2623
Magnetic Resonance Imaging Findings Suggest that Cortical Thickness Mediates Glymphatic Effects on Cognitive Function in Alzheimer’s Disease1Hainan General Hospital, Haikou, China, 2MR Research Collaboration, Siemens Healthineers, Beijing, China, Beijing, China
Synopsis
Keywords: Alzheimer's Disease, Alzheimer's Disease, Cognition
Motivation: Glymphatic function, which eliminates soluble proteins from the brain, is positively associated with cognitive function for patients with Alzheimer’s disease (AD).
Goal(s): To analyze whether the associations between glymphatic function and cognitive function were mediated by regional cortical thickness (CTh) for patients with AD.
Approach: Mediator analysis was conducted to explore the ALPS index as a predictor, regional CThs as mediators, and cognitive test scores as outcomes.
Results: Mediation analysis showed that regional CTh was a significant mediator between ALPS index and executive function.
Impact: CTh is a key mediator between impaired glymphatic function and cognitive decline. Our findings provide insights regarding associations between decreased glymphatic function and cognitive decline in patients with AD.
Introduction
The glymphatic system is a highly organized fluid clearance pathway,1, 2 in which the movement of cerebrospinal fluid along the perivascular space eliminates soluble proteins from the brain;3 this system plays an important role in pathobiology for Alzheimer’s disease (AD). Diffusion tensor image analysis along the perivascular space (DTI-ALPS) techniques have utilized diffusion MRI to estimate glymphatic system activity through the ALPS index.4, 5 Previous studies demonstrated that the ALPS index, representing glymphatic function, is positively correlated with cognitive