2672
Free-breathing self-gated 5D whole-heart CMR at 0.55T: left ventricle, right ventricle, and left atrium function analysis in a single sequence1Department of Diagnostic and Interventional Radiology, Lausanne University Hospital (CHUV) and University of Lausanne (UNIL), Lausanne, Switzerland, 2Dorothy M. Davis Heart and Lung Research Institute, The Ohio State University, Columbus, OH, United States, 3Department of Biomedical Engineering, The Ohio State University, Columbus, OH, United States, 4CIBM Center for Biomedical Imaging, Lausanne, Switzerland, 5Department of Radiology, The Ohio State University, Columbus, OH, United States
Synopsis
Keywords: Low-Field MRI, Low-Field MRI, Heart, Cardiovascular, Pulse sequence design
Motivation: CMR has not seen widespread adoption beyond large urban academic centers. The reasons for this limited uptake include the cost and time-intensive nature of CMR. 5D Free-Running CMR using self-navigation (5D CMR) implemented on a low-field clinical scanner may help bridge this gap.
Goal(s): Investigate the feasibility of cardiac function measurements using 5D CMR on a 0.55T system.
Approach: 5D CMR data were collected in 10 adult subjects and compared to results from reference 2D cines. Right- and left-ventricular ejection fraction and left atrial volume were ascertained.
Results: 5D CMR allowed for time-efficient and concordant measurements when compared to the 2D reference method.
Impact: 5D Free-Running whole-heart CMR without the need for ECG, breath-holding, navigators, or complex scan plane planning enables a highly simplified and time-efficient assessment of myocardial function on a 0.55T clinical system in under 8 min.
Introduction
Routine cardiac magnetic resonance imaging (CMR) requires the use of breath-holds, navigators, and ECG to negate artifacts caused by cardiac and respiratory motion and to recover the motion of the heart.1–5 Recently, 5D Free-Running whole-heart CMR using total self-navigation (5D CMR) has been proposed.6 5D CMR improves the efficiency and accessibility of CMR by obviating the need for ECG placement, breath-holds, navigators, and complex scan plane planning.Additionally, having access to a 3D volume grants retrospective flexibility for slice orientations that were not planned during the scan - such as axial slices which have been shown to be more precise for RVEF quantification,7 and dedicated left atrium views which have been proven to provide more accurate atrial volume measurements.8
To support a simplified and time-efficient CMR exam with high flexibility, we implemented and tested 5D CMR on a 0.55T clinical system with moderate gradient performance in human subjects.
Methods
We implemented 5D CMR using a free-running 3D radial phyllotaxis bSSFP sequence with an RF excitation angle (FA) of 110°, a repetition time (TR) of 4.93ms, an echo time (TE) of 1.97ms, a bandwidth of 64kHz, 3723 shots, 18 segments and 1.4mm isotropic voxel size. The acquisition time was 7min50s.9,10As part of the free-running sequence, a superior-inferior readout was acquired every 18 k-space lines to extract the respiratory and cardiac motion signals. The k-space data was then sub-divided into 20 cardiac and 4 respiratory bins and compressed sensing was used to reconstruct the 5D CMR images (Fig.1).6
Data were collected in 10 healthy subjects on a 0.55T Free.Max scanner (Siemens Healthineers, Germany). 5D CMR was compared to the standard 2D breath-held end-expiration ECG-triggered cine11 images acquired in a short-axis stack (SAX), an axial stack, a two-chamber (2CH) view, a four-chamber (4CH) view, as well as LA-focused 2CH and 4CH views. The 5D CMR images were reformatted into 2D cine. The left ventricular (LV) and right ventricular (RV) ejection fraction (EF) were measured with CVI42 (Circle CVI) for the 5D CMR and SuiteHeart (Neosoft) for the 2D cine by two different observers. Left atrium minimum (LAVImin) and maximum (LAVImax) volume indices were measured on the LA-focused 2CH and 4CH views using the biplane area-length algorithm.8 Statistical significance was calculated using a paired Student’s t-test with p<0.05 considered significant.
Additionally, a GRE variant of 5D CMR was implemented for its use with contrast agent (Ferumoxytol) and tested in 2 volunteers (FA=20°, TR=4.77ms, TE=2.18ms, resolution=2mm isotropic).
