2648
Comparison of data-driven approaches for gradient delay corrections in PDFF mapping using a radial stack-of-stars acquisition1School of Medicine and Health, Technical University of Munich, Munich, Germany, 2Philips Healthcare, Best, Netherlands, 3Philips GmbH Market DACH, Hamburg, Germany
Synopsis
Keywords: Artifacts, System Imperfections: Measurement & Correction, Fat & Fat/Water Separation
Motivation: Data-driven eddy current compensation would allow corrections to be performed retroactively on scanned data without the need for calibration scans or direct measurements during the scan.
Goal(s): This work aims to evaluate data-based eddy current correction techniques for self-gated free-breathing radial SOS sequences in the liver.
Approach: PDFF liver maps were obtained using free-breathing radial SoS scans from four volunteers and the eddy current corrected results were compared to a clinically established breath-hold cartesian sequence.
Results: Data-driven eddy current corrections improve PDFF map homogeneity for radial SoS sequences with the RING method outperforming the spoke alignment.
Impact: Prior studies analyzed various data-driven eddy current corrections in radial imaging, but never quantitatively assessed in vivo PDFF maps. This work is the first to apply multiple data-driven correction techniques in vivo, comparing them to clinically established breath-hold cartesian sequences.
Introduction
Spatial encoding gradients in MRI are affected by imperfections introducing a linear phase in image space affecting phase sensitive information such as proton density fat fraction (PDFF) mapping1,2. This is crucial for non-cartesian trajectories, which are a viable competitor to Cartesian sequences for PDFF mapping due to higher motion and undersampling robustness.Calibration scans either during the scan or using a prior reference phantom are not routinely available on clinical scanners yet3-6. Another approach measures the shifts directly during the scan using expensive NMR probes7,8.
In contrast, data-based approaches enable retrospective data correction independent of prior knowledge of the imaging data. This work compares the performance of a spoke alignment method7 and the RING9,10 to correct gradient delays in PDFF mapping using a radial 6 echo stack-of-stars (SoS) sequence to clinically used Cartesian breath-hold PDFF scans.
Methods
Proposed reconstruction pipelineThe reconstruction pipeline yields PDFF maps for a 6 echo SoS free-breathing acquisition (Fig.1). The acquisition is binned into five motion states using principal component analysis (PCA)11.
The RING correction9 is performed for the first motion state, per echo and exclusively for the central slice. The correction calculates a 2x2 shift matrix S describing the 2D trajectory shifts due to gradient delays for each echo, which is then included for the individual trajectories $$$r_{θ_i}$$$:
$$r_{\theta_i} = S \hat n_{\theta_i} + r_{\theta_{i0}}$$
The RING method is compared to a spoke alignment method performed before the self-navigated reconstruction which selects two opposite spokes and aligns both by computing the linear phase minimizing the residual of the subtracted coil-combined magnitude k-space profiles2.
Afterwards, for all methods, coil sensitivities are computed using ESPIRiT12 and an iterative reconstruction in Julia is performed. Water-fat separation is then performed using a hierarchical multi-resolution Graph-cut13 and employing a multi-peak fat model with a single T2* decay. Only the first motion state is used subsequently for PDFF mapping.
Scan protocol
Liver data was acquired on a 3T (Ingenia Elition X Philips Healthcare) with a free-breathing 6 echo radial SoS sequence (FA=3°, TR/TE1/∆TE=7.3/1.13/0.9ms, FOV=450x450x240mm3, voxel size=2x2x5mm3, 347 spokes per slice, scan time=3min) in four volunteers. An additional respiratory-gated scan was performed for volunteer 1 using the Vital Eye (7mm gating window in FH). For volunteer 2, 3 and 4 a Cartesian 6-echo breath-hold reference scan was performed with a similar FOV and voxel size (scan time=18s, CS-Sense reduction 4). The reference PDFF was determined using the vendor’s PDFF quantification algorithm.
Results
Fig.2 shows PDFF maps of the respiratory-gated 6 echo SoS scan, showing improved PDFF homogeneity for both proposed gradient delay corrections.Fig.3 shows a free-breathing 6 echo SoS scan of volunteer 1. PDFF map homogeneity improves significantly after using self-navigation and even more after performing a gradient delay correction. A self-navigated dataset corrected by RING performed the best.
