2666
Using Pilot Tone for Sequence-Independent Motion Detection in the Head1Advanced Clinical Imaging Technology, Siemens Healthineers International AG, Lausanne, Switzerland, 2Diagnostic and Interventional Radiology, University Hospital of Lausanne (CHUV), Lausanne, Switzerland, 3Center for Biomedical Imaging (CIBM), Lausanne, Switzerland, 4Siemens Healthcare GmbH, Erlangen, Germany, 5Siemens Shenzhen Magnetic Resonance Ltd., Shenzhen, China, 6LTS5, École Polytechnique Fédérale de Lausanne (EPFL), Lausanne, Switzerland
Synopsis
Keywords: Motion Correction, Motion Correction, Pilot Tone, Neuro, Motion detection, Artifact
Motivation: Motion artifacts are a major cause for rescans or for the patient to be recalled for another scanning session; this results in patient discomfort, workflow disruptions and additional costs.
Goal(s): Prospectively provide MR operators with a “motion sensor signal” indicating subject motion to assist them in detecting and reacting to motion events.
Approach: Design a sequence-agnostic Pilot Tone processing pipeline to detect motion and predict image quality degradation.
Results: We showed that Pilot Tone can be used to detect head movement and predict with high accuracy whether the resulting image will be usable for diagnosis.
Impact: This work shows that Pilot Tone can be used for prospective motion detection and image degradation prediction. Such a method may lead to a practically applicable solution to improve the MR workflow, thus reducing patient burden and costs.
