2656
Deep learning based assessment of diagnostic image quality from Free Induction Decay Navigators1Department of Radiology, Boston Children's Hospital and Harvard Medical School, Boston, MA, United States, 2Siemens Medical Solutions, Boston, MA, United States, 3Advanced Clinical Imaging Technology, Siemens Healthineers International AG, Lausanne, Switzerland, 4Radiology, Lausanne University Hospital and University of Lausanne, Lausanne, Switzerland, 5LTS5, Ecole Polytechnique Fédérale de Lausanne, Lausanne, Switzerland, 6Department of Radiology, Massachusetts General Hospital and Harvard Medical School, Boston, MA, United States
Synopsis
Keywords: Motion Correction, Data Acquisition
Motivation: Motion-induced artifacts in pediatric MRI lead to frequent need for rescan, which increases examination time, costs and patient's discomfort.
Goal(s): To develop and validate a deep learning-based method for automated assessment of diagnostic image quality, overcoming limitations of existing motion measurement techniques.
Approach: FID navigators embedded into MPRAGE sequence can provide valuable motion information without prolonging scan time. We train a deep neural network on these signals to accurately predict the diagnostic quality of the image that is to be reconstructed.
Results: Our method surpasses the existing FIDnavΔ approach, achieving AUC of 0.90, with 30% higher specificity and 21% improved precision.
Impact: Our model streamlines MRI procedures by accurately predicting the need for rescans due to patient motion. It has potential to reduce healthcare costs and patient discomfort, and opens new avenues for early scan termination and enhanced clinical workflow efficiency.
Introduction
Pediatric MRI patient motion leads to image artifacts like ghosting, ringing, and blurring, which makes it challenging for radiological interpretation. A rescan is often required which increases the examination time, costs and patient's discomfort. The frequency of sequence repetitions due to movement is estimated to be around 20% [1]. Information about the degree of patient motion, as well as automated image quality assessment, can assist technologists in making optimal decisions regarding the need to repeat the scan.External tracking systems [2][3] provide motion measurements but can be challenging to set up and may disrupt workflow. Gradient based MRI navigators circumvent this issue but prolong the scan time [4][5]. Free induction decay navigators (FIDnavs) [6-8] can be integrated into most sequences, with a minimal effect on the acquisition and have been shown to encode valuable motion information.
Prior work by Wallace et al. showed that a simple cross correlation based classifier on preprocessed FIDnav signals can be a valuable tool for grading diagnostic quality of the images based on severity of motion during acquisition [6][7][8]. However, the setup needs manual threshold allocation for each subject, challenging in clinics. Instead, we introduce a deep neural network that utilizes data from FIDnavigators from many subjects to train a classifier of the motion grade and thus could provide the likelihood of an image being of diagnostic quality. We compare our method to previously published work of Wallace et al [8].