In Fig.4, there is no change in PDFF map quality whether all data or only the first motion state's data is used for the RING correction.
Fig.5 shows the PDFF SoS scan results for three more volunteers and a comparison to the Cartesian breath-hold scan. For all volunteers, the RING method improves PDFF homogeneity compared to the spoke alignment method. For volunteer 2 both correction techniques provide smaller PDFF values than the reference. Quantitative measurements of the PDFF in six different ROIs show good correlation to Cartesian PDFF maps for both radial correction techniques.
Discussion
The results prove the need for both motion-resolved reconstruction techniques and gradient delay correction methods for motion affected areas such as the liver. Though non-cartesian trajectories are inherently more motion robust, it still needs to be accounted for14,15. Comparing the RING and spoke alignment method more homogeneous PDFF images of the RING method are observed. This could be caused by the motion sensitivity of the spoke alignment method, where all spokes of all motion states are used for the correction. The RING method is applicable to a very low number of spokes and, hence, can be used in combination with motion gating to only use data unaffected by motion. However, the current results show no significant changes in the RING performance even when data of multiple motion states is used. This may be caused by a relatively uniform breathing pattern. Future studies will need to address the RING performance for different breathing patterns.Conclusion
This work shows the feasibility of data-driven approaches in correcting gradient delay errors in free-breathing PDFF mapping based on radial SoS acquisitions. In particular, the RING method has been shown to be a viable candidate for homogeneous free-breathing liver PDFF mapping based on radial SoS acquisitions.Acknowledgements
The present research was supported by the German Research Foundation (project number 455422993/FOR5298-iMAGO-P1). The authors also acknowledge research support from Philips Healthcare.References
1. Yu H, Shimakawa A, McKenzie CA, Lu W, Reeder SB, Hinks RS, Brittain JH. Phase and amplitude correction for multi-echo water-fat separation with bipolar acquisitions. J Magn Reson Imaging. 2010 May;31(5):1264-71. doi: 10.1002/jmri.22111. PMID: 20432366; PMCID: PMC3130740.
2. Ruschke S, Eggers H, Kooijman H, Diefenbach MN, Baum T, Haase A, Rummeny EJ, Hu HH, Karampinos DC. Correction of phase errors in quantitative water-fat imaging using a monopolar time-interleaved multi-echo gradient echo sequence. Magn Reson Med. 2017 Sep;78(3):984-996. doi: 10.1002/mrm.26485. Epub 2016 Oct 31. PMID: 27797100.
3. Mason GF, Harshbarger T, Hetherington HP, Zhang Y, Pohost GM, Twieg DB. A method to measure arbitrary k-space trajectories for rapid MR imaging. Magn Reson Med. 1997 Sep;38(3):492-6. doi: 10.1002/mrm.1910380318. PMID: 9339451.
4. Duyn JH, Yang Y, Frank JA, van der Veen JW. Simple correction method for k-space trajectory deviations in MRI. J Magn Reson. 1998 May;132(1):150-3. doi: 10.1006/jmre.1998.1396. PMID: 9615415.
5. Kronthaler S, Rahmer J, Börnert P, Makowski MR, Schwaiger BJ, Gersing AS, Karampinos DC. Trajectory correction based on the gradient impulse response function improves high-resolution UTE imaging of the musculoskeletal system. Magn Reson Med. 2021 Apr;85(4):2001-2015. doi: 10.1002/mrm.28566. Epub 2020 Nov 30. PMID: 33251655.
6. Armstrong T, Dregely I, Stemmer A, Han F, Natsuaki Y, Sung K, Wu HH. Free-breathing liver fat quantification using a multiecho 3D stack-of-radial technique. Magn Reson Med. 2018 Jan;79(1):370-382. doi: 10.1002/mrm.26693. Epub 2017 Apr 16. PMID: 28419582; PMCID: PMC5837283.
7. De Zanche N, Barmet C, Nordmeyer-Massner JA, Pruessmann KP. NMR probes for measuring magnetic fields and field dynamics in MR systems. Magn Reson Med. 2008 Jul;60(1):176-86. doi: 10.1002/mrm.21624. PMID: 18581363.