function in patients with AD.3, 6 Despite progress in AD research, the relationship between decreased glymphatic function and cognitive decline in patients with AD has not been fully explored. We hypothesized that cortical atrophy mediates the effect of glymphatic function on cognitive decline in patients with AD. We explored associations of glymphatic function and cortical thickness (CTh) with cognitive dysfunction, then investigated whether CTh mediates the relationship between glymphatic function and cognitive function in patients with AD.Methods
We included 145 patients with AD and 35 cognitively normal (CN) individuals from the Alzheimer's Disease Neuroimaging Initiative (ADNI) cohort, and 96 patients with AD and 21 CN individuals from our center. Participants underwent three-dimensional T1-weighted magnetic resonance imaging, diffusion tensor imaging (DTI), and neuropsychological evaluation. Whole-brain glymphatic function was measured by DTI along the perivascular space (ALPS). CTh maps were estimated and each hemisphere was divided into 33 cortical regions according to the Desikan–Killiany atlas. CTh values were compared among diagnostic groups using one-way analysis of covariance (ANCOVA). For patients with AD, we investigated associations between ALPS and CTh with cognitive dysfunction. Additionally, we conducted mediator analysis to explore the ALPS index as a predictor, regional CThs as mediators, and cognitive test scores as outcomes.Results
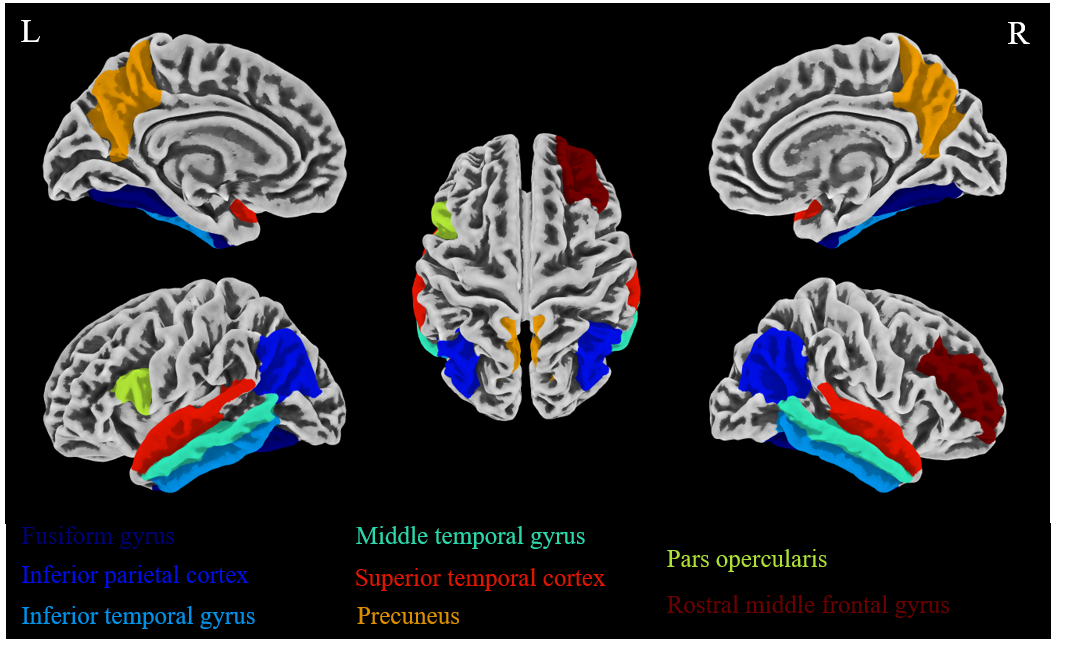
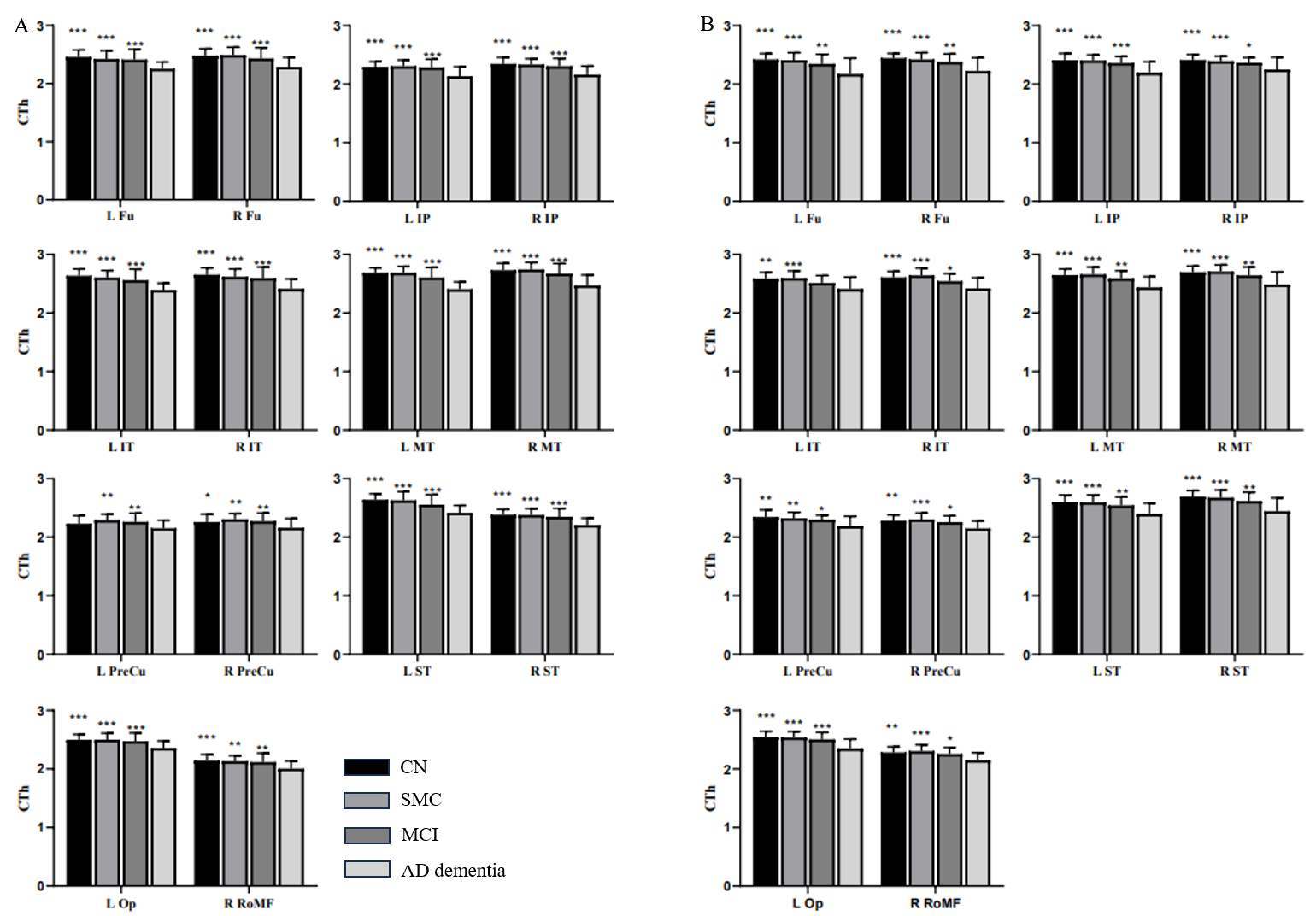
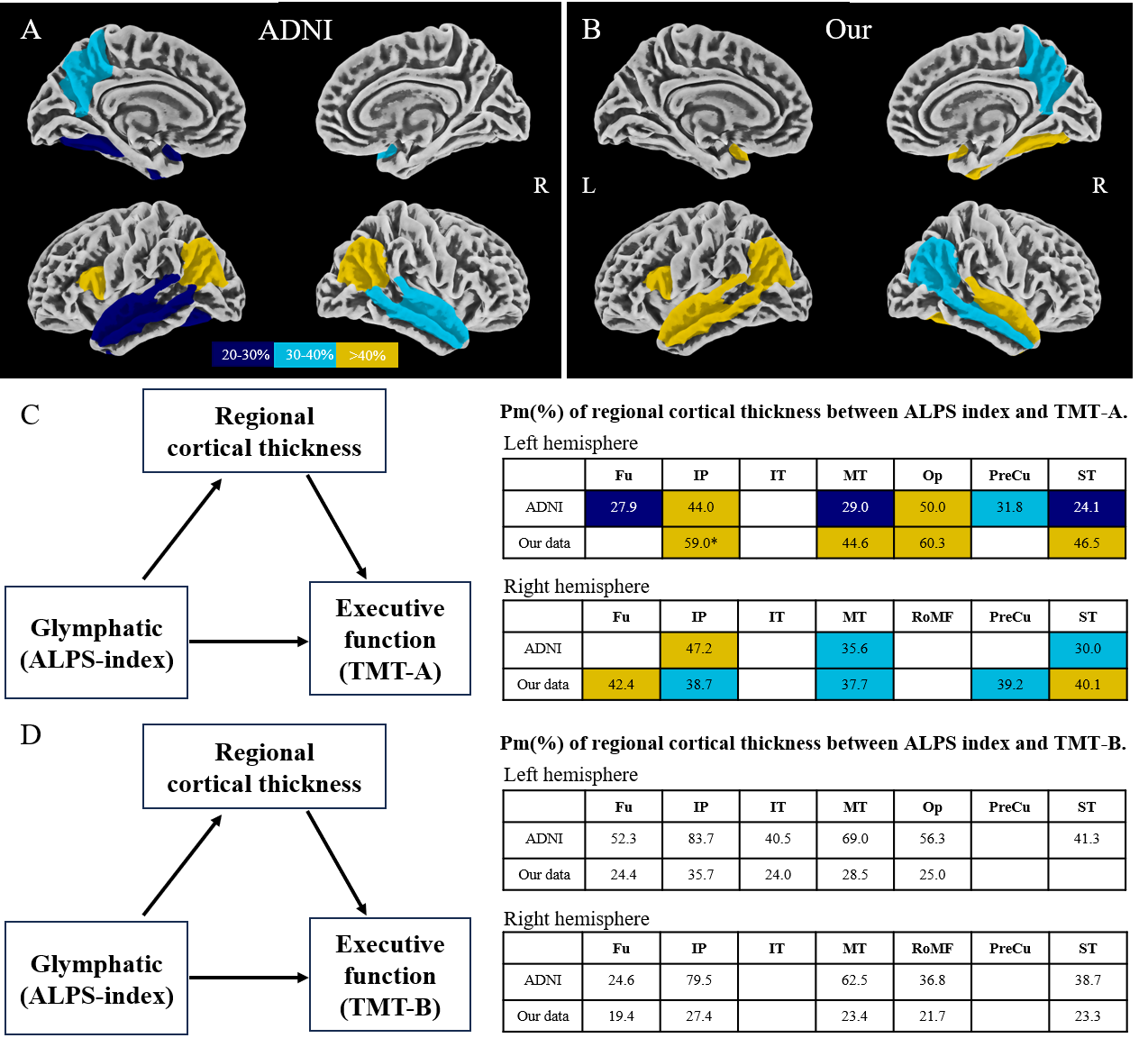
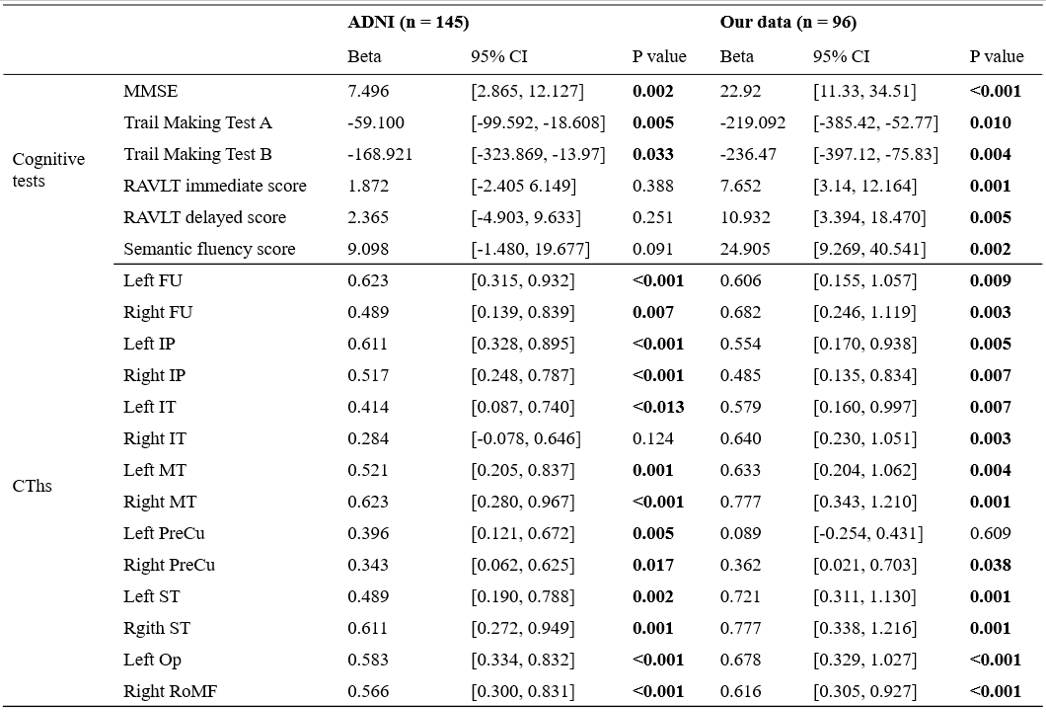
