2642
Leveraging Compressed Sensing for Improvement of FIDDLE Image Quality Rather Than for Acquisition Speed1Siemens Medical Solutions USA, Inc., Durham, NC, United States, 2Duke Cardiovascular MR Center, Duke University, Durham, NC, United States, 3Siemens Medical Solutions USA, Inc., Issaquah, WA, United States
Synopsis
Keywords: Artifacts, Cardiovascular, FIDDLE
Motivation: Imperfect breath holding and cardiac arrhythmia create chest wall and cardiac ghosting in conventional segmented dark-blood LGE images (FIDDLE) often rendering them non-clinical.
Goal(s): We aimed to apply compressed sensing ‘CS’ as the solution to this problem, to acquire FIDDLE images without ghosting, even in challenging patients.
Approach: CS can acquire multiple high-spatial and excellent-temporal resolution single shots that intrinsically never display ghosting artifacts. Sparsity is created along the shot dimension, enabling CS to reconstruct the generally not-so-sparse FIDDLE images. Single shot averaging further improves SNR.
Results: The CS FIDDLE images show high SNR and no ghosting. They should simplify clinical imaging.
Impact: The CS FIDDLE method should improve clinical CMR image quality and alleviate the need for repeated acquisitions due to poor breath holding. It also enables using CS for the acquisition of single still-frame images with intrinsically higher SNR.
Background
Compressed Sensing (CS) is commonly used to significantly accelerate acquisition while accepting variable reductions in image quality (IQ). Here we explored the opposite approach for breath-held Flow Independent Dark Blood Delayed Enhancement (FIDDLE), a black-blood LGE technique1. We applied CS for IQ improvement of FIDDLE while keeping acquisition time, spatial