2671
Simultaneous Contrast-Free 3D Aortic Lumen and Vessel Wall Imaging at 0.55T at systole and diastole1Millennium Institute for Intelligent Healthcare Engineering, Santiago, Chile, 2School of Biomedical Engineering, King's College London, London, United Kingdom, 3Institute for Biological and Medical Engineering, Pontificia Universidad Católica de Chile, Santiago, Chile, 4MR Research Collaborations, Siemens Healthcare Limited, Camberley, United Kingdom, 5School of Engineering, Pontificia Universidad Católica de Chile, Santiago, Chile
Synopsis
Keywords: Low-Field MRI, Low-Field MRI, cardiovascular,aortic imaging
Motivation: Bright-blood and black-blood imaging are relevant for assessing aortic pathologies. Research on aortic imaging at 0.55T which could potentially make MRI more accessible and affordable is scarce.
Goal(s): To evaluate the feasibility of a novel non-contrast enhanced simultaneous bright- and black-blood aorta imaging at 0.55T at systole and diastole.
Approach: Five healthy volunteers were scanned at 0.55T with the proposed accelerated and non-rigid motion-compensated sequence (iT2prep-BOOST). Adiabatic, MLEV4 and MLEV8 T2-preparation pulses were compared.
Results: Good image quality was obtained for simultaneous acquisition of 3D bright- and black-blood aorta imaging at 0.55T at systole and diastole with the proposed iT2prep-BOOST and MLEV8 T2-preparation.