Method
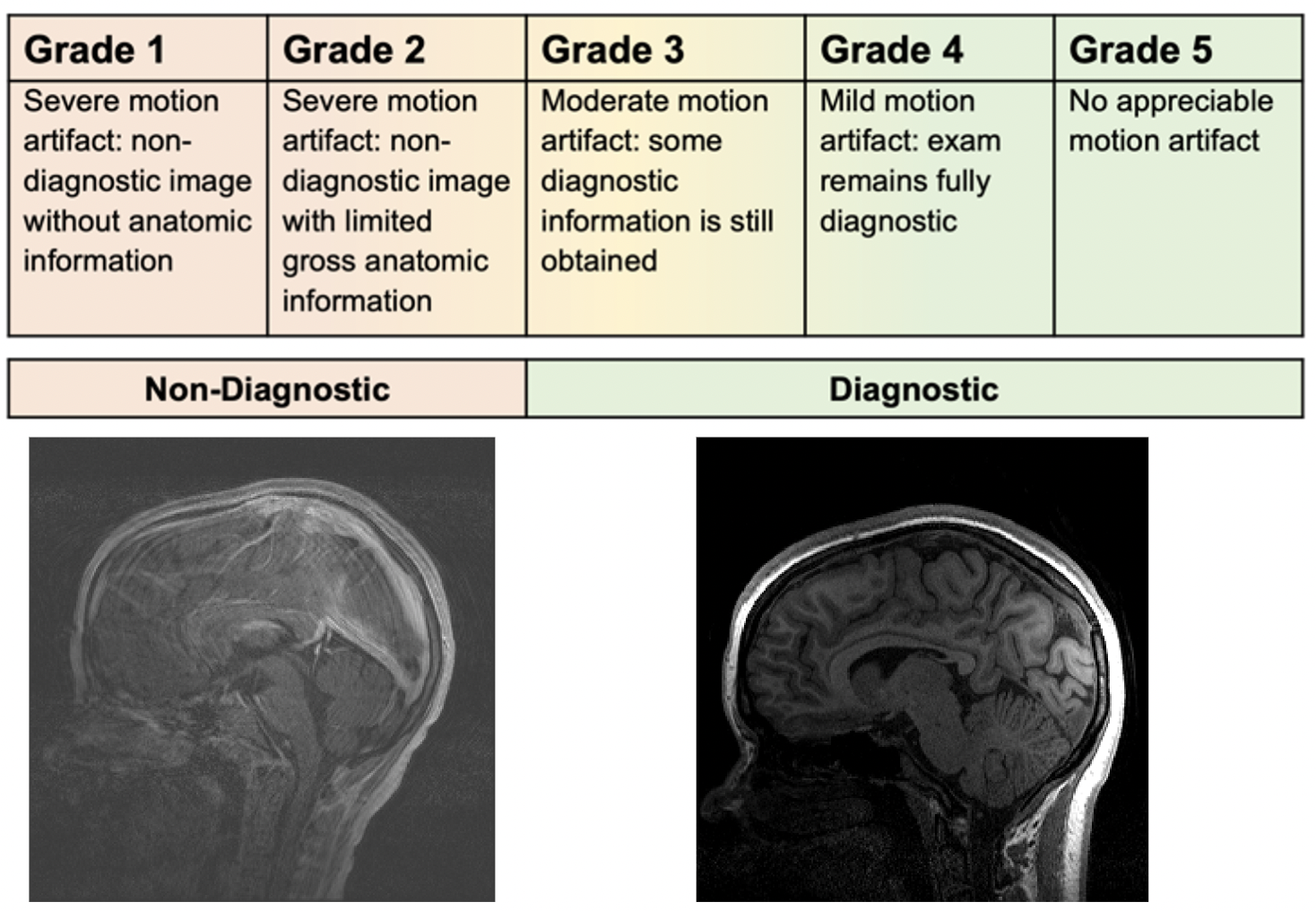
DataData from 90 pediatric subjects (age 13.4±5.1 years) was acquired using FIDnav integrated T1W MPRAGE sequence on a 3T scanner (MAGNETOM Trio, A Tim System; Siemens, Erlangen, Germany) with a 32-channel head coil. Acquisition parameters were: TR 1540 ms, TI 800 ms, TE 2.47 ms, flip angle 9°, FOV 220 × 220 × 152 mm, resolution 0.9 mm isotropic, GRAPPA acceleration 2, and total acquisition time 4.2 minutes. A Cartesian sampling trajectory was used with a sagittal acquisition plane. FIDnavs, embedded with a 0.2ms increase in minimum TE, did not affect overall acquisition time, thanks to the large dead time in MPRAGE scans. Reconstructed images were assessed by two trained licensed radiologists on a five point Likert scale to evaluate their diagnostic quality (as described in Figure 3),, and motion score was assigned respectively to each.