and temporal resolution identical to the conventional (CONV) segmented technique2. Specifically, we aimed to eliminate the frequent ghosting (GHO) produced by segmented interleaved reordering during imperfect breath holds or arrhythmia.FIDDLE combines a magnetization transfer and inversion recovery (MT-IR) preparation to separate tissue from blood so that the magnetization of blood, myocardium, and infarct are ordered from smallest to largest. In the phase sensitive IR (PSIR) reconstructed FIDDLE image, the magnetization levels are mapped to a grey scale. Blood as the smallest species is depicted black.
Methods
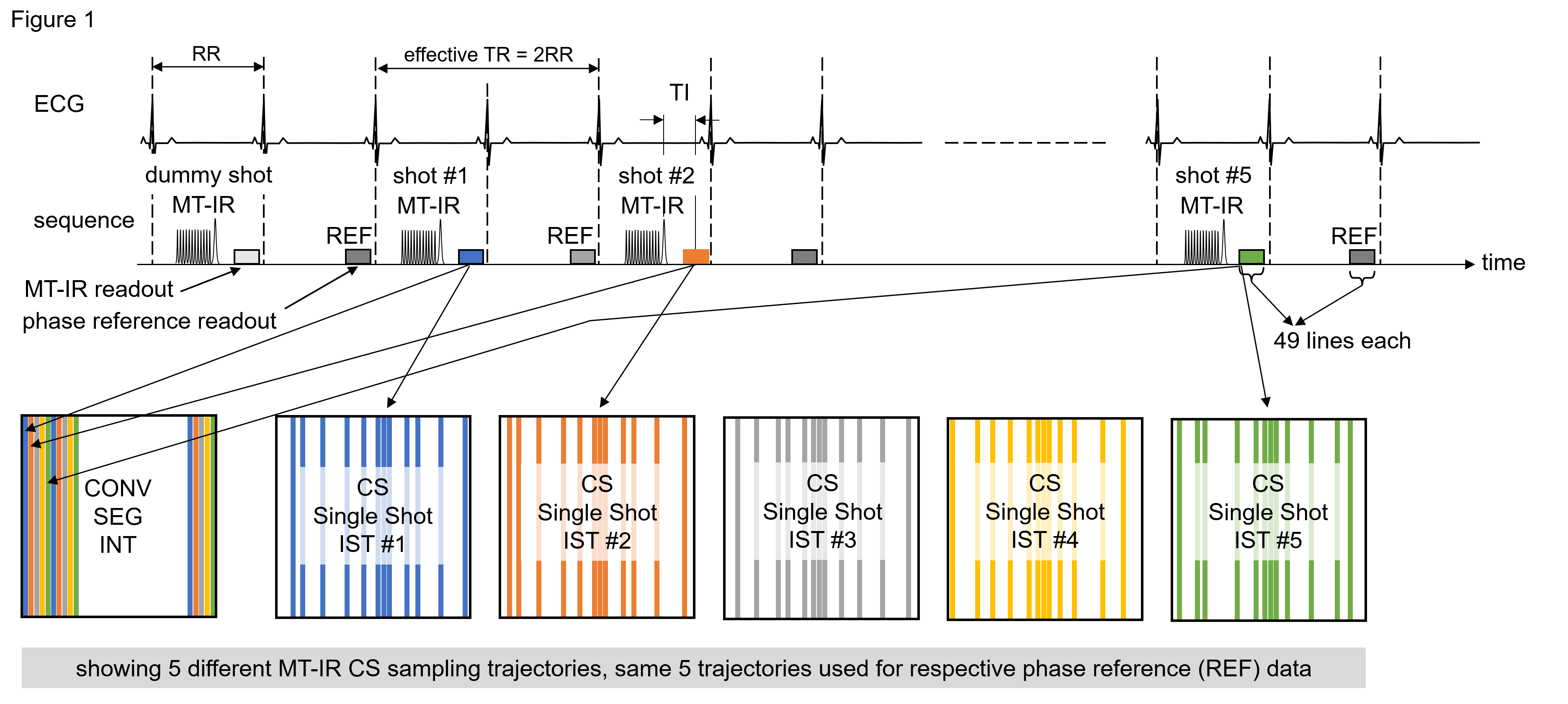
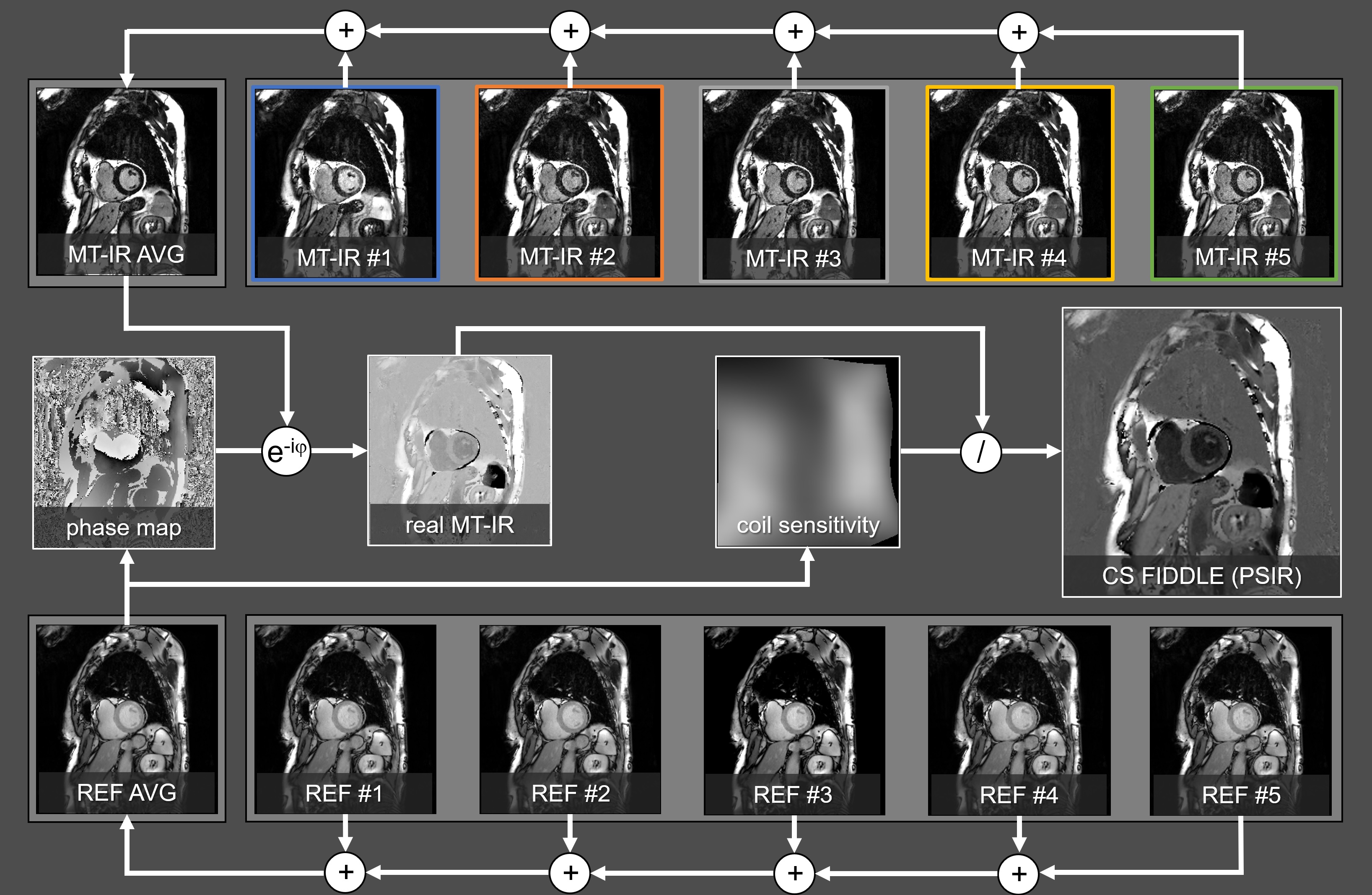
In 30 CMR patients we acquired 35 CONV immediately followed by 35 prototype CS FIDDLE data sets on a 3T clinical MR scanner (MAGNETOM Vida, *Siemens Healthineers AG, Erlangen, Germany). Each breath-held acquisition consisted of 5 MT-IR shots of 49 lines alternating with 5 PSIR reference (REF) shots (256 x 245 matrix, 10 heartbeats). CONV employed interleaved segmented reordering. Each CS MT-IR shot had a different variable density incoherent sampling trajectory (IST). Each REF used the same IST as its preceding MT-IR shot (Figure 1). Each CS MT-IR data set was reconstructed into a separate single shot image jointly with the other MT-IR shots, to exploit sparsity in the shot dimension. The CS MT-IR images were averaged (MT-IR AVG) to remove IST dependent artifacts and improve SNR (Figure 2). An averaged reference (REF AVG) image was created from CS REF data in the same manner. We implemented the PSIR reconstruction as MATLAB program (MathWorks, Natick, MA) and compiled it into a chroot container, executed within the FIRE3 