabama, Mobile, AL, United States, 4Siemens Medical Solutions USA, Inc., Malvern, PA, United States
Synopsis
Keywords: Low-Field MRI, Low-Field MRI, Lung, Tissue Characterization, Reader Performance Study
Motivation: Although MRI has had low adoption in lung imaging due to susceptibility artifacts, limiting its utility in pulmonary parenchymal imaging, low-field MRI (0.55T) has potential to address those limitations.
Goal(s): However, its thoracic diagnostic capabilities remain indeterminate, so our goal was to compare its ability to detect common lung pathologies to chest CT and provide comparable quantitative measurements.
Approach: Structures and pathologies were measured with both modalities, and two radiologists identified lung pathologies with MRI only.
Results: Results indicated that readers were able to detect pathologies using 0.55T MRI, serving as a first step in exploring 0.55T MRI as an alternative modality.
Impact: Our study revealed potential for 0.55T MRI as an emerging tool for MR-based anatomic evaluation of the lung, and its limitations. This can expand lung imaging options and potentially provide better tissue characterization for diagnoses like lung cancer.
Introduction
Although MRI for lung imaging has had challenges due to image degradation, the newly emerging low field (0.55T) MR system has the advantage of reduced susceptibility artifact at the air-tissue interface while also offering modern image acquisition and respiratory navigation technologies1-5. Our objective is to evaluate the ability of 0.55T MRI to detect and provide comparable measurements of normal anatomic structures and lung pathologies to chest CT. Furthermore, we wanted to conduct a reader performance study to evaluate whether radiologists can identify common lung pathologies from only reading 0.55T MRI. We hypothesize that quantitative measurements of normal thoracic anatomic structures and common lung pathologies will be well correlated between these imaging modalities, and that readers can diagnose and identify common lung pathologies using 0.55T MRI only.Methods
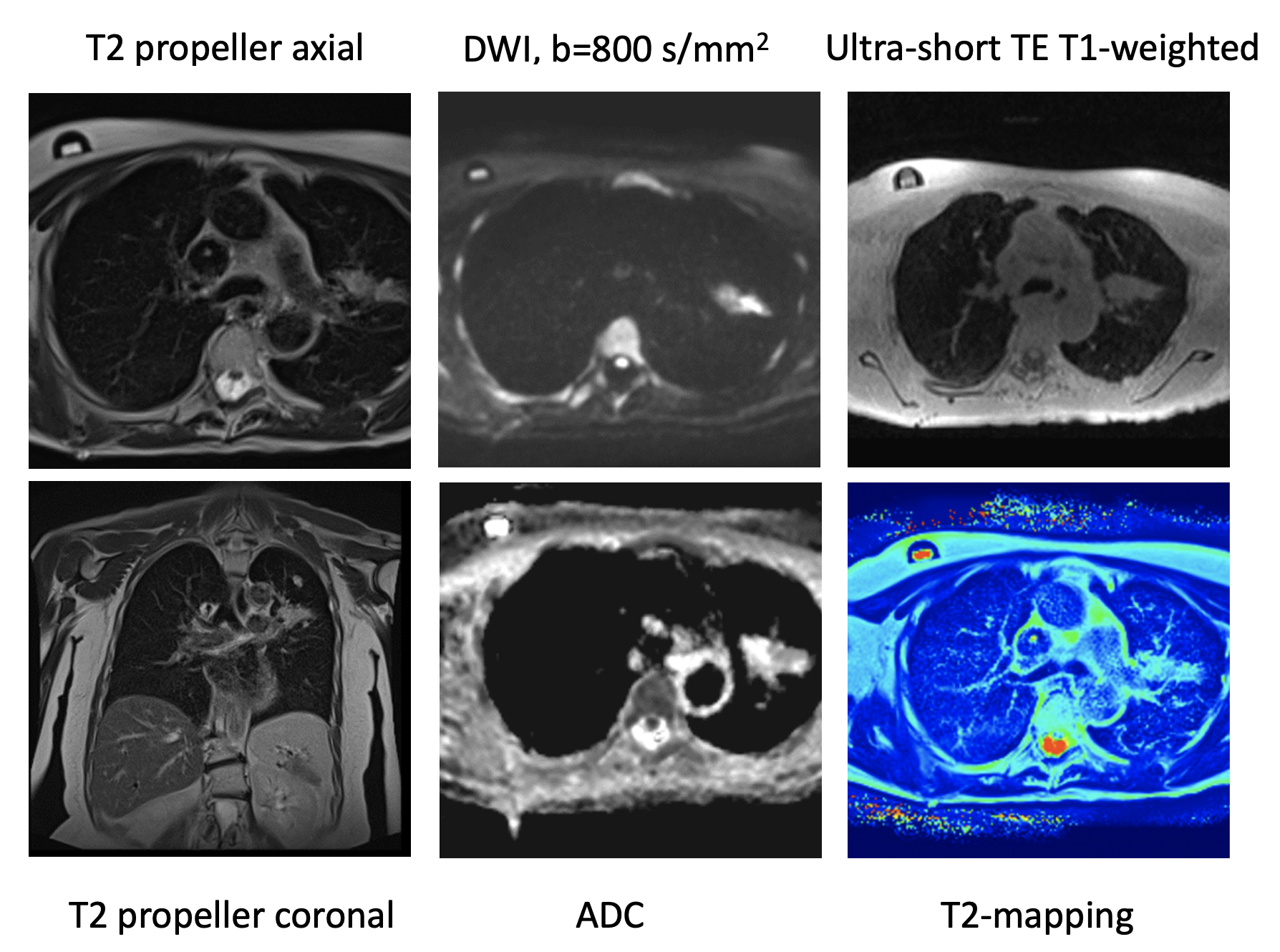
We prospectively enrolled 28 patients with heterogeneous pulmonary pathologies encompassing benign nodules, malignancies, infections, bronchiectasis, and interstitial lung diseases, who concurrently underwent same-day CT or PET/CT. A 0.55T scanner (MAGNETOM Free.Max system, Siemens Healthcare, Erlangen, Germany) was used with respiratory-navigated T2 BLADE Coronal, T2 BLADE Axial, T1 ultrashort echo time (UTE) with spiral readout, and