2631
Association between Glymphatic Function and Peripheral Inflammation in Different Motor Subtypes of Parkinson Disease1Department of Radiology, Fujian Medical University Union Hospital, Fujian, China, 2Department of Neurology, Fujian Medical University Union Hospital, Fujian, China, 3MR Research Collaboration Team, Siemens Healthineers Ltd, Shanghai, China
Synopsis
Keywords: Parkinson's Disease, Parkinson's Disease, Glymphatic Function, Peripheral Inflammation, DTI-ALPS
Motivation: The association between glymphatic system and peripheral inflammation has not been well studied.
Goal(s): Our study aimed to explore the relationship between glymphatic system and peripheral inflammation in PD patients and PD subtypes, and their link to motor symptoms.
Approach: We used DTI to calculate the DTI-ALPS index, a non-invasive measure of glymphatic function, and evaluated the association between the DTI-ALPS index and clinical parameters using multiple linear regression.
Results: Our study revealed a correlation between peripheral inflammation and glymphatic dysfunction in PD, particularly in TD subtype. Furthermore, the association between peripheral inflammation and clinical severity was observed in PD and PIGD patients.
Impact: This study provides new insights into the pathophysiology of PD and potential therapeutic options.
Introduction
Recent evidence suggests a crucial role of both central and peripheral inflammation in the pathogenesis and progression of Parkinson's disease (PD)1,2. Moreover, mounting evidence supports the role of peripheral inflammation, encompassing both cytokines and immune cells, in PD's pathophysiology3,4. However, the mechanisms connecting central and peripheral inflammation remain unclear. The glymphatic system, a cerebral ‘waste clearance’ system, plays an important role in cerebral immunological surveillance and peripheral immune responses5. The non-invasive diffusion tensor image analysis along the perivascular space (DTI-ALPS) index has recently been shown to provide a good representation and reproducibility for glymphatic clearance function in vivo6. Therefore, the aim of our study was to investigate the link between DTI-ALPS index and peripheral inflammation in PD patients, Tremor Dominant (TD) subtype and postural instability and gait difficulty (PIGD) subtype, as well as their connection with PD's motor symptoms.Methods
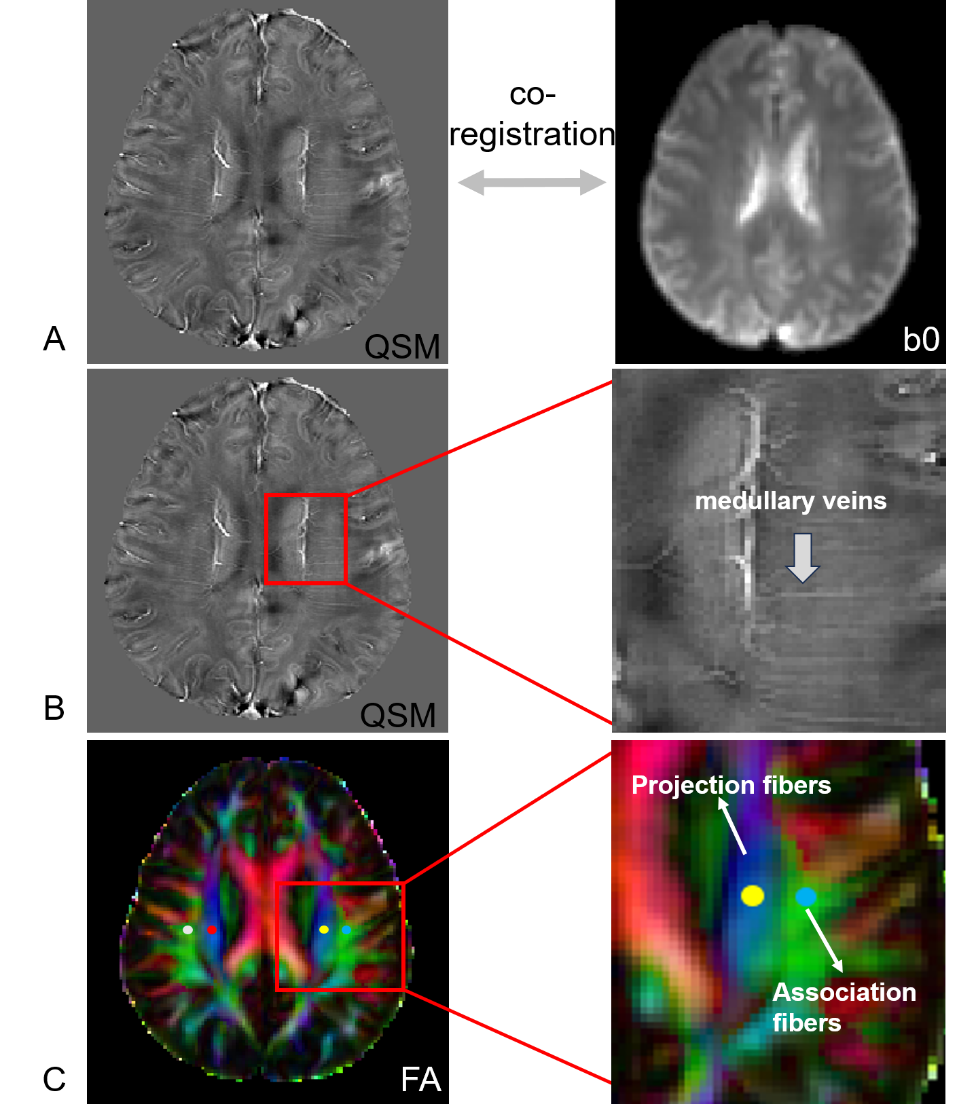
This study enrolled 96 PD patients, including 31 with TD and 50 with PIGD. Magnetic resonance imaging (MRI) including quantitative susceptibility mapping (QSM) and diffusion tensor imaging (DTI) were performed on a 3T system (MAGNETOM Prisma, Siemens Healthcare, Erlangen, Germany). DTI was acquired using a spinning-echo echo-planar imaging (SE-EPI) sequence with 9 b-values (250, 350, 400, 550, 750, 950, 1100, 1150, 1500 s/mm2) and 3, 2, 4, 4, 3, 12, 8, 4 and 6 directions, respectively. The parameters were TR = 3900 ms; ER = 88ms; FOV = 230 × 230mm2. QSM imaging was based on 3D flow-compensated multi-echo gradient-echo (GRE) images in the axial plane (TR = 35 ms; first TE = 6.67 ms; uniform echo spacing = 6.24 ms; last TE = 25.39 ms; number of echoes = 4; FA = 15◦; FOV = 280 × 320 mm2; voxel size = 0.72 × 0.72 × 2 mm3). Diffusion tensor including a color-coded fractional anisotropy (FA) map and diffusivity map were created to calculate diffusivity in the direction of the x-axis, y-axis, and z-axis on each image. STISuite (https://people.eecs.berkeley.edu/~chunlei.liu/software.html) was used to calculate the QSM map. QSM images were co-registered to the b0 images by rigid-body-registering the first echo magnitude image from the GRE pulse sequence to b0 images using SPM12 (www.fil.ion.ucl.ac.uk/spm/software/spm12). The slice where the direction of the deep medullary veins was vertical to the ventricle body was identified and labeled by