Network Architecture
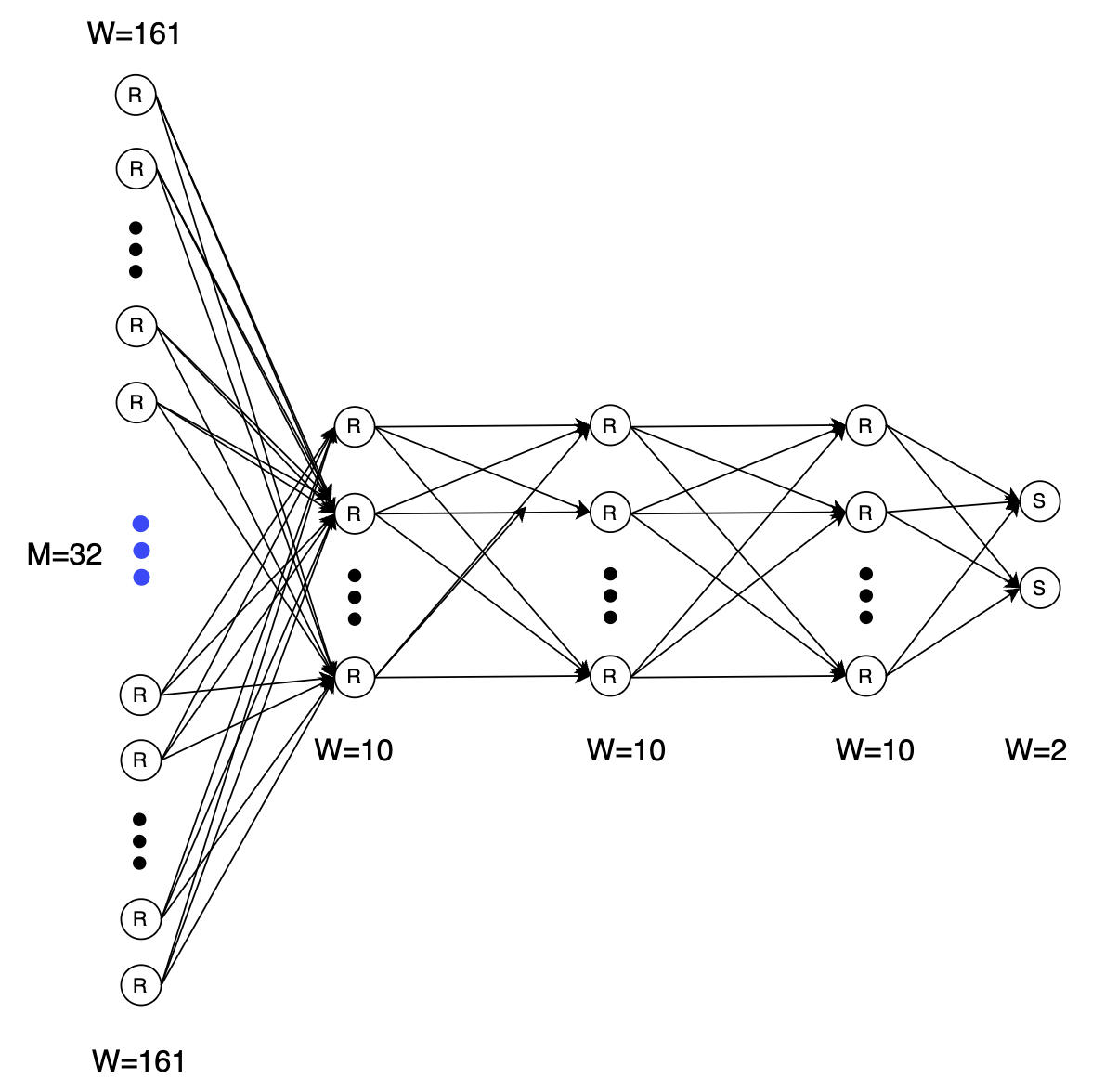
We designed a deep neural network that learns the mapping between multi-channel complex FID navigator signals and diagnostic image quality scores that were assigned by a trained radiologist using a score based system for the training data (Figure 1). The network consists of parallel fully connected layers, with ReLU activation in hidden layers and sigmoid in the output.(Figure 2).