8. Dietrich, B.E., Brunner, D.O., Wilm, B.J., Barmet, C., Gross, S., Kasper, L., Haeberlin, M., Schmid, T., Vannesjo, S.J. and Pruessmann, K.P. (2016), A field camera for MR sequence monitoring and system analysis. Magn. Reson. Med., 75: 1831-1840. https://doi.org/10.1002/mrm.25770
9. Rosenzweig, S, Holme, HCM, Uecker, M. Simple auto-calibrated gradient delay estimation from few spokes using Radial Intersections (RING). Magn Reson Med. 2019; 81: 1898–1906. https://doi.org/10.1002/mrm.27506
10. BART Toolbox for Computational Magnetic Resonance Imaging, DOI: 10.5281/zenodo.592960
11. Rosenzweig S, Scholand N, Holme HCM, Uecker M. Cardiac and Respiratory Self-Gating in Radial MRI Using an Adapted Singular Spectrum Analysis (SSA-FARY). IEEE Transactions on Medical Imaging 2020; 39:3029–3041. 10.1109/tmi.2020.2985994.
12. Uecker M, Lai P, Murphy MJ, Virtue P, Elad M, Pauly JM, Vasanawala SS, Lustig M. ESPIRiT-an eigenvalue approach to autocalibrating parallel MRI: Where SENSE meets GRAPPA. Magnetic Resonance in Medicine 2013; 71:990–1001. 10.1002/mrm.24751.
13. Boehm C, Diefenbach MN, Makowski MR, Karampinos DC. Improved Body Quantitative Susceptibility Mapping By Using a Variable-layer Single-min-cut Graph-cut for Field-mapping. Magn Reson Med 2020; 85:1697–1712. 10.1002/mrm.28515.
14. Armstrong, T., Dregely, I., Stemmer, A., Han, F., Natsuaki, Y., Sung, K. and Wu, H.H. (2018), Free-breathing liver fat quantification using a multiecho 3D stack-of-radial technique. Magn. Reson. Med, 79: 370-382. https://doi.org/10.1002/mrm.26693