Results
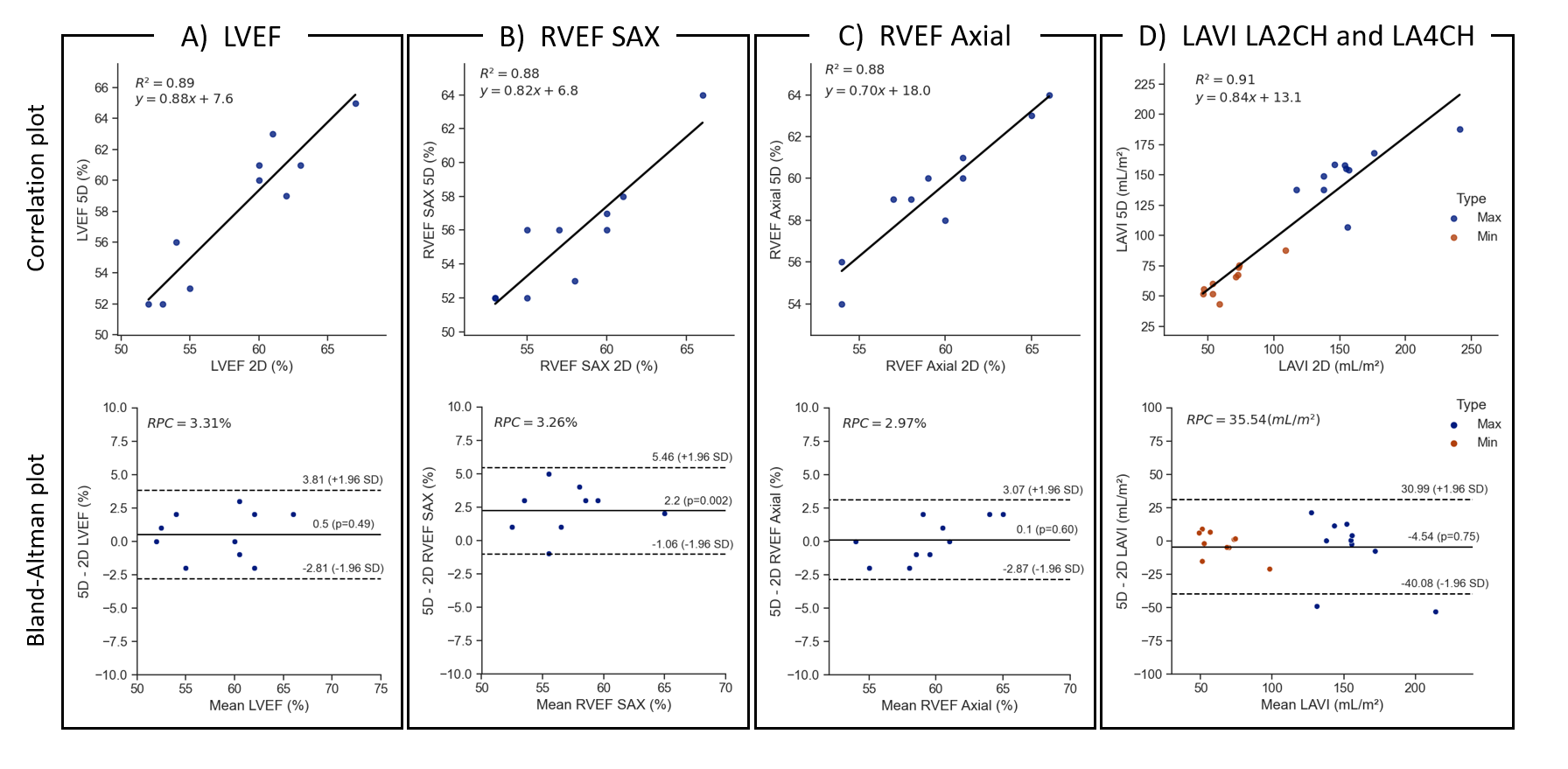
The segmentation of the blood pool was feasible in all cases, although the reformatted 5D CMR images demonstrated lower visual image sharpness and contrast when compared to the reference standard, (Fig.2 and Fig.3). The duration for all 2D cine acquisitions was 30-45min while that of 5D CMR was always 7min50s.The LVEF measurements from 5D CMR and the reference standard were in good concordance (58±5% and 59±5%, p=0.49) (Fig.3). RVEF was significantly different when measured on the SAX images (56±4% for 5D CMR and 58±5% for 2D cine, p=0.002), but not when measured on the axial view (60±3% for 5D CMR and 60±4% for 2D cine,p=0.85). The LAVImax was 29.2±3.9mL/m2 when measured on the 5D CMR images and 29.3±5.0mL/m2 on the 2D cines (p=0.9). The LAVImin volumes were similarly in good agreement with 10.6±2.4mL/m2 for 5D CMR and 10.8±2.2mL/m2 for the 2D cines (p=0.6, Fig.4).