Impact: The proposed approach enables 3D simultaneous bright- and black-blood aorta imaging at 0.55T during a fast free-breathing scan and thus shows promise for the detection of different aortic diseases, potentially making aortic MRI more accessible and affordable.
Introduction
Bright-blood lumen and black-blood vessel wall images have been shown to be clinically useful in the assessment of aortic disease. Currently, both contrasts are acquired in separate scans with different spatial resolution and geometries, leading to long scan times and image misregistration. Recently, a respiratory motion-compensated 3D framework (iT2prep-BOOST) for simultaneous contrast-free aortic lumen and vessel wall imaging was developed at 1.5T1 but not demonstrated for aortic imaging at lower field, which could potentially make MRI more accessible and affordable. Here, we evaluate the feasibility of iT2prep-BOOST at 0.55T for aorta imaging at both systole and diastole. To ensure good quality imaging at systole and high flow and susceptibility regions, we also evaluated the performance of adiabatic, MLEV4 and MLEV8 T2 preparation pulses for aorta imaging in iT2prep-BOOST sequence.Methods
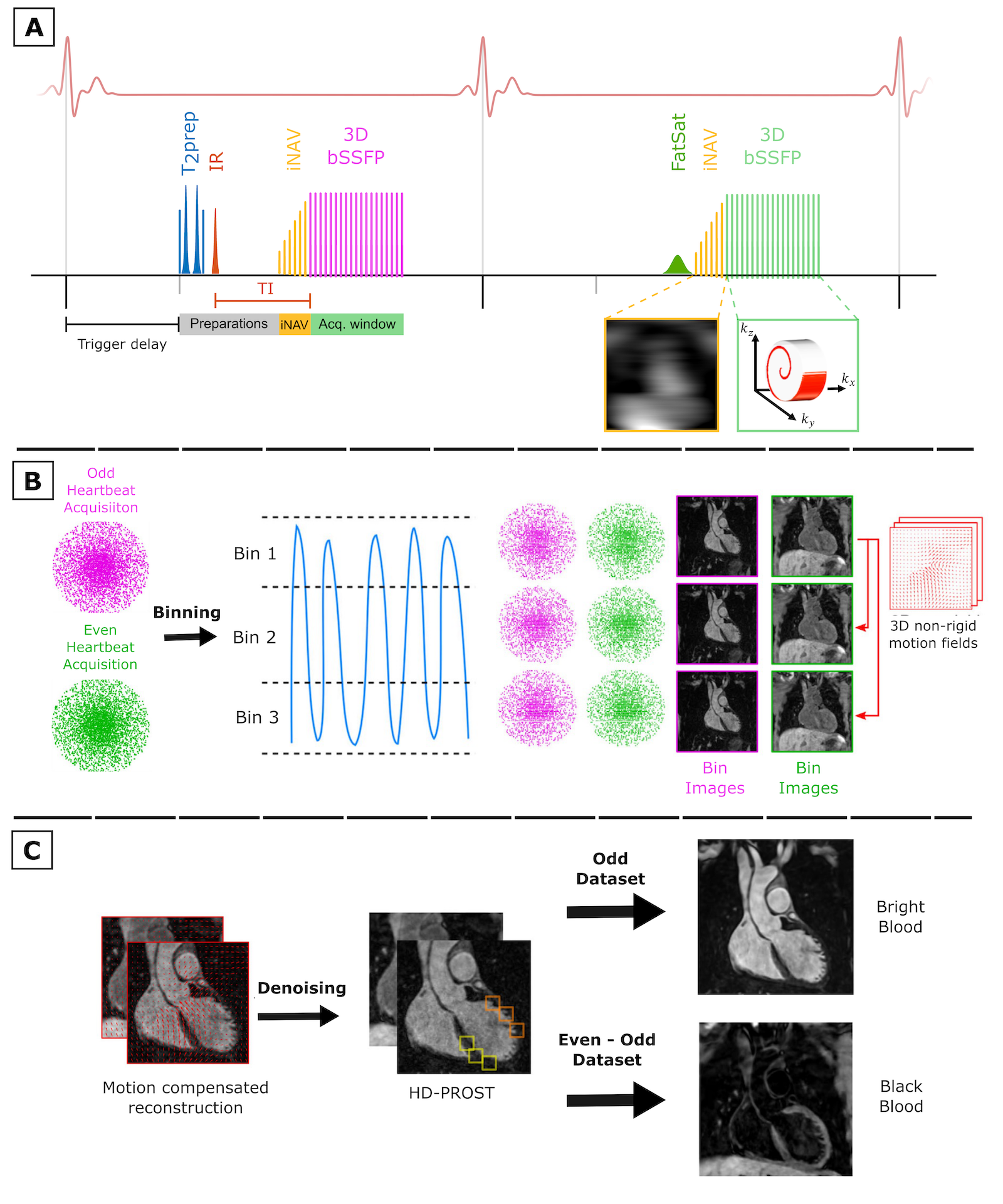
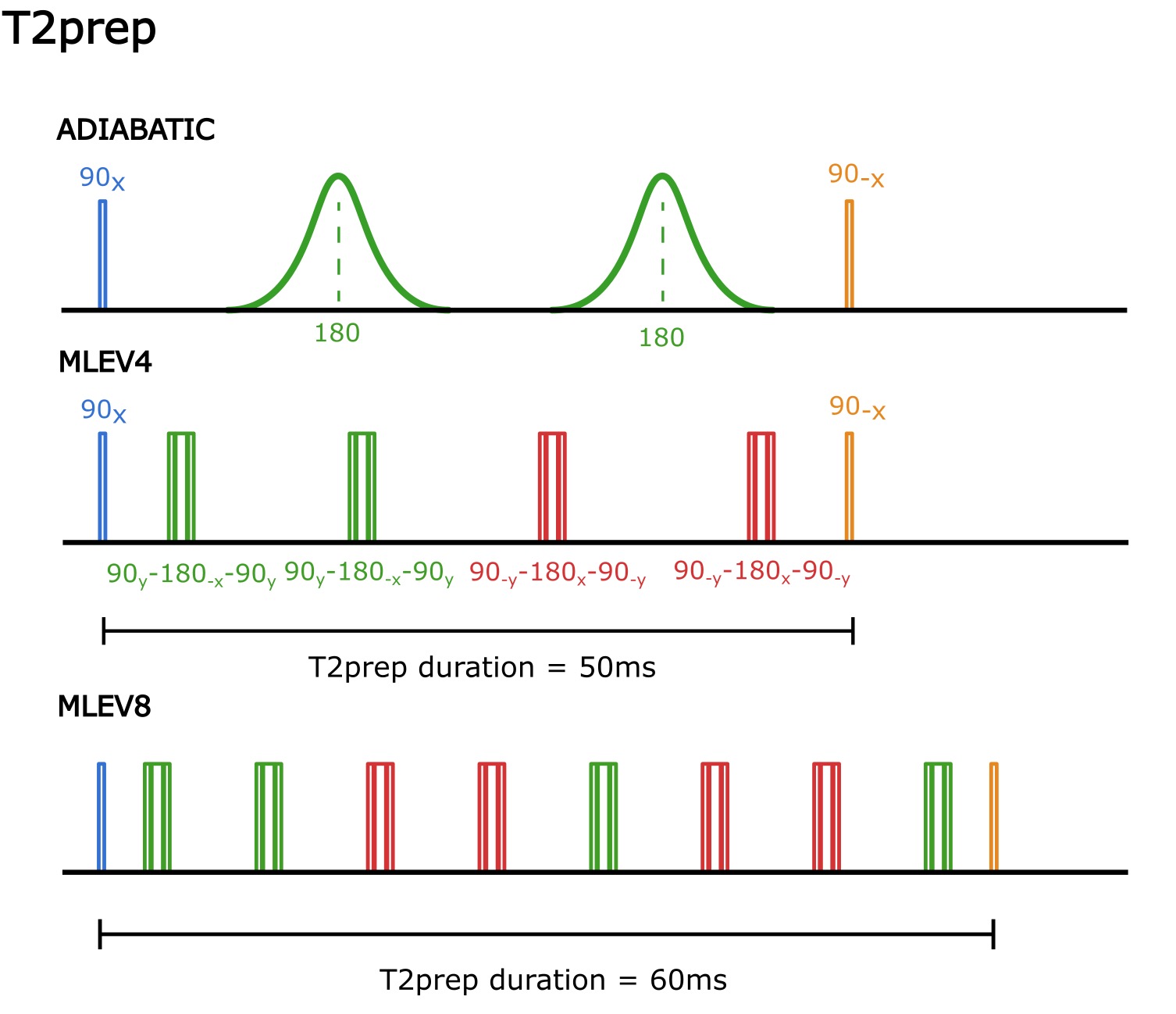
Five healthy volunteers were scanned at 0.55T (MAGNETOM Free.Max, Siemens Healthineers, Erlangen). Three were scanned only at systole for T2 preparation (T2prep) pulses comparison and two were scanned at both systole