works-in-progress package* on the scanner for immediate image display. A coil sensitivity and a phase map were calculated from the REF AVG image to create a real-valued, coil-normalized FIDDLE image (Figure 2). We compared CONV and CS FIDDLE images for GHO (present/absent) by McNemar’s test. A Wilcoxon signed-rank test assessed IQ (Likert scale 3-0, excellent, good, moderate, nondiagnostic), subjective SNR (3-1, excellent, good, moderate), and comparative rank (RANK, better, equivalent, worse). SNR was measured in blood and myocardium of the MT-IR AVG images and compared between CONV and CS by a two-tailed t-test.Results
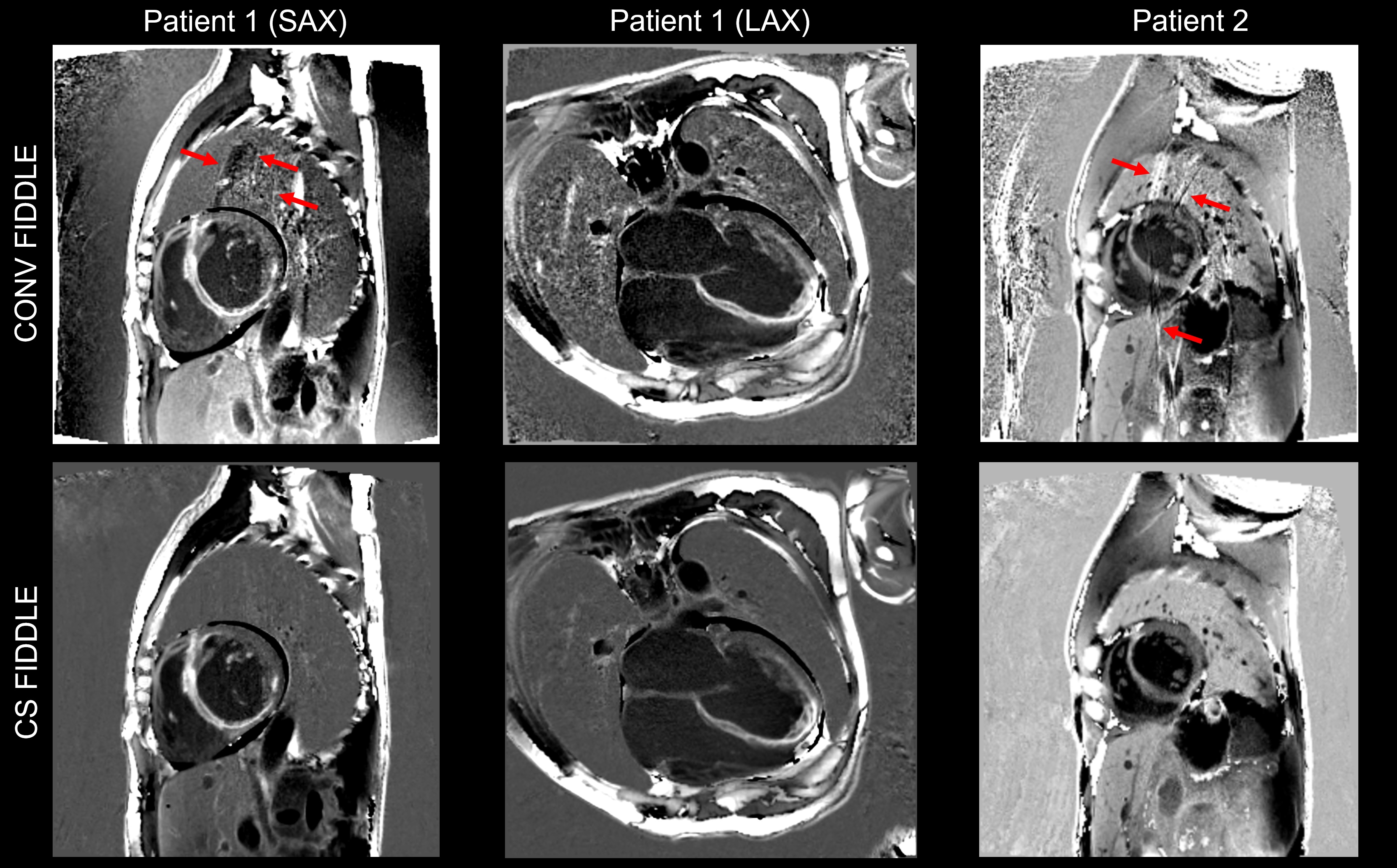
27 short-axis (SAX) and 8 long-axis (LAX) images were acquired (13 infarcts total). There were significantly fewer ghosting artifacts in CS FIDDLE vs CONV (0 vs 7, p< 0.05). IQ was higher for CS FIDDLE compared to CONV (1.9±0.1 vs 1.4±0.1, p< 0.05). RANK was significantly higher for CS FIDDLE (better 66%, equivalent 34%, p< 0.05). Measured SNR was significantly higher for the CS MT-IR AVG images in blood (CS 59.2±6.0 vs CONV 40.5±4.1, p < 0.0001) and myocardium (CS 25.5±2.9 vs CONV 19.3±2.4, p < 0.001), but not in infarct (CS 82.4±23.2 vs CONV 58.9±10.5). Subjective SNR was higher for CS FIDDLE compared to CONV (2.0±0.1 vs 1.3±0.1, p< 0.0001).Figure 3 shows typical CONV and CS FIDDLE images. In the SAX views of patients 1 and 2, ghosting is present in CONV (arrows), but absent in the CS FIDDLE images. Patient 1 has extensive enhancement in the septum, inferior wall, and apex. In patient 2, late enhancement in the anteroseptum and anterior wall is visualized with CS FIDDLE, but it is obscured by ghosting in CONV FIDDLE. The CS FIDDLE images appear cleaner, likely due to the increased SNR. In CS FIDDLE, the absence of salt-and-pepper noise in the lungs and air is probably owed to the new coil sensitivity calculation as part of our PSIR reconstruction.