The 5D CMR images obtained in subjects with Ferumoxytol yielded higher image quality and similar blood-myocardium contrast when compared to the non-contrast images (Fig.5).
Discussion
We demonstrated that 5D CMR supports the measurement of cardiac function on a 0.55T clinical system with moderate gradient performance. 5D CMR provides quantitative LV, RV and LA functional analysis results that are consistent with those from the reference standard while the 5D data were collected in under 7min50s using a single mouse-click to initiate the scans.Although 5D CMR results in lower image quality, it is more time-efficient, eliminates the need for ECG placement, breath-holding, and navigators, and therefore significantly improves efficiency, reduces operator and patient involvement, and abbreviates the scan duration decisively. This advances the hypothesis that 5D CMR will be less operator dependent and that there will no longer be a requirement for highly trained experts to collect CMR data. 5D CMR also provides a 3D volume that can retrospectively be reformatted into any anatomical views, thus removing the need for complex slice planning during the exam. This is advantageous for the accuracy of measurement on LA-focused views and on axial stack of cine which are not performed routinely in CMR.
Acknowledgements
This study was funded by the Swiss National Science Foundation (Grant Numbers 143923, 173129 and 167871).References
- Bluemke DA, Boxerman JL, Atalar E, et al. Segmented K-space cine breath-hold cardiovascular MR imaging: Part 1. Principles and technique. AJR Am J Roentgenol. 1997;169(2):395-400. doi:10.2214/ajr.169.2.9242742
- Larson AC, White RD, Laub G, et al. Self-gated cardiac cine MRI. Magn Reson Med. 2004;51(1):93-102. doi:10.1002/mrm.10664
- Larson AC, Kellman P, Arai A, et al. Preliminary investigation of respiratory self-gating for free-breathing segmented cine MRI. Magn Reson Med. 2005;53(1):159-168. doi:10.1002/mrm.20331
- Stehning C, Börnert P, Nehrke K, Eggers H, Stuber M. Free-breathing whole-heart coronary MRA with 3D radial SSFP and self-navigated image reconstruction. Magn Reson Med. 2005;54(2):476-480. doi:10.1002/mrm.20557