Introduction
In neuroimaging, motion artifacts are a major cause for rescans or - in the worst case - for the patient to be recalled for another scanning session; this results in patient discomfort, workflow disruptions and additional costs1. For cardiac imaging, the Pilot Tone (PT) method has shown promising results to reliably detect motion2,3 and few studies have demonstrated its potential use for neuro imaging4,5.The PT method uses a small coil to generate a continuous, mono-frequency RF signal which can be continuously received by the scanner’s receive RF chain without interfering with the image acquisition2. It is modulated by conductive materials (e.g., brain tissue) in the vicinity of the transmit/receive coils2 and can thus provide information for the detection and correction of head motion6.
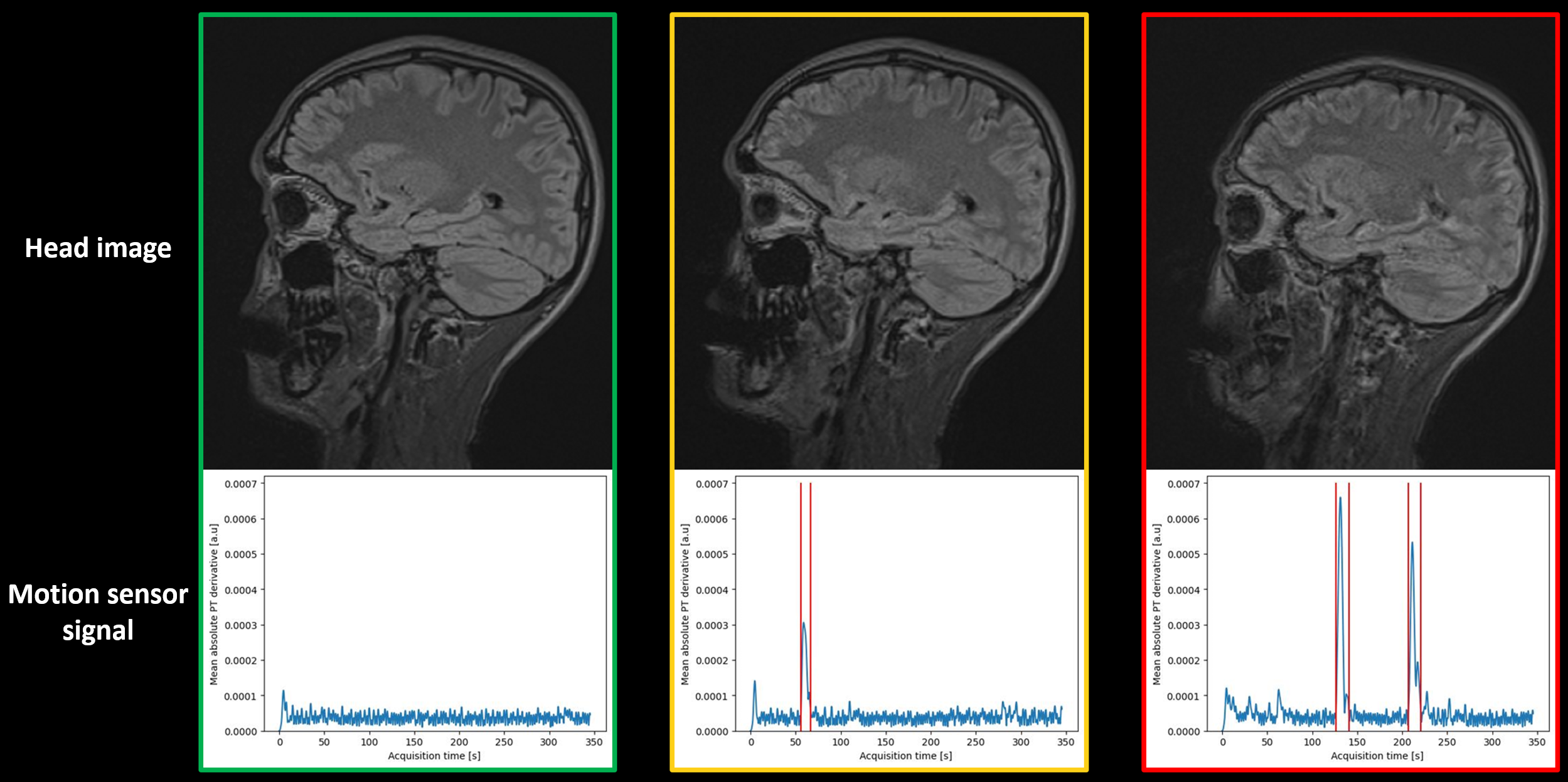
In this work, we propose the use of PT for head motion detection during 3D acquisitions to inform the MR operator in real time about the predicted image quality. To this end, each scan is classified in a traffic light manner: GREEN = no motion artifact, YELLOW = motion but clinically useful, RED = non-diagnostic motion artifacts.
Methods
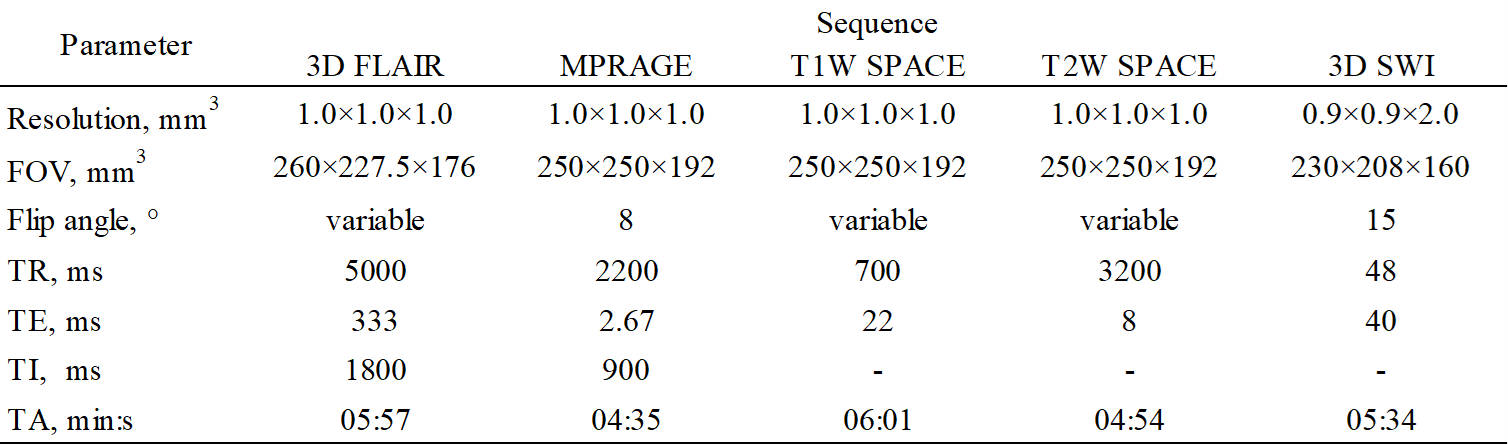
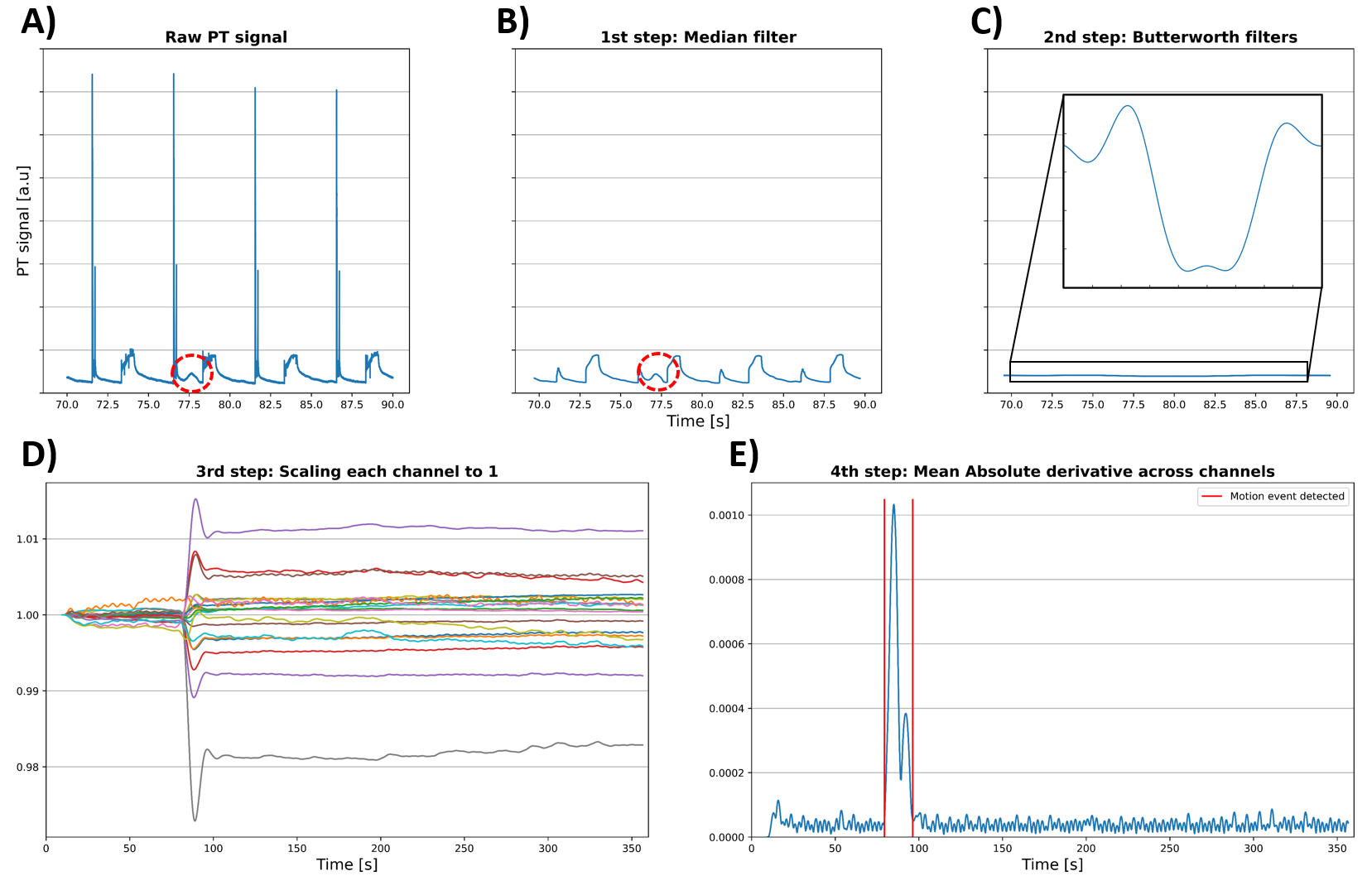
Five volunteers were scanned at 1.5T (MAGNETOM Sola, Siemens Healthcare, Erlangen, Germany) with different sequences typically used in clinical routine (see Table 1). All scans were acquired using the standard 20-channel head/neck coil and research application sequences. The PT signal was generated using the transmitter in a commercially available 12-channel body coil strapped onto the head coil. Each subject underwent multiple sessions of three scans with the same instructions: one scan staying still, followed by scans with one and two bulk movements. The resulting images were labelled (GREEN, YELLOW, RED) by an MR technologist (JBL, 13 years of experience). For each scan, the multi-channel raw PT signal was recorded and processed offline in Python (version 3.9).The PT signal is highly sensitive to RF interferences; the amplitude of these interferences is much higher than the position-dependent modulation (see Figure 1A). To detect motion in the PT signal, the following steps were applied to the magnitude of the recorded signals: first, a 250 ms median filter was applied (Figure1B), followed by two applications of Butterworth lowpass digital filters (Figure 1C). Then, each channel was scaled independently to a mean value of 1, to mitigate inter-subject and inter-scan differences (Figure 1D). Finally, we calculate a “motion sensor signal” by computing the mean of the absolute derivative across channels (Figure 1E).