15. Zhong X, Hu HH, Armstrong T, Li X, Lee YH, Tsao TC, Nickel MD, Kannengiesser SAR, Dale BM, Deshpande V, Kiefer B, Wu HH. Free-Breathing Volumetric Liver R2* and Proton Density Fat Fraction Quantification in Pediatric Patients Using Stack-of-Radial MRI With Self-Gating Motion Compensation. J Magn Reson Imaging. 2021 Jan;53(1):118-129. doi: 10.1002/jmri.27205. Epub 2020 Jun 1. PMID: 32478915.
Figures
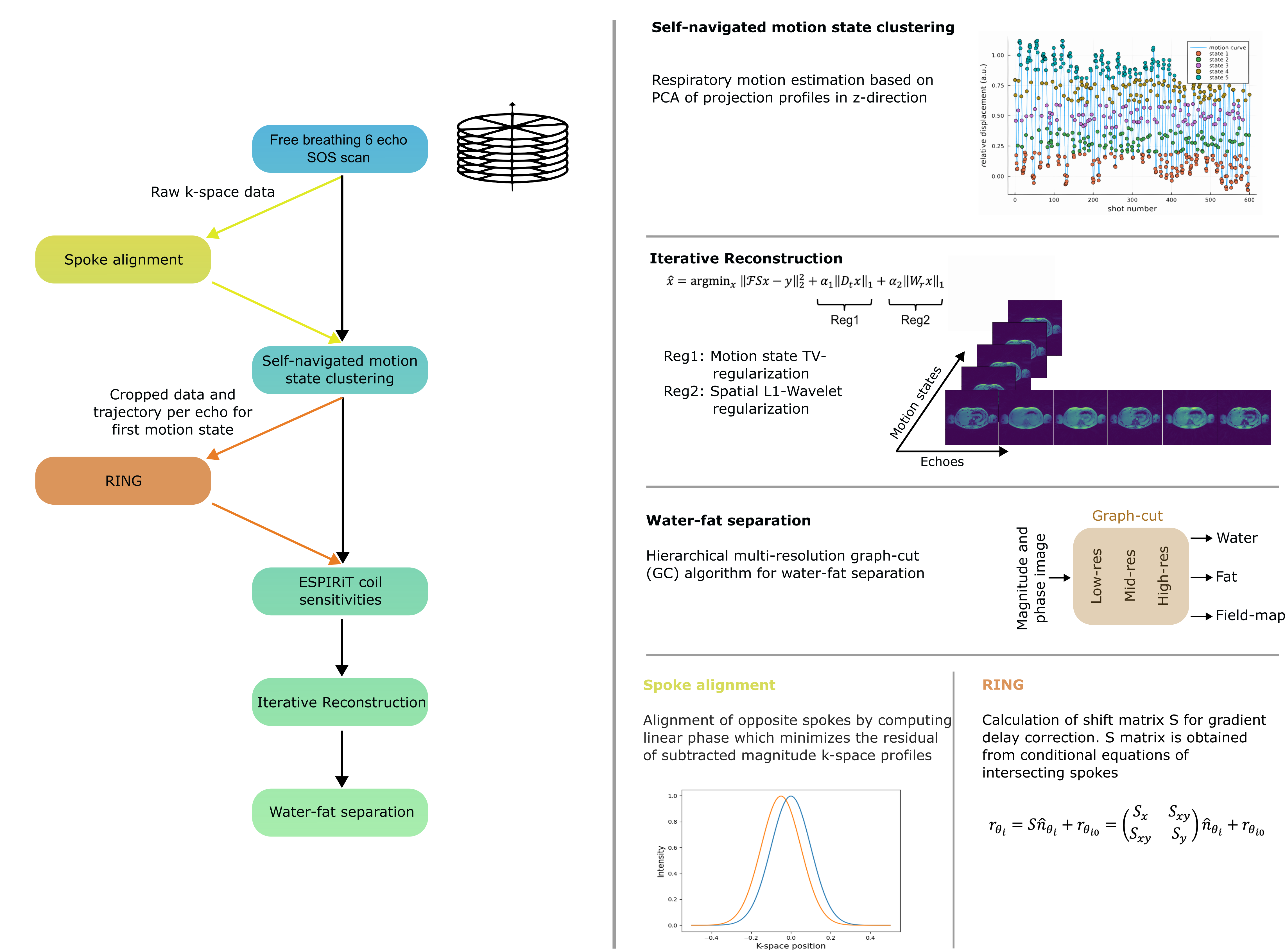
Figure 1. Data-driven correction pipeline for radial 6 echo stack-of-stars data using either RING or a spoke alignment method. Spoke alignment is performed on all k-space data due to its dependence on opposite spokes2. Five different motion states are used for self-navigation. RING correction9 is performed for the first motion state, per echo and exclusively for the central slice. Coil sensitivities are calculated via ESPIRiT12 before the iterative reconstruction. Water-fat separation is performed using the Graph-cut13 and employing a multi-peak fat model with a single T2* decay.
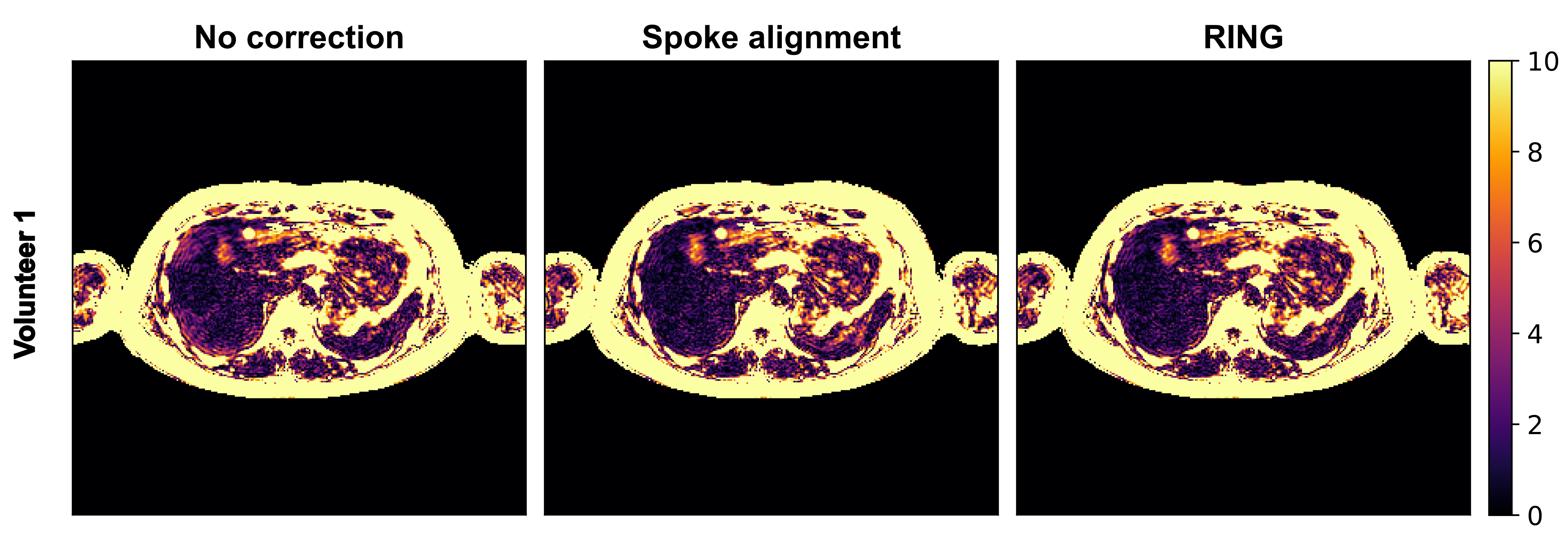
Figure 2. PDFF images of a respiratory-gated acquisition of volunteer 1 using left: no correction, middle: spoke alignment, and right: RING. The gating window was set to 7mm and in FH direction. Results show more homogeneous PDFF maps for both correction techniques. There is no observable difference between the image quality of the spoke alignment and RING.