Pre-processing
We processed complex FID signals from all channels with N timepoints by 1) taking only the absolute part of the complex signal to eliminate the effect of phase shifts 2) removing the DC component of the signal to suppress the receiver gain effects by subtracting the mean of the first three measurements as a reference measure. The data was further augmented by flipping the time courses, which does not alter the labels assuming k-space energy is symmetric.
Training
The proposed network architecture was used on a clinical dataset of 90 subjects. It was split into 81 training and 9 validation subjects with 3 permutations, randomizing indices. Each dataset was ensured to be class-balanced. Training was performed with 9-fold cross-validation, resulting in a total of 27 independent training runs. The network was trained for 10,000 epochs with early stopping based on validation loss with patience of 400. We used the Adam optimizer with a learning rate of 0.0001 and a batch size of 81. Hyperparameters and network architecture were selected via a grid search, optimizing for validation accuracy. Dropout was tested but did not improve performance.
Results
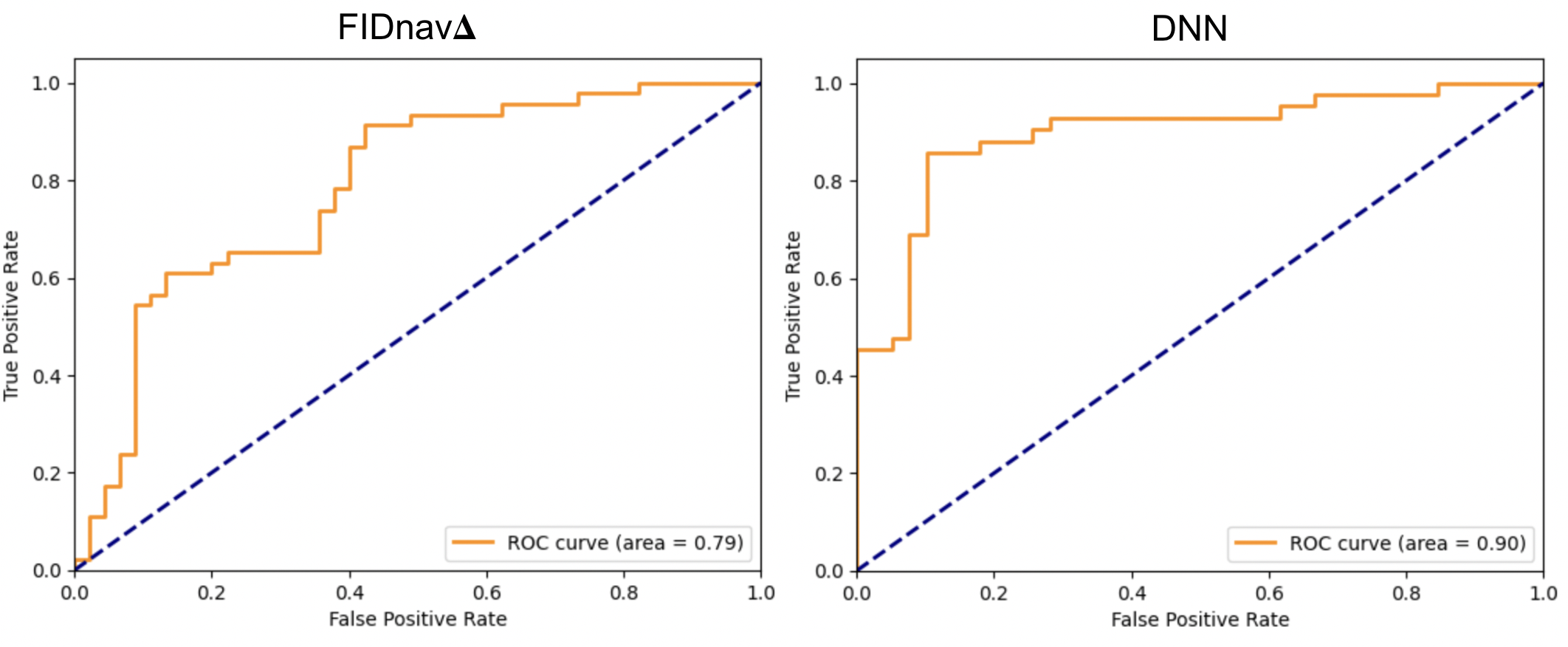
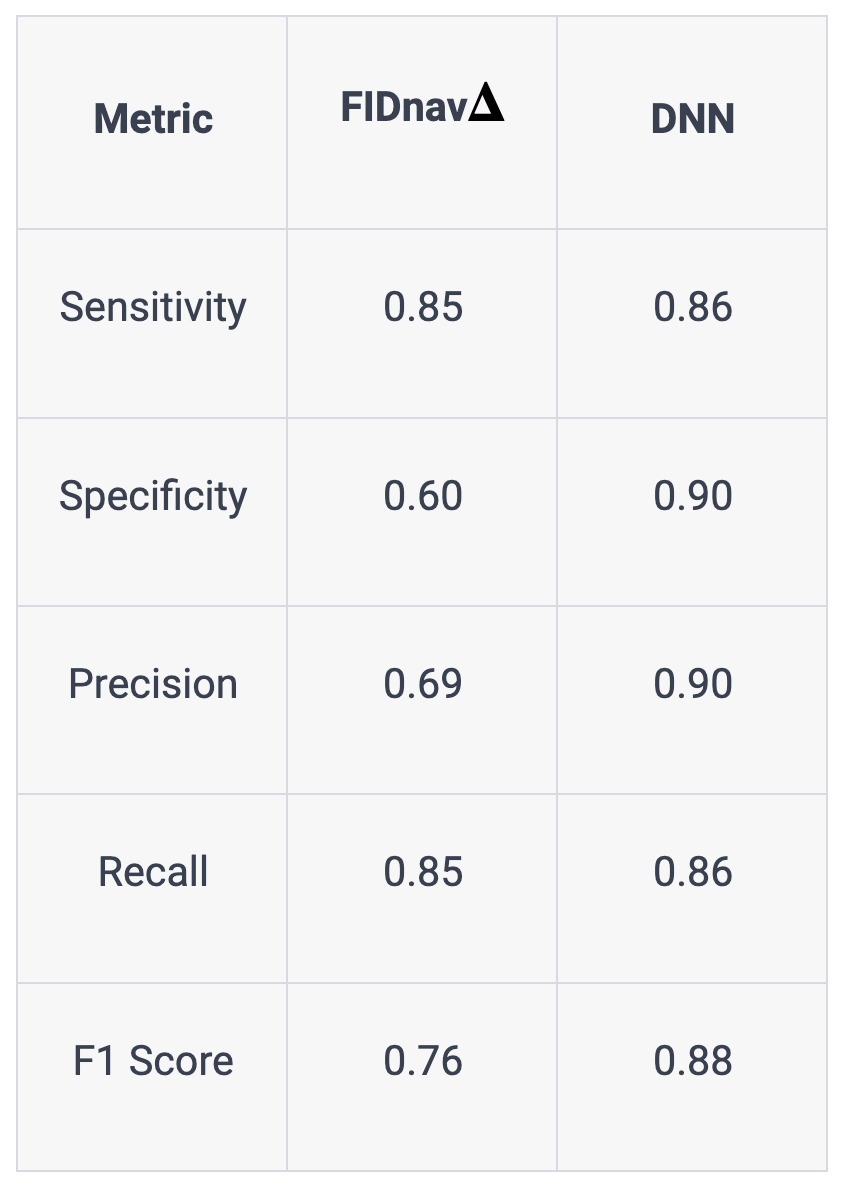
In the ROC curve analysis (Figure 4), the FIDnav𝚫 method [8] achieved a moderate diagnostic AUC of 0.79. The DNN method showed superior performance with an AUC of 0.90, indicating better efficacy in differentiating diagnostic image quality. Comparison shows the DNN method outperforms FIDnav𝚫, with 30% better specificity and 21% improved