the QSM map. Four 3-mm-diameter regions of interest (ROIs) were placed in the bilateral projection fiber and the association fiber on the labeled slice using ITK-snap software. The ALPS index in each hemisphere was calculated as follows: ALPS index=mean(Dxproj,Dxassoc)/mean(Dyproj,Dzassoc) . Peripheral inflammation profiles including leukocyte, monocyte, neutrophil and lymphocyte counts, neutrophil-to-lymphocyte ratio (NLR) and platelet-to-lymphocyte ratio (PLR). Spearman’s correlation and multivariate linear regression analyses were conducted to describe the association between peripheral immune, ALPS index and MDS-UPDRS III in PD and motor subtypes patients.Results
In PD patients, mean ALPS index showed a significant Spearman correlation with lymphocyte counts, NLR, and PLR (all P<0.05). However, this association became insignificant after adjusting for age, sex, and duration. In the TD subtype, a significant Spearman correlation was found between ALPS index and lymphocyte, leukocyte counts, and NLR (all P<0.05). In multiple linear regression, the lymphocyte and leukocyte counts remained significantly correlated with ALPS index (β = 0.606, P=0.001 and β = 0.388, P=0.026). PLR only had a trend towards a negative relationship with mean ALPS index. In PIGD patients, mean ALPS index was found to have a negative Spearman correlation with monocyte counts, however, this association disappeared in multiple linear regression. MDS-UPDRS III was significantly Spearman-associated with leukocyte, lymphocyte counts, and PLR in both PD and PIGD subtype patients (all P<0.05). After adjusting for age, sex, and duration, the association remained significant except for PLR in PD patients.Discussion
Our results suggest that glymphatic dysfunction is associated with peripheral inflammation in PD patients, especiallyparticularly in the TD subtype. The possible mechanisms may contribute to the cerebral drain effect of the glymphatic system. According to previousPrevious research, has indicated that diminished glymphatic function results in reduced alpha-synuclein clearance. The accumulated alpha-synuclein7. Alpha-synuclein that accumulates is drained to the cervical lymph node through the glymphatic system, ultimately contributing to peripheral inflammation in PD5. The various findings presented in TD and PIGD subtypes imply that the pathogenic mechanisms and progression are different in the various PD phenotypes.Conclusion
In conclusion, our study indicates that peripheral inflammation is linked to glymphatic dysfunction and clinical severity in PD patients, particularly in the TD subtype. These findings may offer novel insights into the pathophysiology and potential therapeutic targets of PD.Acknowledgements
NoneReferences
1.Hirsch E C, Standaert D G. Ten unsolved questions about neuroinflammation in Parkinson's disease[J]. Movement Disorders, 2021, 36(1): 16-24.
2.Tansey MG, Romero‐Ramos M. Immune system responses in Parkinson's disease: Early and dynamic. European Journal of Neuroscience 2018;49:364-383.
3.Tansey MG, Wallings RL, Houser MC, Herrick MK, Keating CE, Joers V. Inflammation and immune dysfunction in Parkinson disease. Nature Reviews Immunology 2022;22:657-673.
4.Muñoz‐Delgado L, Macías‐García D, Jesús S, et al. Peripheral Immune Profile and Neutrophil‐to‐Lymphocyte Ratio in Parkinson's Disease. Movement Disorders 2021;36:2426-2430.
5.Liu Z, Huang Y, Wang X, et al. The cervical lymph node contributes to peripheral inflammation related to Parkinson’s disease. Journal of Neuroinflammation 2023;20.
6.Zhang W, Zhou Y, Wang J, et al. Glymphatic clearance function in patients with cerebral small vessel disease. NeuroImage 2021;238.
7.Zou W, Pu T, Feng W, et al. Blocking meningeal lymphatic drainage aggravates Parkinson’s disease-like pathology in mice overexpressing mutated α-synuclein. Translational Neurodegeneration 2019;8.
Figures