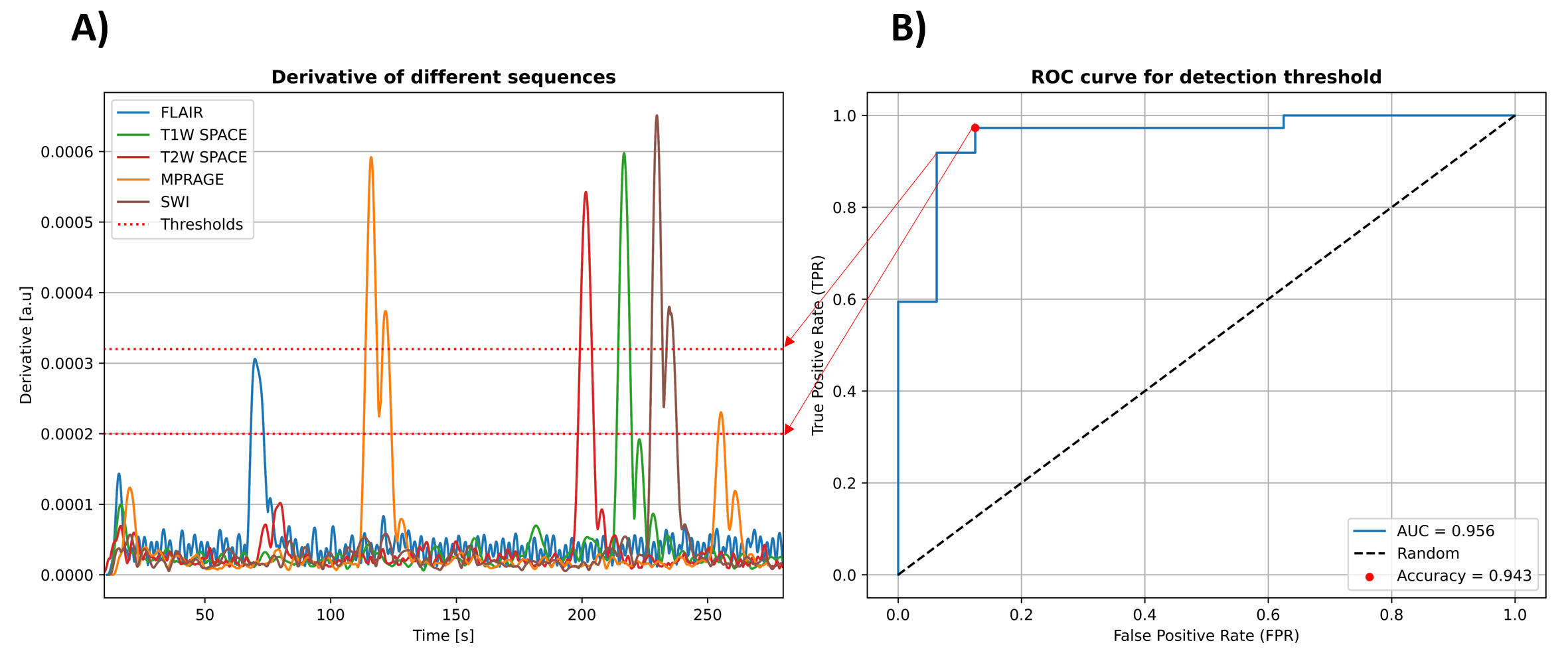
The analysis of the “motion sensor signal” was performed in two steps: first, motion events were detected. Second, the motion event’s impact on the image quality was predicted. Detection is based on a constant threshold: a movement is detected if the “motion sensor signal” exceeds this threshold, otherwise the algorithm labels the image GREEN. A Receiver Operator Curve analysis was performed to optimize the threshold.
