2635
Alterations in Brain Glymphatic Function and White Matter Microstructural Properties in patients with IBD1Department of Magnetic Resonance, Lanzhou University Second Hospital, LanZhou, China, 2Philips Healthcare, Xi’an, China
Synopsis
Keywords: White Matter, Inflammation, Inflammatory Bowel Disease
Motivation: The mechanisms underlying brain structural changes and its relationship with neuropsychological symptoms in inflammatory bowel disease (IBD) remain unclear.
Goal(s): To explore the relationship between the function of the glymphatic system, changes in white matter microstructure, and clinical symptoms in patients with IBD.
Approach: Diffusion along perivascular spaces (DTI-ALPS) and tract-based spatial statistics (TBSS) techniques were used.
Results: The observed alterations in white matter microstructure and decreased clearance rate of the glymphatic system in IBD may be an external manifestation of neuroinflammation. These abnormalities are related to sleep disorders and pain in IBD patients.
Impact: Neuroinflammation is known to have adverse effects on glymphatic flow. The changes in diffusion MRI indicators suggest glymphatic dysfunction in IBD. Chronic visceral pain reduces the diffusion rate. The changes in diffusion MRI indicators are associated with poor cognitive performance.
Introduction
Inflammatory bowel disease (IBD) is a kind of immune mediated gastrointestinal disease1 that may cause inflammatory reactions in peripheral tissues. The glymphatic system is a waste drainage system in the brain2. Glymphatic clearance dysfunction may lead to neuronal damage, followed by cognitive and emotional abnormalities3. Previous studies have provided evidence to suggest an association between drainage dysfunction and neuroinflammation4. However, the brain structural, glymphatic clearance changes and its relationship with neuropsychological symptoms in IBD remain less explored. This study aims to explore the neuropathological mechanisms of brain changes in IBD patients by examining alterations in brain glymphatic function and white matter microstructural properties in patients with IBD.Materials and Methods
This study was approved by the Ethics Committee of Lanzhou University Second Hospital. All MR examination were performed on a 3.0 T MR scanner (Ingenia CX, Philips Healthcare, Netherlands) equipped with 32 channel head coils. In this prospective study, 58 IBD patients and 30 age/sex-matched health controls (HC) were included. The diffusion spectrum imaging (DSI) data was obtained with a maximum b-value set at 4000. The parameters are as follows: [TR]=4200 ms, [TE]=89 ms, voxel size = 2×2×2 mm3, Matrix = 104x104. A total of 72 slices were acquired using a multiband acceleration factor of 3. The QSIPrep5 based on Nitype6 was used for preprocessing. DSI-studio (https://dsi-studio.labsolver.org/) was used to fit the DTI model parameters, such as fractional anisotropy (FA), mean diffusivity (MD), radial diffusivity (RD), axial diffusivity (AD), and obtain the diffusion metrics in the X, Y, and Z axes. Tract-Based Spatial Statistics (TBSS) was employed to assess group-level differences in voxel-based diffusion metric values based on the white matter skeleton of fiber bundles. The methods used to calculate the DTI-ALPS is referenced by previous research to represents the function of the glymphatic system4.Statistical analysis was performed using SPSS version 25.0 (IBM). The General Linear Model (GLM) was used to group comparison of the DTI-ALPS index while controlling for age, gender, education level, and total intracranial volume (TIV). Furthermore, Pearson correlation coefficients were used to investigate the relationships between DTI-ALPS index and white matter microstructural changes in IBD patients with clinical symptom scores and psychometric testing. A significance level of P<0.05 was set.