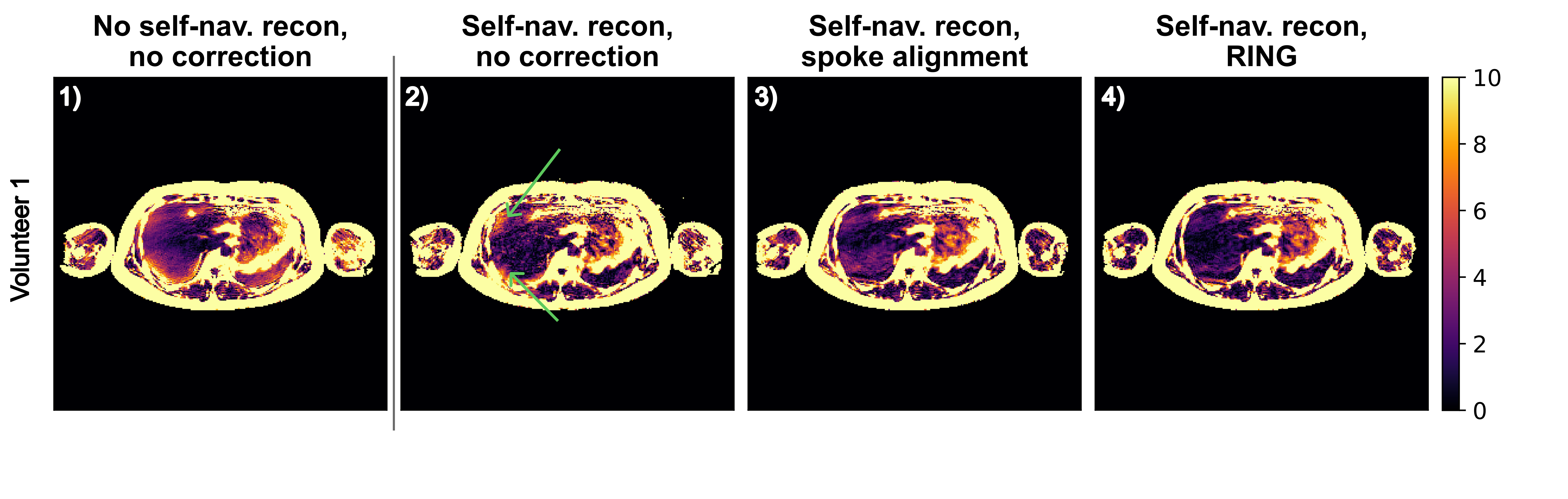
Figure 3. PDFF maps of a free-breathing SoS acquisition of volunteer 1. 1) reference without self-navigated reconstruction and gradient delay correction; 2) only self-navigated reconstruction; 3), 4) self-navigated reconstruction with spoke alignment or RING method, respectively. Maps are more homogeneous when a self-navigation-based reconstruction is used and even more following a gradient delay correction. Arrows in 2) show artifacts on the edge of the right liver lobe, which are corrected for after gradient delay correction. RING produces the most homogeneous results.