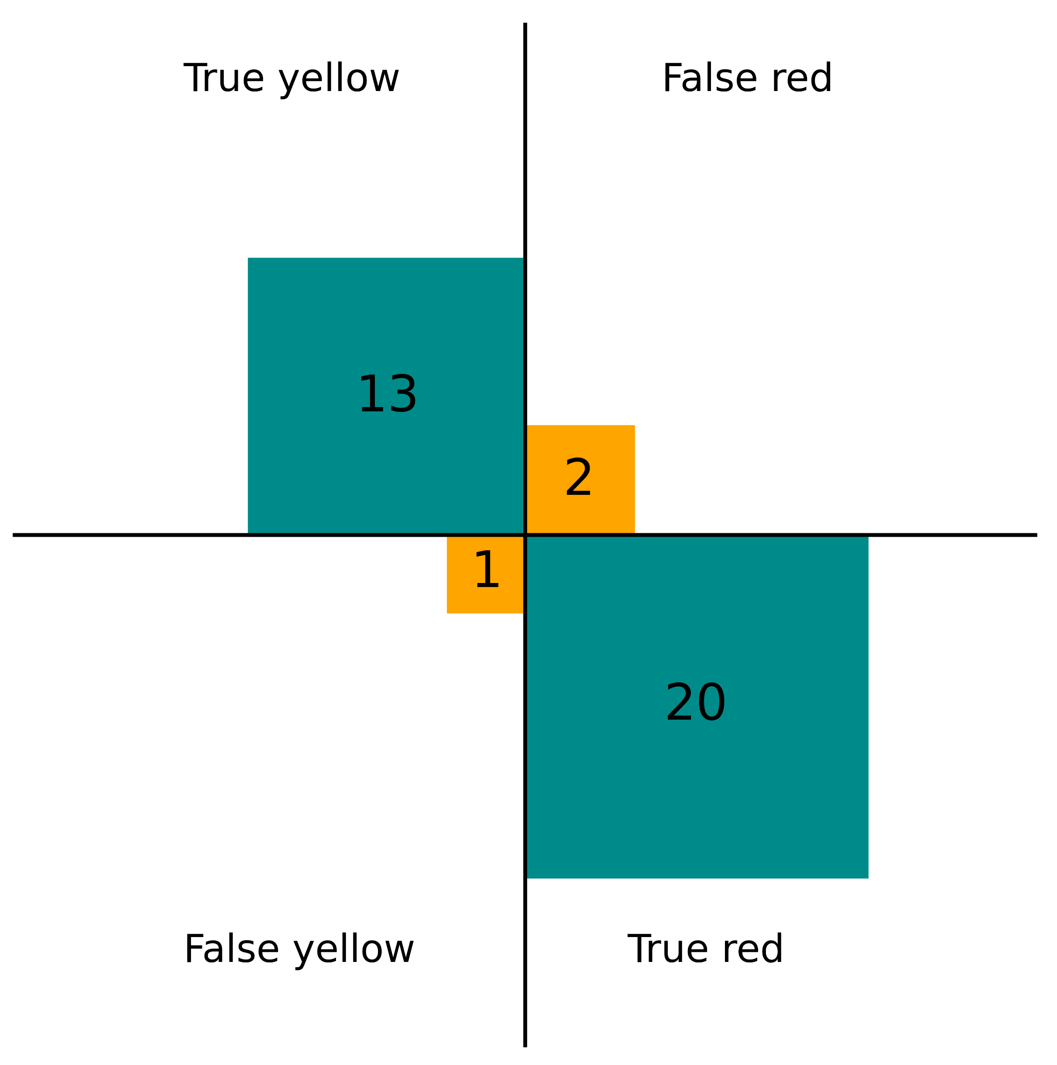
For the model classifying image degradation, i.e., deciding if a motion event will result in a YELLOW or RED label, a Support Vector Machine (SVM) was used with features extracted from the last detected motion event including when the event occurred and the severity of previous events (Figure 3A&B). The performance of the SVM was evaluated by computing the confusion matrix from each scan’s prediction in a Leave-One-Out cross-validation pattern.