and diastole using the T2prep pulse that gave the best results (MLEV8). The iT2prep-BOOST framework (Fig. 1) consists of an ECG-triggered free-breathing interleaved 3D bSSFP research sequence with 4-fold undersampled variable-density Cartesian trajectory2, image-based navigation (iNAV)3 for 100% respiratory scan efficiency and non-rigid motion correction followed by HD-PROST denoising4. T2 preparation and inversion recovery preparation pulses are applied in odd heartbeats and no preparation is applied in even heartbeats. The contrast acquired in odd heartbeats is used for lumen visualization, while black-blood contrast is obtained by the direct subtraction between both bright-blood contrasts obtained in each heartbeat. The performance of adiabatic, MLEV4 and MLEV8 refocusing pulses (Fig. 2) was compared at high flow and susceptibility regions. Acquisition parameters include: FOV= 312x312x132 mm, resolution=1.5mm3, flip-angle even heartbeat=110 deg, flip-angle odd heartbeat=80 deg, TR=5.3 ms, TE= 2.65 ms, T2prep duration for MLEV4 and adiabatic pulse=50ms, T2prep duration for MLEV8 = 60ms, TI for MLEV4 and adiabatic preparations pulses=90ms, TI for MLEV8 preparation pulse=85ms , 4x acceleration and a acquisition time = ~7,5 min.Results and Discussion
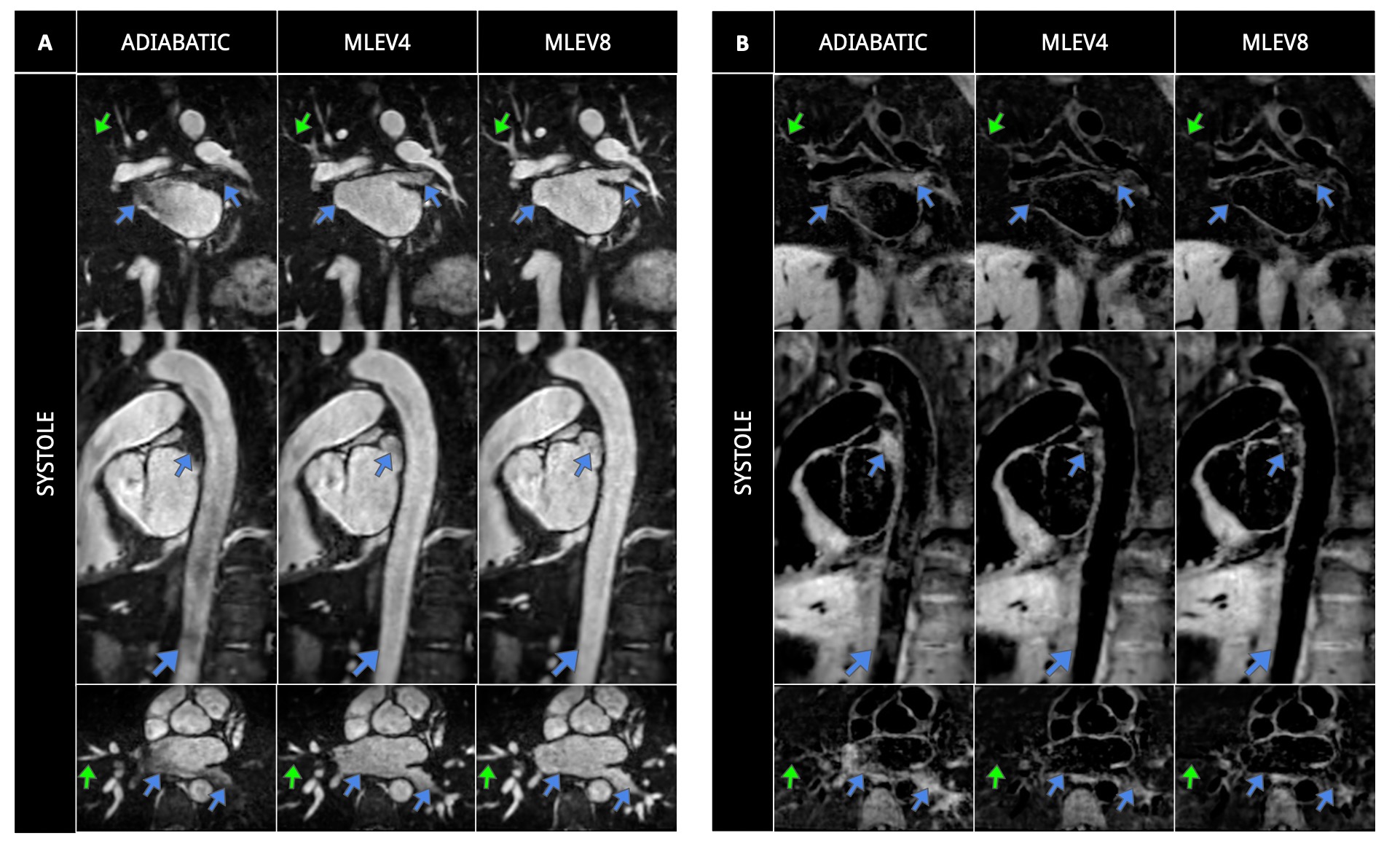
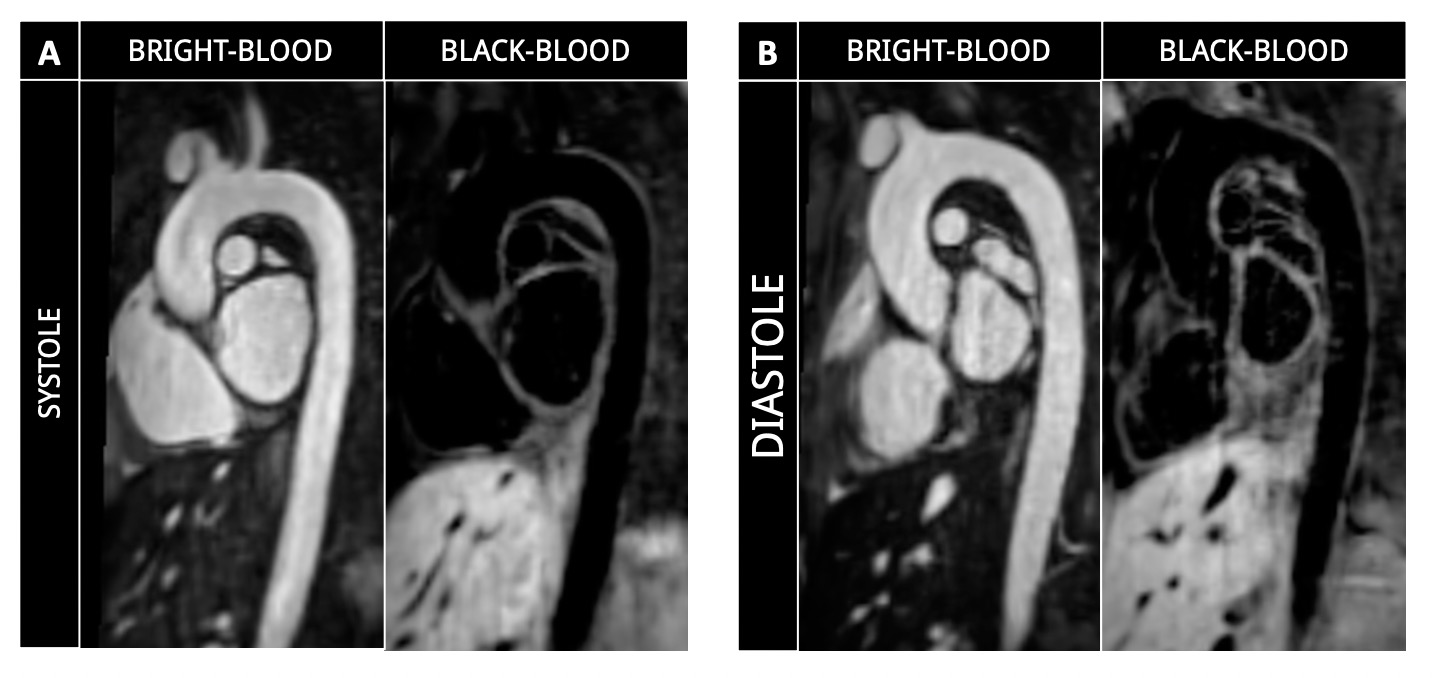