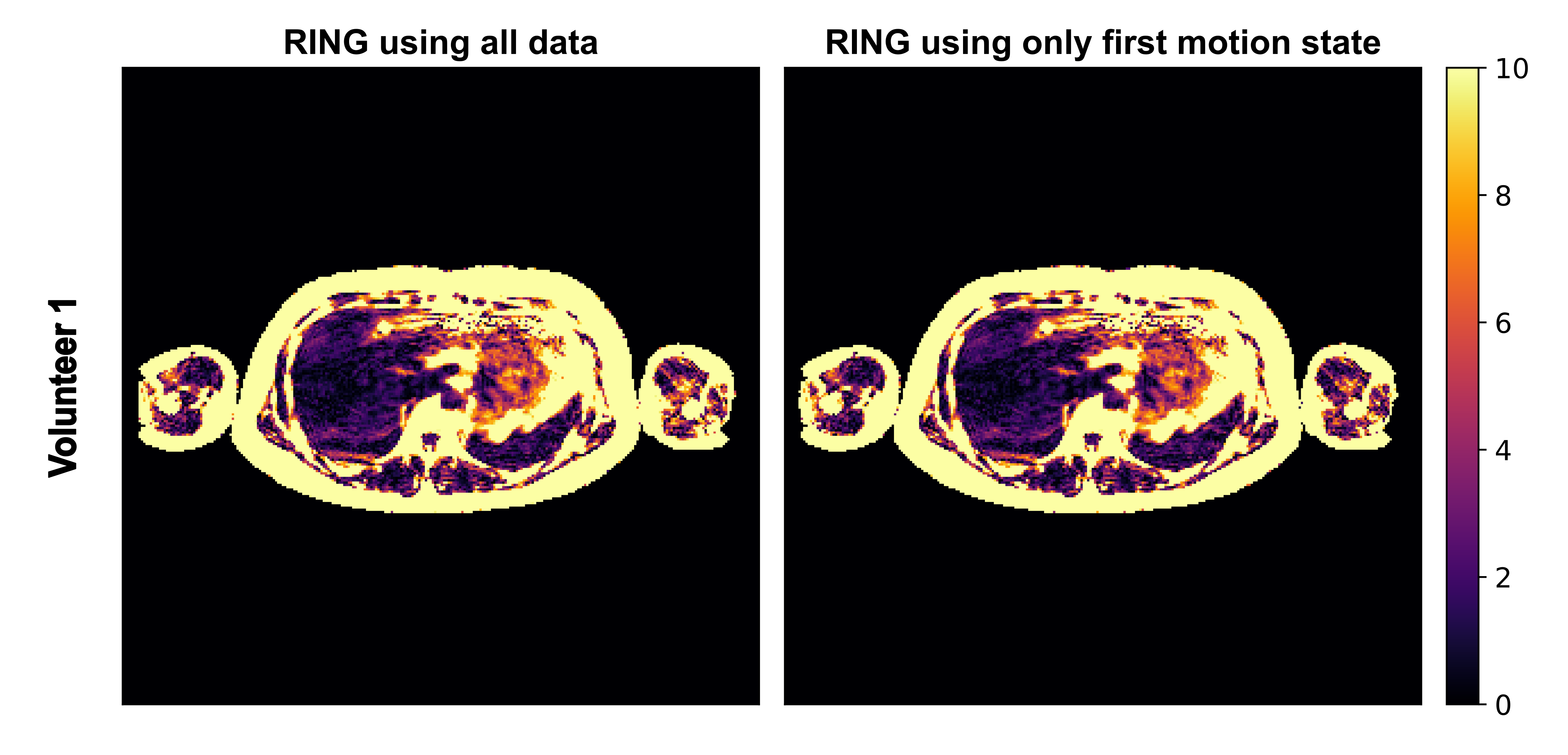
Figure 4. PDFF maps of volunteer 1 when the RING method was performed using all data from all motion states versus using only the data from the first motion state. No significant differences in PDFF map homogeneity are observed.