- Pang J, Sharif B, Fan Z, et al. ECG and navigator-free four-dimensional whole-heart coronary MRA for simultaneous visualization of cardiac anatomy and function. Magn Reson Med. 2014;72(5):1208-1217. doi:10.1002/mrm.25450
- Di Sopra L, Piccini D, Coppo S, et al. An automated approach to fully self-gated free-running cardiac and respiratory motion-resolved 5D whole-heart MRI. Magn Reson Med. 2019;82(6):2118-2132. doi:10.1002/mrm.27898
- Jimenez-Juan L, Joshi SB, Wintersperger BJ, et al. Assessment of right ventricular volumes and function using cardiovascular magnetic resonance cine imaging after atrial redirection surgery for complete transposition of the great arteries. Int J Cardiovasc Imaging. 2013;29(2):335-342. doi:10.1007/s10554-012-0083-8
- Tondi L, Badano LP, Figliozzi S, et al. The use of dedicated long-axis views focused on the left atrium improves the accuracy of left atrial volumes and emptying fraction measured by cardiovascular magnetic resonance. J Cardiovasc Magn Reson. 2023;25(1):10. doi:10.1186/s12968-022-00905-w
- Piccini D, Littmann A, Nielles-Vallespin S, et al. Spiral phyllotaxis: the natural way to construct a 3D radial trajectory in MRI. Magn Reson Med. 2011;66(4):1049-1056. doi:10.1002/mrm.22898
- Coppo S, Piccini D, Bonanno G, et al. Free-running 4D whole-heart self-navigated golden angle MRI: Initial results. Magn Reson Med. 2015;74(5):1306-1316. doi:10.1002/mrm.25523
- Kramer CM, Barkhausen J, Bucciarelli-Ducci C, et al. Standardized cardiovascular magnetic resonance imaging (CMR) protocols: 2020 update. J Cardiovasc Magn Reson Off J Soc Cardiovasc Magn Reson. 2020;22(1):17. doi:10.1186/s12968-020-00607-1
Figures
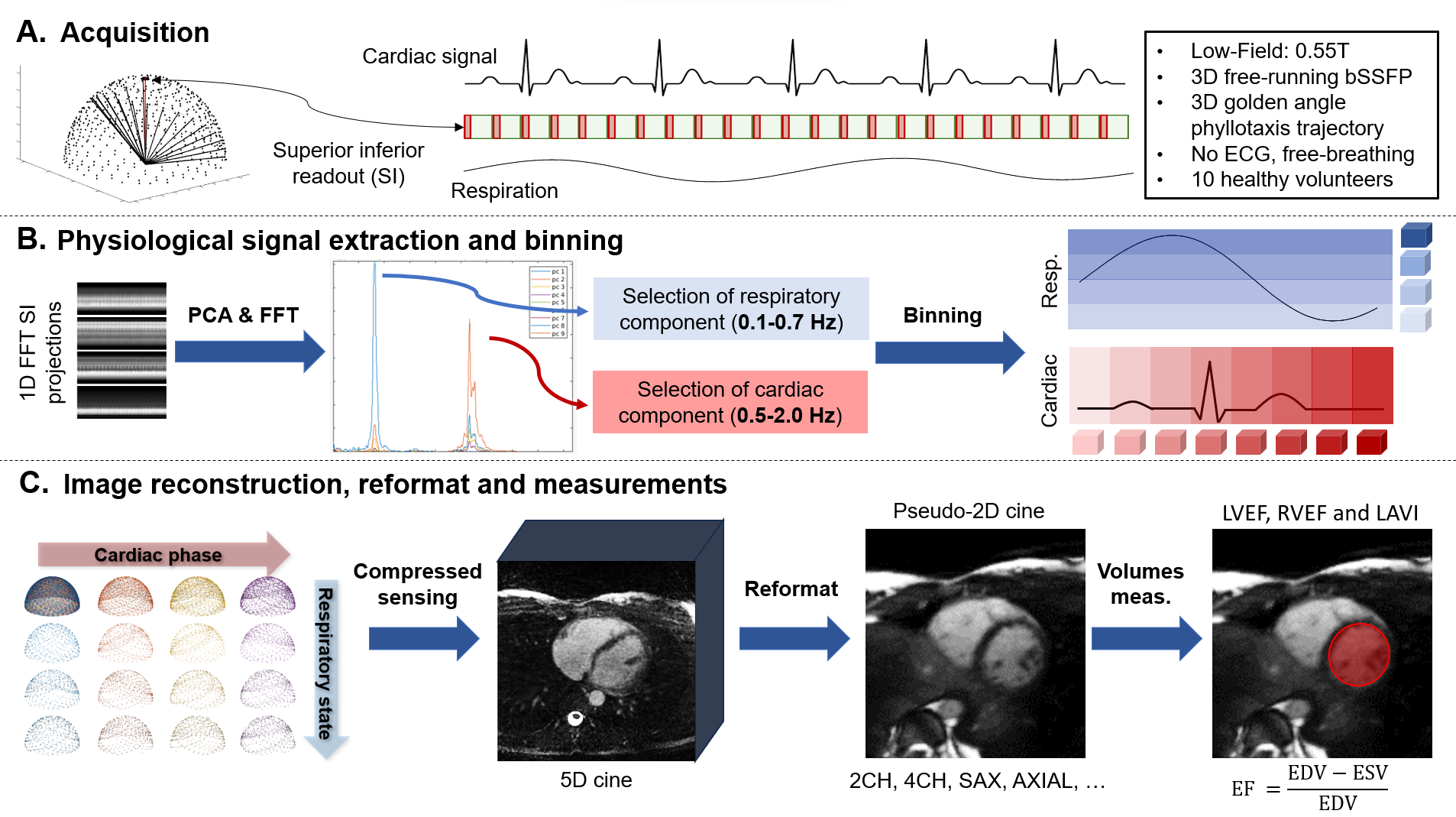
Figure 1: 5D CMR acquisition, reconstruction, and processing schematic. The pulse sequence consists of a segmented 3D radial bSSFP sequence with a phyllotaxis pattern that starts each segment with a superior-inferior (SI) readout for self-navigation purposes. The SIs are extracted, and principal component analysis (PCA) is applied to extract the cardiac and respiratory motion and to bin all readouts accordingly. Lastly, the 5D images are reconstructed and reformatted into 2D cines with 8mm slice thickness on which LV, RV and LA volumes are measured at end systole and end diastole.