Bright-blood and black-blood images acquired using adiabatic-T2prep, MLEV4-T2prep and MLEV8-T2prep for systole at 0.55T are shown in Fig. 3 for a representative subject. Good image quality can be observed in lumen visualization for the three T2 preparation schemes, with a better signal homogeneity for MLEV4- and MLEV8-T2 preparation, in contrast to the adiabatic preparation pulse which results in signal drops in some areas of the aorta (arrows). This signal loss can also be perceived in the black blood images, causing irregularities in the wall of the aorta due to the subtraction process by which it is obtained. Regarding MLEV pulses, MLEV8-T2prep provides better visualization of small structures and a slightly better signal homogeneity in comparison of MLEV4-T2prep likely caused by the shorter spacing between refocusing pulses which may minimize signal loss due to blood flow. Bright-blood and black-blood images for systole and diastole with the MLEV8-T2prep are shown in Fig. 4 for a second and third volunteer. Good image quality is obtained for both contrasts and cardiac phases despite the decrease in the magnetic field strength. A video going through coronal slices for bright-blood and black blood contrast for a representative subject is shown in Fig. 5.Conclusion
In this work we demonstrate the feasibility of simultaneous acquisition of 3D bright blood and black blood aortic images using a 0.55T contemporary MR scanner. Good image quality was observed for both systole and diastole with MLEV8 T2 preparation. Future work will include evaluation in a larger cohort of healthy volunteers and subjects with aortic disease.Acknowledgements