Conclusion
CS FIDDLE images had significantly better IQ than CONV segmented images. Motion-induced ghosting was substantially absent since it originates from k-space segmentation, while CS FIDDLE uses single-shots. SNR was higher with CS FIDDLE, likely due to the denoising feature of CS and the denser sampling of k-space center. Interestingly, we utilized the acceleration afforded by CS to acquire multiple single shots, thereby creating sparsity along the shot dimension, which in turn allowed applying the CS technique to the generally not-so-sparse FIDDLE images.A potential next step is to perform a motion correction (MOCO4) of the CS images prior to averaging, to account for residual motion during breath holding. A free breathing version with higher IQ, better spatial and temporal resolution, and higher SNR than possible with conventional averaged MOCO techniques4 will also be investigated.
Acknowledgements
References
1. Kim H, Rehwald, W, Kim R, et al. Dark-Blood Delayed Enhancement Cardiac Magnetic Resonance of Myocardial Infarction, J Am Coll Cardiol Img 2018;11:1758–69
2. Simonetti O, Kim R, et al. An Improved MR Imaging Technique for the Visualization of Myocardial Infarction. Radiology 2001; 218:215–223.
3. Chow K, Kellman P, Xue H. Prototyping Image Reconstruction and Analysis with FIRE. Proc. SCMR. Virtual Scientific Sessions; 2021. p. 838972.
4. Xue H, Shah S, Greiser A, et al. Motion Correction for Myocardial T1 Mapping Using Image Registration with Synthetic Image Estimation. Magn ResonMed 67:1644–1655, 2012.
Figures