diffusion weighted imaging (DWI) sequences (both UTE and DWI using research applications). A sample low-field MRI protocol is shown in Figure 1. The maximum diameter of the ascending aorta, descending aorta, left and right branch pulmonary arteries, main pulmonary artery, mid thoracic trachea, and sternal thickness were measured with CT and T2 BLADE Axial sequence. Representative lymph nodes, nodules of varying sizes, and consolidations described on the CT report were measured with CT and T2 BLADE Axial, or UTE if not visible on T2 BLADE Axial. Measurements were compared using coefficient of determination (R2) with significant correlation defined as P < 0.05. Mean of absolute difference (MAD) was also calculated.Six radiologists as part of a reader performance study independently read all corresponding CT images and then graded the overall image quality of MRI images on a 3-point Likert-type scale (1=low, 2=moderate, 3=good). Intraclass correlation coefficient was calculated for the standardized overall image quality gradings. After a four week wash out period, two readers identified the presence of common lung pathologies using only 0.55T MRI. Sensitivity was calculated as the percentage of major diagnoses reported on CT that were identified and visible to the reader on MRI by each pathology category.
Results
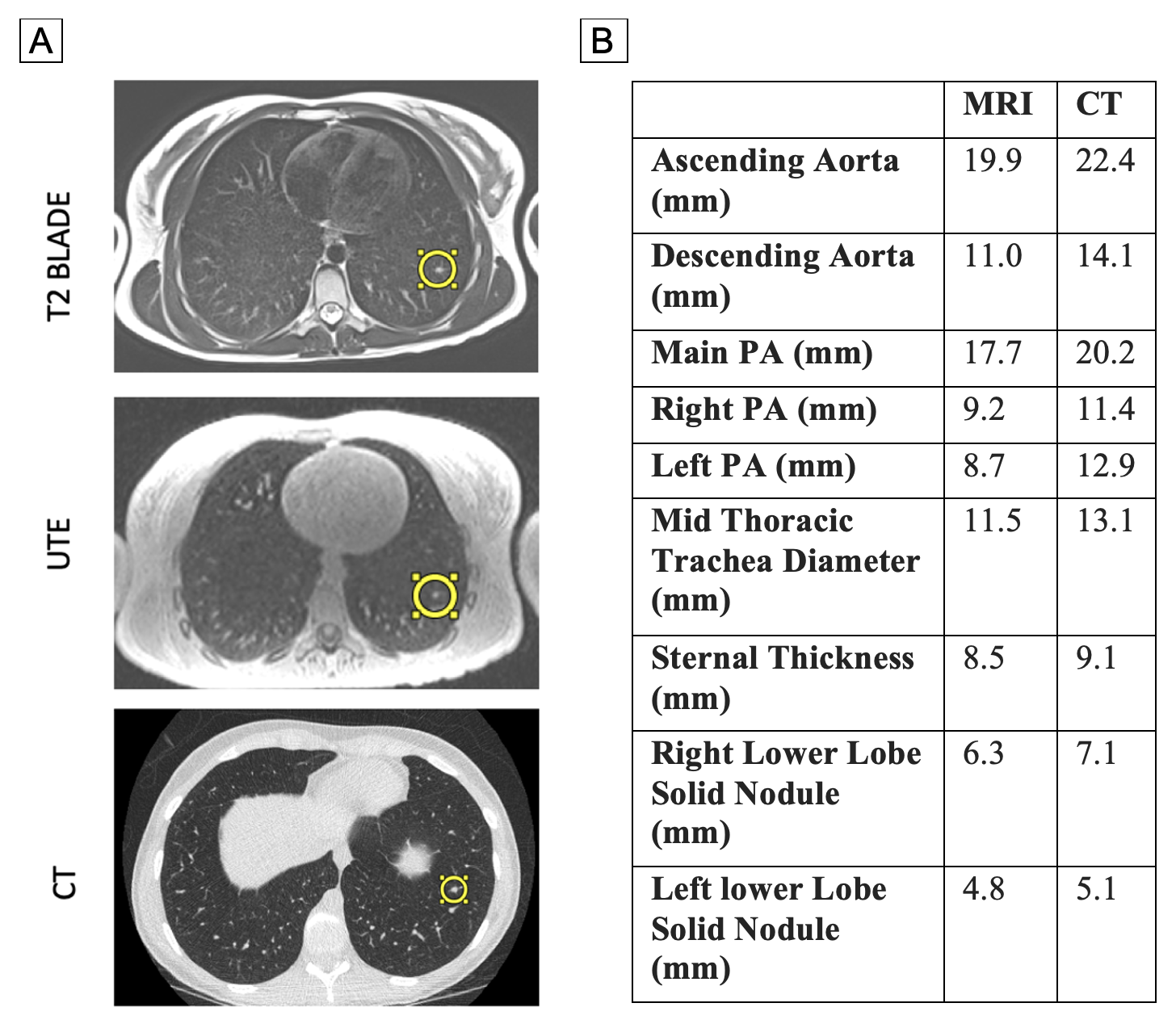
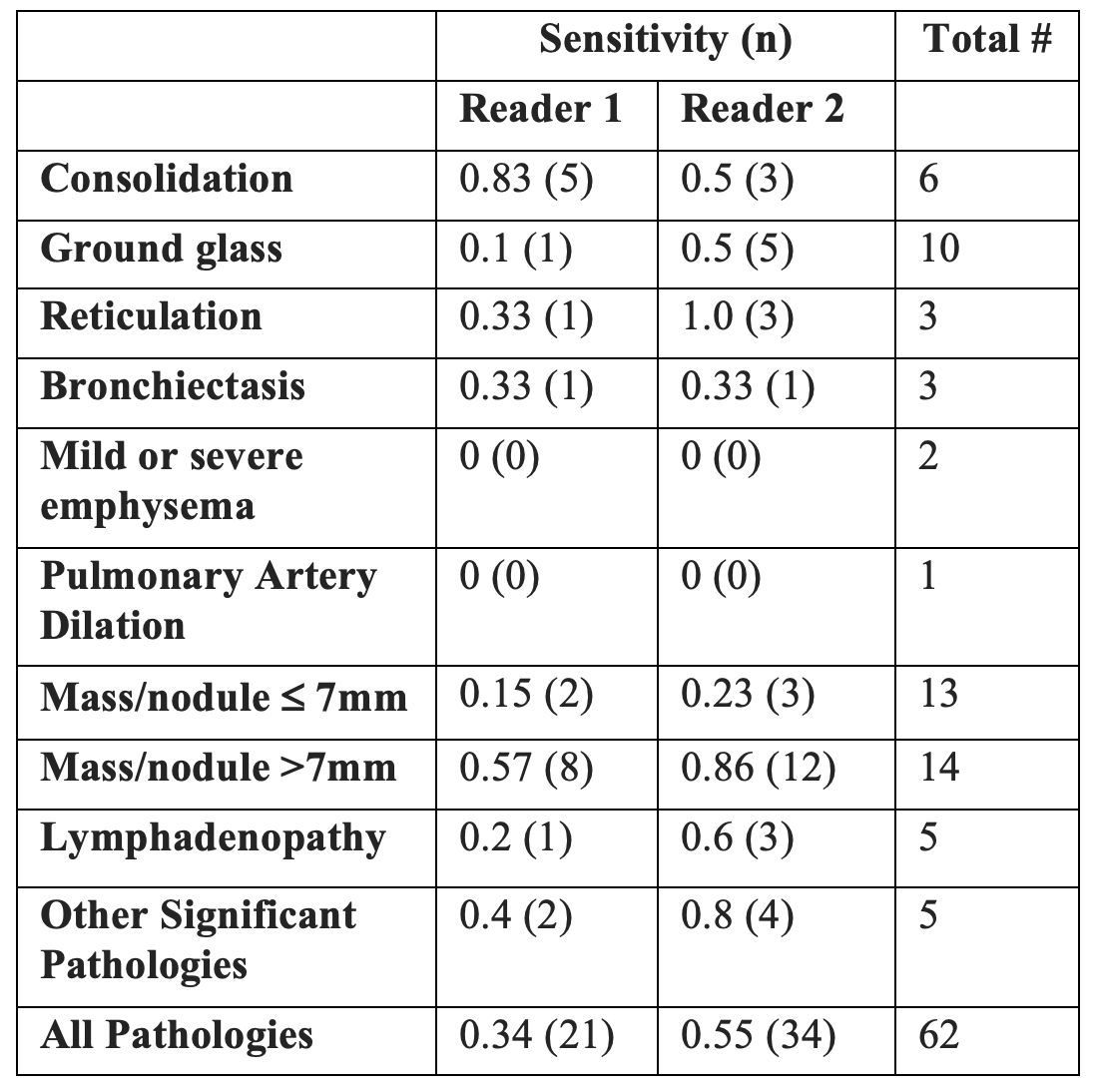
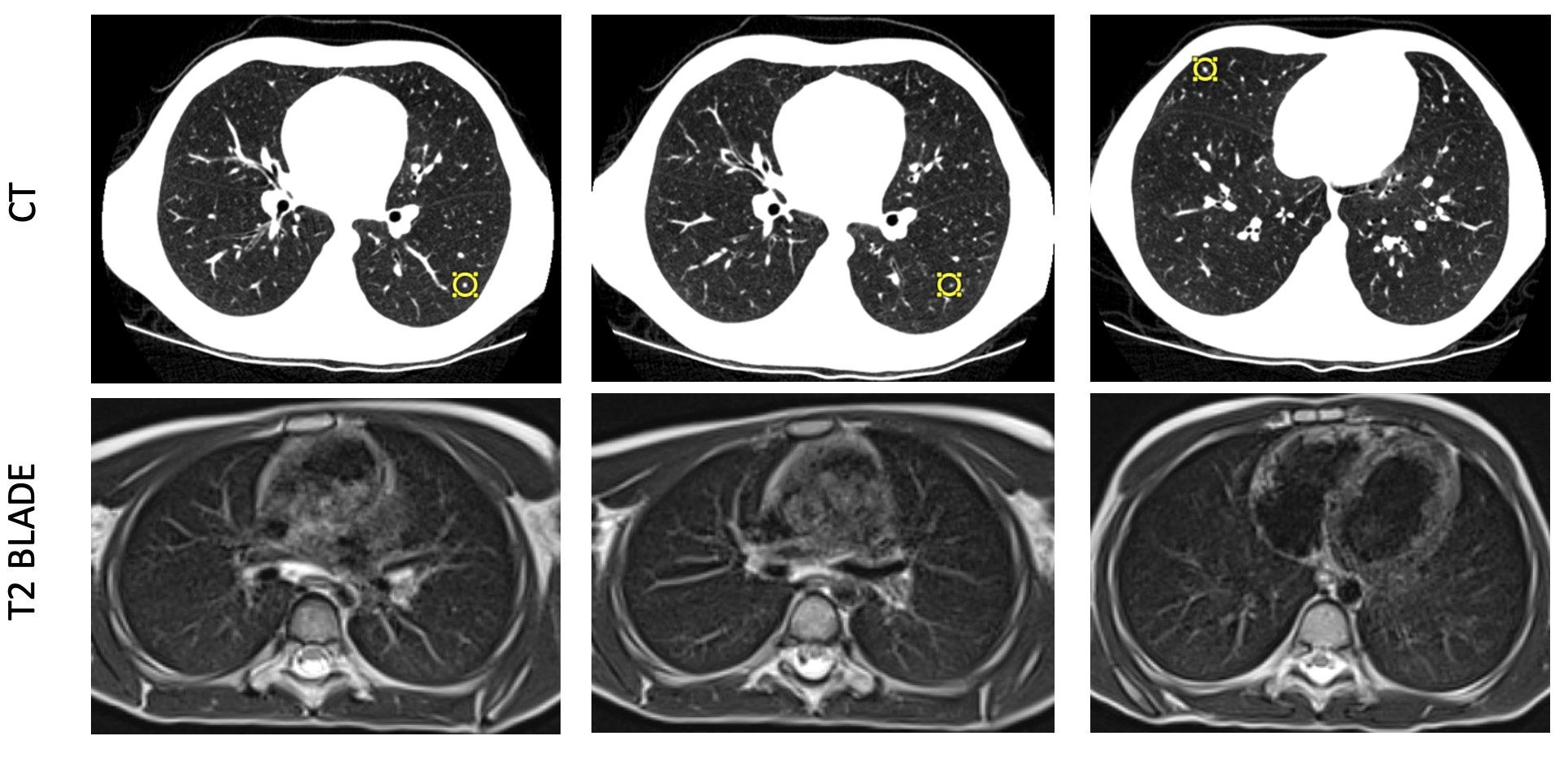
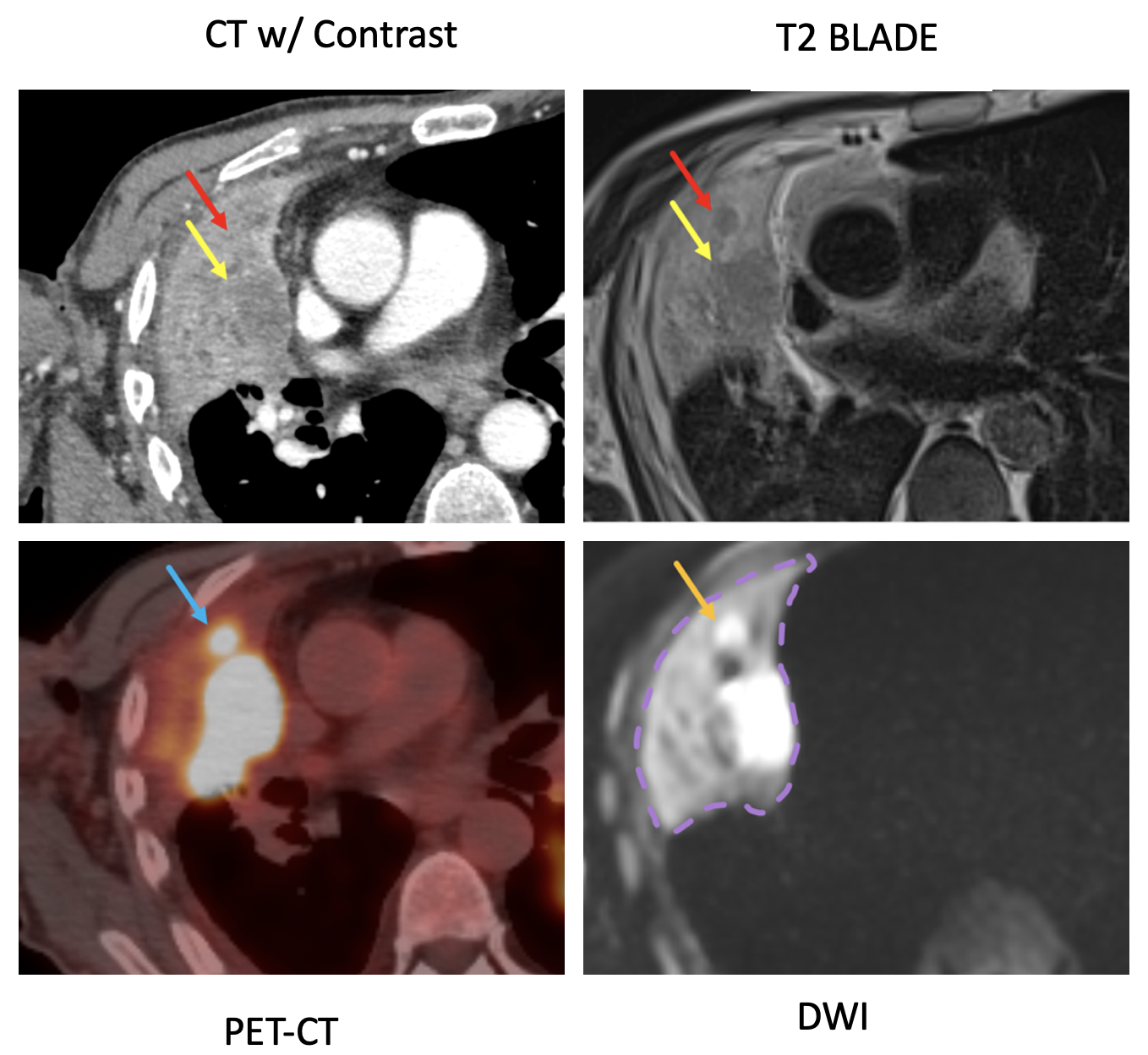
An overall correlation of R2 = 0.89 was observed for the ascending aorta; 0.79, descending aorta; 0.73, main pulmonary artery; 0.74, right pulmonary artery; 0.27, left pulmonary artery; 0.93, mid-thoracic trachea diameter; 0.81, sternal thickness (P<0.0001). The MAD was the lowest for mid-sternal thickness at 0.63 mm, and highest for right pulmonary artery at 2.4 mm. For 24 pathologies measured (solid nodule = 15, subsolid nodule = 1, cavitary consolidation = 1, mass = 2, consolidation = 1, mediastinal lymph node = 4), we achieved overall R2 = 0.95 (P<0.0001) and MAD = 1.5 mm. Figure 2 shows a comparison of organ and nodule measurements with CT and MRI for a patient with scattered pulmonary nodules.Results of the reader performance study demonstrated a mean of 2.2 and standard deviation of 0.5 for overall image quality grading. Intraclass correlation was 0.44 after standardizing the image quality gradings. Sensitivity of pathology identification using 0.55T MRI was calculated, and was highest for consolidation (Reader 1) and reticulation (Reader 2) (Figure 