(1) BHF RG/20/1/34802 (2) EPSRC EP/V044087/1 (3) ANID Millennium Institute iHEALTH, ICN2021_004; Fondecyt 1210637 and 1210638; Fondequip Mayor EQY210003; Basal Funding, IMPACT, FB210024 and (6) the Technical University of Munich – Institute for Advanced Study.References
1. Simultaneous Highly Efficient Contrast-Free Lumen and Vessel Wall MR Imaging for Anatomical Assessment of Aortic Disease. Munoz C, Fotaki A, Hua A, Hajhosseiny R, Kunze KP, Ismail TF, Neji R, Pushparajah K, Botnar RM, Prieto C. J Magn Reson Imaging. 2023 Oct;58(4):1110-1122. doi: 10.1002/jmri.28613.
2. Highly efficient respiratory motion compensated free-breathing coronary MRA using golden-step Cartesian acquisition. Prieto C, Doneva M, Usman M, Henningsson M, Greil G, Schaeffter T, Botnar RM. J Magn Reson Imaging. 2015 Mar;41(3):738-46. doi: 10.1002/jmri.24602.
3. Whole-heart coronary MR angiography with 2D self-navigated image reconstruction. Henningsson M, Koken P, Stehning C, Razavi R, Prieto C, Botnar RM. Magn Reson Med. 2012 Feb;67(2):437-45. doi: 10.1002/mrm.23027.
4. High-dimensionality undersampled patch-based reconstruction (HD-PROST) for accelerated multi-contrast MRI. Bustin A, Lima da Cruz G, Jaubert O, Lopez K, Botnar RM, Prieto C. Magn Reson Med. 2019 Jun;81(6):3705-3719. doi: 10.1002/mrm.27694.
Figures