Results
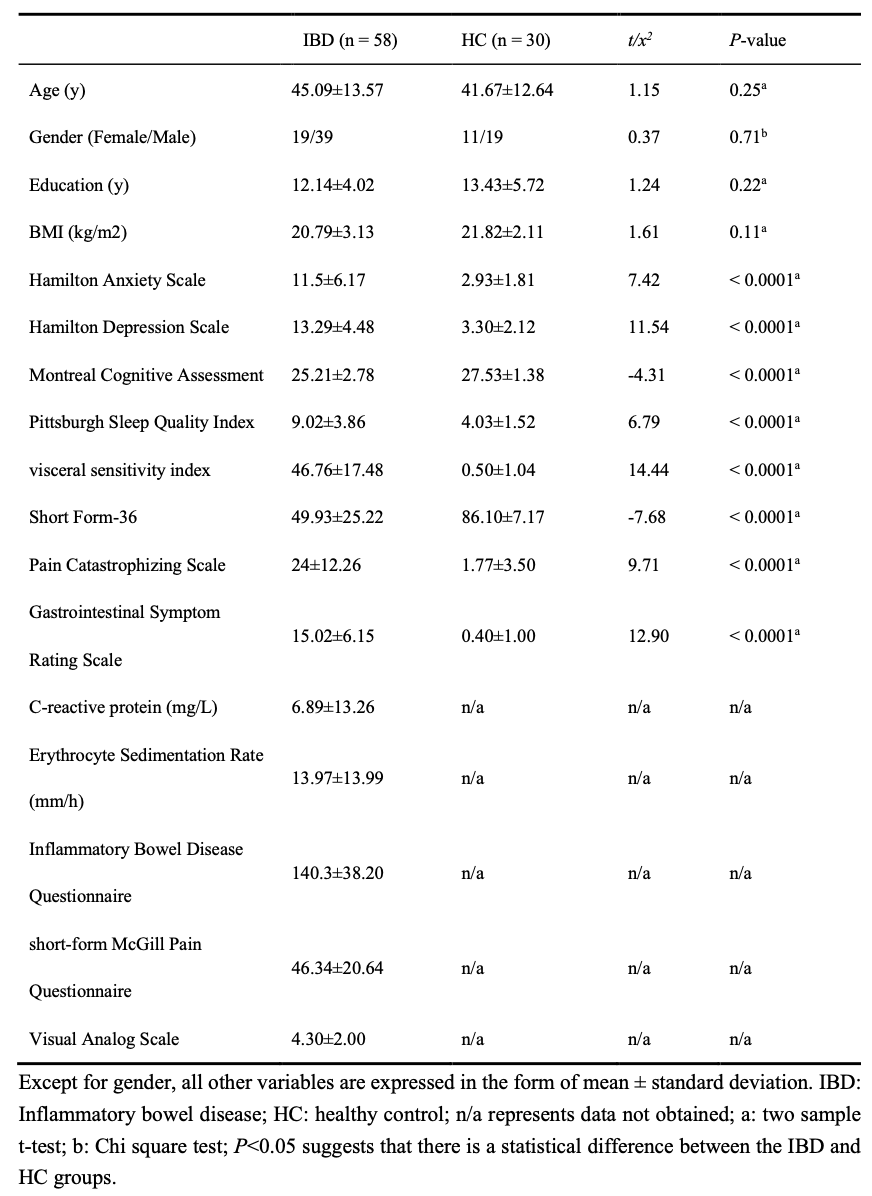
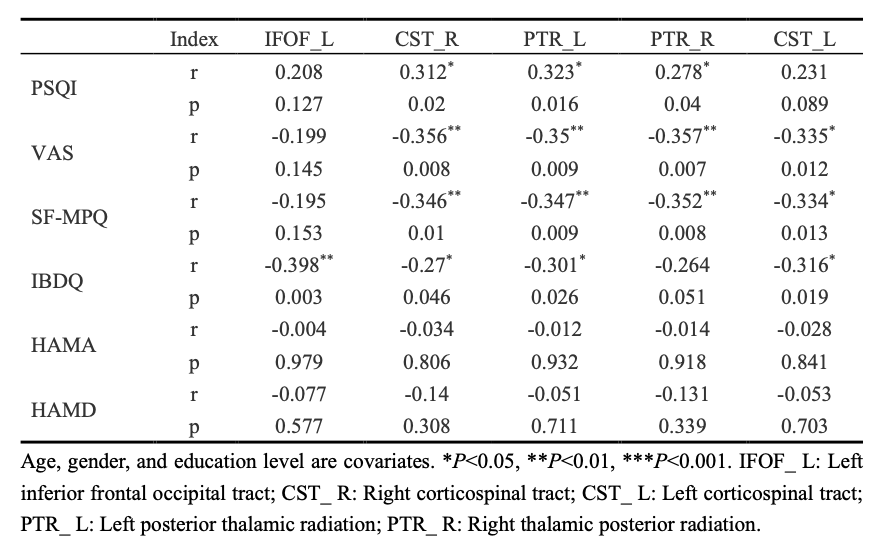
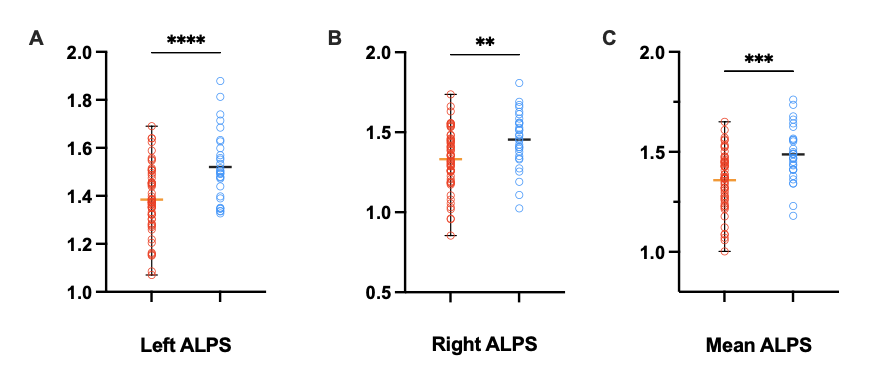
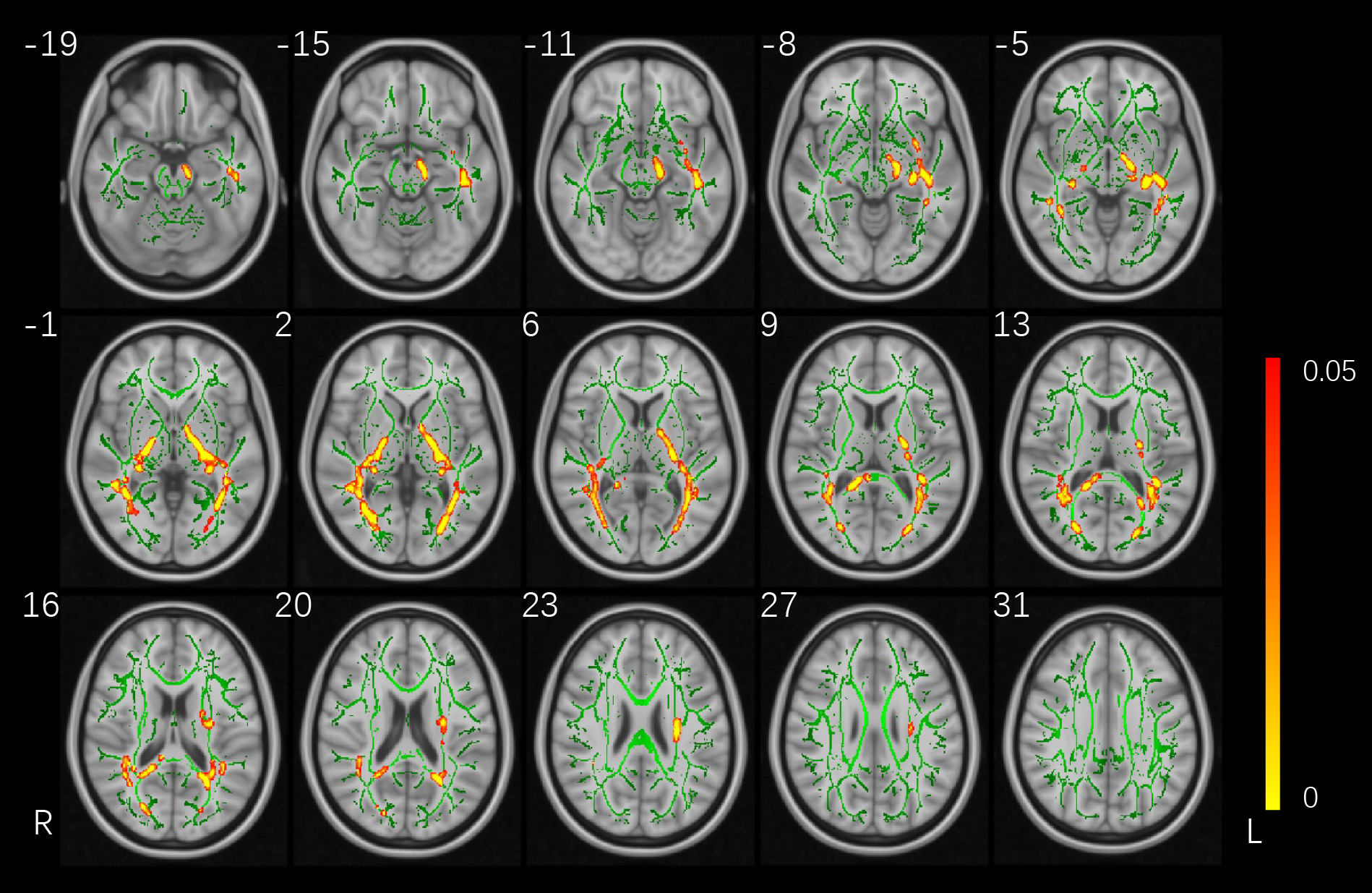
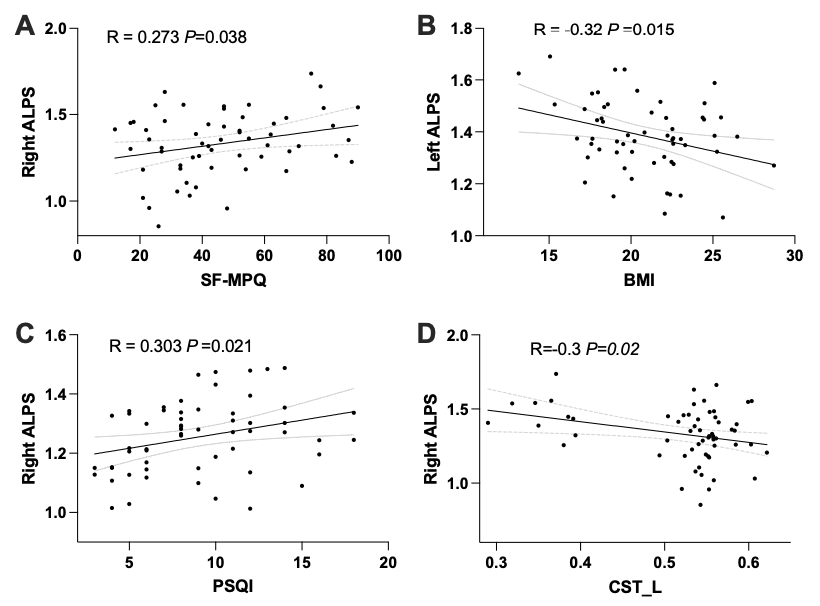
The results of clinical data are shown in Table 1. After adjusting for age, gender, years of education, and TIV, the DTI-ALPS index of the IBD patient group was significantly decreased, and the difference in DTI-ALPS index of the left hemisphere was more significant than that of the right hemisphere (shown as Figure 1). Using a threshold of 0.2 for the average FA of the white matter skeleton, Figure 2 displayed the results of the FA analysis based on TBSS. Compared to the HC group, the IBD group exhibited significant reductions in FA values in the left inferior fronto-occipital fasciculus (IFOF), bilateral corticospinal tract (CST), and bilateral posterior thalamic radiation (PTR) (P<0.05, TFCE corrected). Parameters such as MD, AD, and RD did not show significant differences in the group comparisons (P>0.05, TFCE corrected).The average FA value of the left IFOF was significantly negatively correlated with the IBDQ score (R=-0.398, P=0.003). The average FA values of the right CST and bilateral PTR showed significant positive correlations with the PSQI score (P<0.05). VAS and SF-MPQ scores exhibited negative correlations with the FA values of all different