3). Both readers were unable to identify emphysema and pulmonary artery dilation, and had trouble identifying pulmonary nodules smaller than 8 mm. Thus, CT is better for detection of small nodules <8mm, a significant limitation of 0.55T MRI (Figure 4). However, 0.55T MRI also has its strengths and potential applications, particularly for tumor recurrence detection. An example case in Figure 5 shows how detection of a satellite nodule adjacent to a dominant right upper lobe mass was obstructed by atelectasis in CT, but was conspicuous on DWI.
Conclusion
Low field (0.55T) MRI and CT demonstrated excellent quantitative correlation for normal thoracic anatomic structures and across a diverse set of pulmonary pathologies. Furthermore, our reader performance study results demonstrated overall good image quality for 0.55T and high sensitivity in the detection of consolidations and large nodules, but difficulty in detection of smaller nodules, emphysema, and pulmonary artery dilation. Particularly, an example case of tumor recurrence detection revealed a valuable area of application for 0.55T MRI. Hence, 0.55T MRI has potential for expanding lung imaging options for radiosensitive populations and providing better tissue characterization for lung cancer.Acknowledgements
This project was supported by a University of California, San Francisco, Department of Radiology and Biomedical Imaging’s Seed Grant and a RSNA Medical Student Grant. Special thanks to every member of the Sohn Laboratory, readers of the 0.55T MRI reader performance study, and the MRI imaging scientists at Siemens Healthineers for their generous support.References
- Bergin CJ, Glover GH, Pauly JM. Lung parenchyma: magnetic susceptibility in MR imaging. Radiology. 1991 Sep;180(3):845-8. doi: 10.1148/radiology.180.3.1871305. PMID: 1871305.
- Campbell-Washburn AE, Malayeri AA, Jones EC, et al. T2-weighted Lung Imaging Using a 0.55-T MRI System. Radiology: Cardiothoracic Imaging. 2021;3:e200611 doi: 10.1148/ryct.2021200611.
- Campbell-Washburn AE, Ramasawmy R, Restivo MC, et al. Opportunities in Interventional and Diagnostic Imaging by Using High-Performance Low-Field-Strength MRI. Radiology. 2019;293:384–393 doi: 10.1148/radiol.2019190452.
- Kumar S, Liney G, Rai R, et al. Magnetic resonance imaging in lung: a review of its potential for radiotherapy. Br J Radiol. 2016 April; 89(1060): 20150431. doi: 10.1259/bjr.20150431
- Wild JM, Marshall H, Bock M, et al. MRI of the lung (1/3): methods. Insights Imaging. 2012 Aug;3(4):345-53. doi: 10.1007/s13244-012-0176-x.
Figures