In both cohorts, we found consistent differences in CTh among the CN, SMC, MCI, and AD dementia groups at the bilateral fusiform gyrus, bilateral inferior parietal cortex, bilateral inferior temporal gyrus, bilateral middle temporal gyrus, bilateral superior temporal cortex, bilateral precuneus, left pars opercularis, and right rostral middle frontal gyrus (Figure 1). In both cohorts, the ALPS index was significantly positively correlated with MMSE score; it was negatively correlated with the TMT-A and TMT-B scores (Table 1). The ALPS index was not significantly associated with RAVLT immediate, RAVLT delayed, or semantic fluency scores in the ADNI cohort; however, it was positively associated with RAVLT immediate, RAVLT delayed, and semantic fluency scores in our cohort. Additionally, both cohorts showed correlations between the ALPS index and CTh in multiple brain regions, but not in the right inferior temporal gyrus (ADNI cohort; p = 0.124) or left precuneus (our cohort; p = 0.609). Figures 3 shows the Pm of CTh in AD-related cortical regions to the relationship between ALPS index and executive function. Analysis of executive function, measured by the TMT-A score (Fig. 4A-C), showed that regional CTh was a significant mediator; its Pm was approximately 24.1–50.0% of the total effect in the ADNI cohort and 37.7–60.3% of the total effect in our cohort. CTh regions with significant mediating effects in both cohorts were the bilateral inferior parietal cortex, bilateral middle temporal gyrus, bilateral superior temporal cortex, and left pars opercularis. Analysis of the TMT-B score (Fig. 4D) showed that CTh regions with significant mediating effects in both cohorts were the bilateral fusiform gyrus, bilateral inferior parietal cortex, bilateral middle temporal gyrus, left inferior temporal gyrus, left pars opercularis, right rostral middle frontal gyrus, and right superior temporal cortex.Discussion and Conclusion