fiber bundles except for the left IFOF (P<0.05). IBDQ scores displayed negative correlations with the FA values of all different fiber bundles except for the right PTR (P<0.05). Please referred to Table2 and Figure 3 for details.
Discussion
Peripheral inflammation is known to cause neuronal damage and increase the risk of neurodegenerative diseases7. This may mean that the observed changes in white matter microstructure and decreased clearance rate of the glymphatic system in IBD are both caused by neuroinflammation. Chronic visceral pain has been proven to be related to microstructural damage in the brain8. The results indicate that IBD patients also exhibit changes in brain microstructure and are significantly correlated with clinical factors such as pain and sleep disorders.Conclusion
The reduced function of the brain glymphatic system in clearing waste in IBD patients is related to abnormal white matter microstructure integrity and the impact of neuroinflammation. Improving the sleep quality of patients may help reduce the impact of neuroinflammation on the brain, which would be a potential alternative treatment option.Acknowledgements
I would like to thank every participants in this research for their help.References
1. MacDonald S, Heisler C, Mathias H, et al. Stakeholder Perspectives on Access to IBD Care: Proceedings From a National IBD Access Summit. J Can Assoc Gastroenterol 2022;5:153-160.
2. Taoka T, Masutani Y, Kawai H, et al. Evaluation of glymphatic system activity with the diffusion MR technique: diffusion tensor image analysis along the perivascular space (DTI-ALPS) in Alzheimer’s disease cases. Japanese journal of radiology 2017;35:172-178.
3. Andica C, Kamagata K, Takabayashi K, et al. Neuroimaging findings related to glymphatic system alterations in older adults with metabolic syndrome. Neurobiology of Disease 2023;177:105990.
4. Taoka T, Masutani Y, Kawai H, et al. Evaluation of glymphatic system activity with the diffusion MR technique: diffusion tensor image analysis along the perivascular space (DTI-ALPS) in Alzheimer's disease cases. Jpn J Radiol 2017;35:172-178.
5. Gorgolewski K, Burns CD, Madison C, et al. Nipype: a flexible, lightweight and extensible neuroimaging data processing framework in python. Front Neuroinform 2011;5:13.
6. Cieslak M, Cook PA, He X, et al. QSIPrep: an integrative platform for preprocessing and reconstructing diffusion MRI data. Nat Methods 2021;18:775-778.
7. Zhang W, Xiao D, Mao Q, Xia H. Role of neuroinflammation in neurodegeneration development. Signal Transduction and Targeted Therapy 2023;8:267.
8. Frøkjær JB, Olesen SS, Gram M, et al. Altered brain microstructure assessed by diffusion tensor imaging in patients with chronic pancreatitis. Gut 2011;60:1554-1562.
Figures