Results
The “motion sensor signal” in Figure 2A has the same behavior and amplitude across all sequences for both resting state and motion events. In Figure 2B, the ROC curve (AUC=0.956) shows a good discrimination between scans with and without motion artifacts (3/53 misclassified scans), the optimal threshold for our experiments was found to be 2×10-4 [a.u.]. The SVM model achieved a 92% accuracy in the cross-validation as shown in Figure 3C and example images in Figure 4.Discussion and Conclusion
We showed that the PT can be used to detect head movement, confirming prior work4,5,7. In the limits of this study, our framework predicted with high accuracy whether the resulting image will be usable for diagnosis. This method could be used to directly update the FOV after a severe motion event8, saving precious time in clinical practice.While these results are promising, the method has limited ability to detect slow and continuous motion (e.g., head sinking into pillow), as well as setup-related variations (e.g., PT generator location) which will need further investigation.
In conclusion, our results may lead to a practically applicable and cost-effective solution to warn the MR operator of an image-degrading motion event already during the acquisition, which can save a considerable amount of unnecessary scan time. This improves the MR workflow, thus reducing patient burden and costs.
Acknowledgements
No acknowledgement found.References
1. Andre JB, Bresnahan BW, Mossa-Basha M, Hoff MN, Smith CP, Anzai Y, Cohen WA. Toward Quantifying the Prevalence, Severity, and Cost Associated With Patient Motion During Clinical MR Examinations. J Am Coll Radiol. 2015;12(7):689-95
2. P. Speier, M. Fenchel, and R. Rehner, “PT-Nav: a novel respiratory navigation method for continuous acquisitions based on modulation of a pilot tone in the MR-receiver,” Magn Reson Mater Phys Biol Med, vol. 28, pp. S97–S98, 2015
3. Ludwig J, Speier P, Seifert F, Schaeffter T, Kolbitsch C. Pilot tone-based motion correction for prospective respiratory compensated cardiac cine MRI. Magn Reson Med. 2021;85(5):2403-2416.
4. T.E. Wallace, C. Ariyurek, F. Calakli, T. Kober, S.K. Warfield, and O. Afacan, “High Temporal Resolution Head Motion Tracking using Pilot Tone and 3D Radials” in ISMRM Meeting and Exhibition Abstract 2023.
5. N.R.F. Huttinga, S. Anand, C.A.T. van den Berg, A. Sbrizzi, and M. Lustig, “Three-dimensional rigid head motion correction using the Beat Pilot Tone and Gaussian Processes” in ISMRM Meeting and Exhibition Abstract 2023.
6. P. Speier, M. Bacher, J. Bollenbeck, M. Fenchel and T. Kober, “Separation And Quantification Of Head Motion Modes By Pilot Tone Measurements” in ISMRM Meeting and Exhibition Abstract 2018.
7. Y. Brackenier, T. Wilkinson, L. Cordero-Grande, R. Tomi-Tricot, P. Bridgen, S. Giles, E. De Vita, S.J. Malik, and J.V. Hajnal, “Pilot Tone meets DISORDER: Improved data-driven motion-corrected brain MRI by leveraging Pilot Tone signal variations” in ISMRM Meeting and Exhibition Abstract 2022.
8. Tisdall, M.D., Hess, A.T., Reuter, M., Meintjes, E.M., Fischl, B. and van der Kouwe, A.J.W., Volumetric navigators for prospective motion correction and selective reacquisition in neuroanatomical MRI. Magnetic Resonance Medicine, 68: 389-399.
Figures