precision. Additionally, there's a marginal increase in sensitivity and recall (both by 1%), and a notable 12% enhancement in the F1 score. These outcomes highlight the DNN method's advanced capability in classifying FID signals for MRI image quality assessment.Discussion
Our study demonstrates integrated FID signals' potential in differentiating diagnostics, reducing costs. Future work will investigate estimation of diagnostic quality from smaller sets of data which can open the possibility of early stopping of scans.Acknowledgements
This work was supported partially by the National Institute of Diabetic and Digestive and Kidney Diseases (NIDDK), National Institute of Biomedical Imaging and Bioengineering (NIBIB), National Institute of Neurological Disorders and Stroke (NINDS) and National Library of Medicine (NLM) of the National Institutes of Health under award numbers R01DK125561, R21DK123569, R21EB029627, R01NS121657, R01 EB019483, S10OD0250111.References
[1] Andre, J.B., Bresnahan, B.W., Mossa-Basha, M., Hoff, M.N., Smith, C.P., Anzai, Y. and Cohen, W.A., 2015. Toward quantifying the prevalence, severity, and cost associated with patient motion during clinical MR examinations. Journal of the American College of Radiology, 12(7), pp.689-695
[2] Qin, L., van Gelderen, P., Derbyshire, J.A., Jin, F., Lee, J., de Zwart, J.A., Tao, Y. and Duyn, J.H., 2009. Prospective head‐movement correction for high‐resolution MRI using an in‐bore optical tracking system. Magnetic Resonance in Medicine: An Official Journal of the International Society for Magnetic Resonance in Medicine, 62(4), pp.924-934