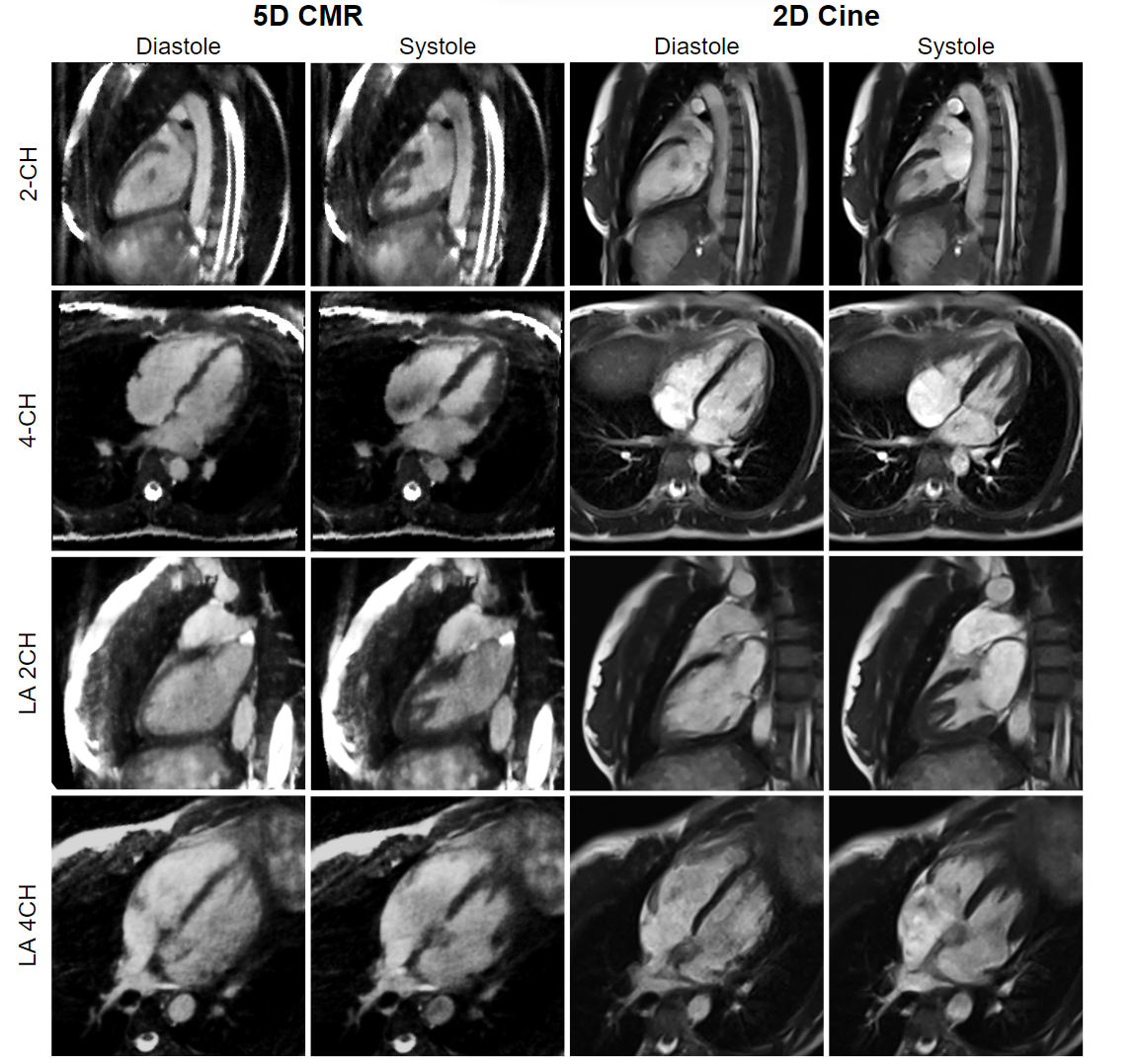
Figure 2: A comparison of ED and ES frames of 5D CMR and 2D cine on volunteer 1. ES and ED images show that the range of motion is similar in both cases. The LA-focused 2-chamber and 4-chamber views display larger volumes in systole when compared to the standard 2-chamber and 4-chamber view.