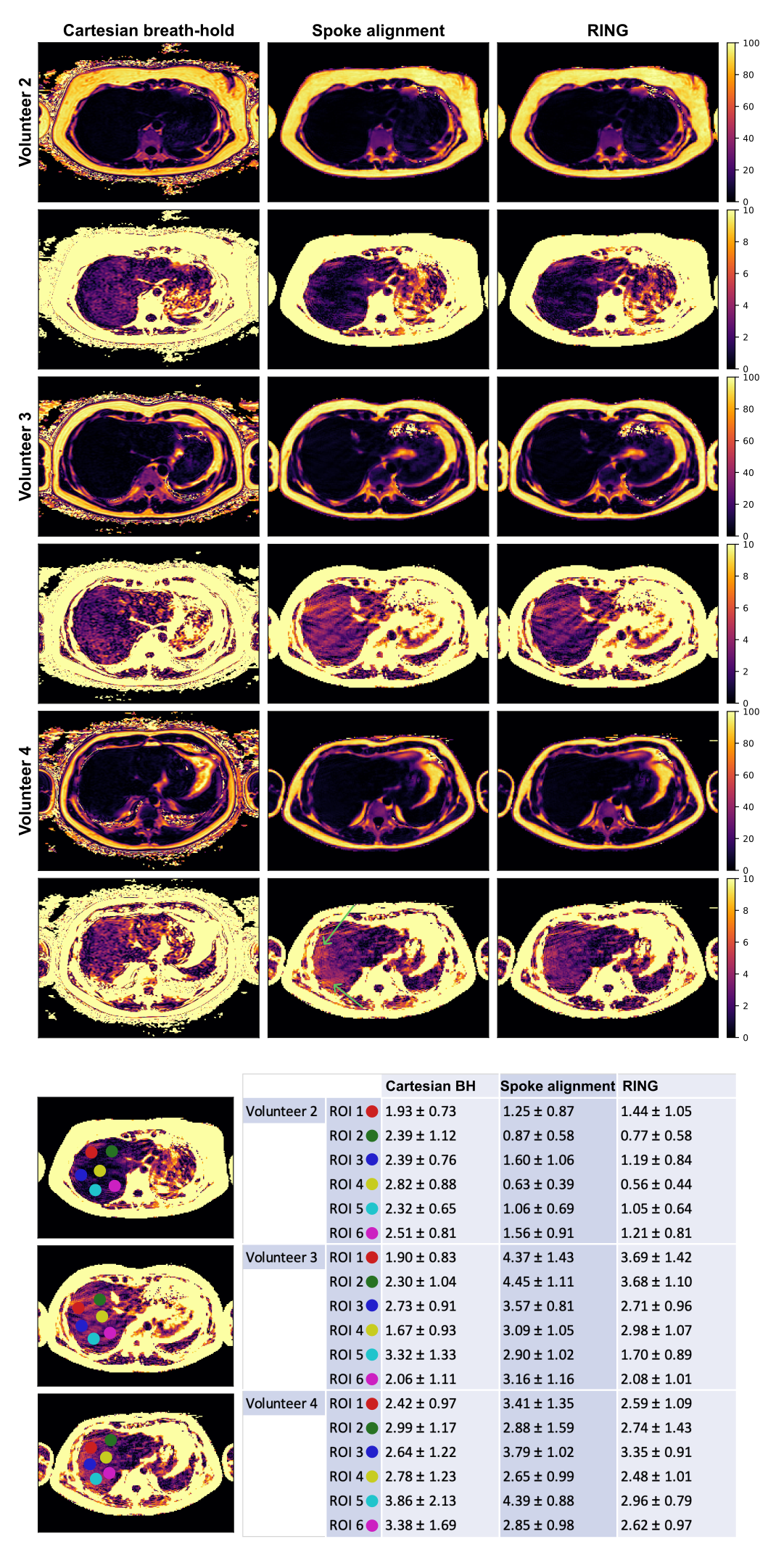
Figure 5. PDFF maps of three volunteers comparing a clinical Cartesian breath-hold sequence to a radial SoS acquisition. The RING method yields more homogeneous PDFF maps compared to the spoke alignment. The arrows for the spoke aligned results of volunteer 4 show artifacts at the edge of the liver lobe.
Mean values and standard deviation of PDFF across all six ROIs for Cartesian BH, Spoke alignment, RING respectively:
Volunteer 2: 2.39 ± 0.26, 1.16 ± 0.35, 1.04 ± 0.29;
Volunteer 3: 2.33 ± 0.55, 3.59 ± 0.61, 2.81 ± 0.75;
Volunteer 4: 3.01 ± 0.48, 3.33 ± 0.61, 2.79 ± 0.29