[3] Afacan, O., Wallace, T.E. and Warfield, S.K., 2020. Retrospective correction of head motion using measurements from an electromagnetic tracker. Magnetic resonance in medicine, 83(2), pp.427-437
[4] White, N., Roddey, C., Shankaranarayanan, A., Han, E., Rettmann, D., Santos, J., Kuperman, J. and Dale, A., 2010. PROMO: real‐time prospective motion correction in MRI using image‐based tracking. Magnetic Resonance in Medicine: An Official Journal of the International Society for Magnetic Resonance in Medicine, 63(1), pp.91-105
[5] Tisdall, M.D., Hess, A.T., Reuter, M., Meintjes, E.M., Fischl, B. and van der Kouwe, A.J., 2012. Volumetric navigators for prospective motion correction and selective reacquisition in neuroanatomical MRI. Magnetic resonance in medicine, 68(2), pp.389-399
[6] Kober, T., Marques, J.P., Gruetter, R. and Krueger, G., 2011. Head motion detection using FID navigators. Magnetic resonance in medicine, 66(1), pp.135-143
[7] Wallace, T.E., Afacan, O., Waszak, M., Kober, T. and Warfield, S.K., 2019. Head motion measurement and correction using FID navigators. Magnetic resonance in medicine, 81(1), pp.258-274
[8] Wallace, T.E., Afacan, O., Jaimes, C., Rispoli, J., Pelkola, K., Dugan, M., Kober, T. and Warfield, S.K., 2021. Free induction decay navigator motion metrics for prediction of diagnostic image quality in pediatric MRI. Magnetic resonance in medicine, 85(6), pp.3169-3181
[9] A. Paszke et al., "PyTorch: An imperative style, high-performance deep learning library," in Advances in Neural Information Processing Systems 32, 2019.
Figures