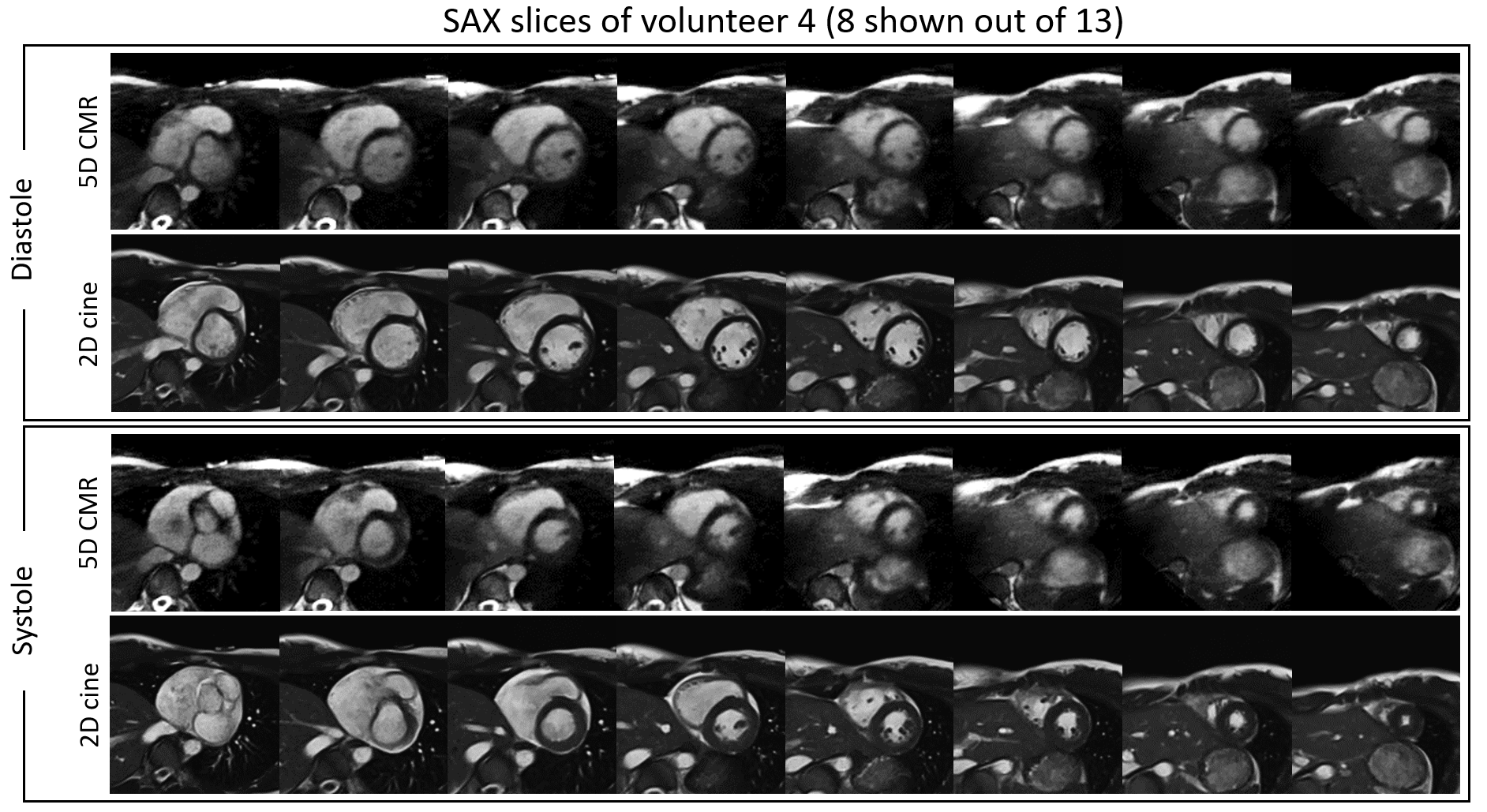
Figure 3: Short axis stack slices in systole and diastole, comparison between the 2D cine and 5D CMR acquisitions without contrast agent. Both the 2D cines and the 5D CMR images show excellent contrast between the blood and the myocardium supporting segmentation of the blood pool of the left and right ventricle.