In this study, we used the ALPS index as an indicator of glymphatic function. Among patients with AD, the ALPS index was significantly associated with MMSE, TMT-A, and TMT-B scores in both cohorts. We speculated that the effect of the glymphatic system on cognitive outcomes was mediated by atrophy of these cortical regions. Our analysis confirmed that the association between the ALPS index and executive function (TMT-A and TMT-B) was fully mediated by CTh in the bilateral inferior parietal cortex, bilateral middle temporal gyrus, left pars opercularis, and right temporal cortex.Acknowledgements
This project was supported by the National Natural Science Foundation of China (81971602, 82160327, and 82271977), the Key Science and Technology Project of Hainan Province (ZDYF2021SHFZ239), the Hainan Academician Innovation Platform Fund, and the Hainan Province Clinical Medical Center. Parts of the data used in preparation of this manuscript were obtained from the ADNI database (adni.loni. usc.edu). As such, the investigators within the ADNI study contributed to the design and implementation of ADNI and/or provided data but did not participate in analysis or writing of this article. Data collection and sharing for this project was funded by the Alzheimer's Disease Neuroimaging Initiative (ADNI) (National Institutes of Health Grant U01 AG024904) and DOD ADNI (Department of Defense award number W81XWH-12-2-0012). ADNI is funded by the National Institute on Aging, the National Institute of Biomedical Imaging and Bioengineering, and through generous contributions from the following: AbbVie, Alzheimer’s Association; Alzheimer’s Drug Discovery Foundation; Araclon Biotech; BioClinica, Inc.; Biogen; Bristol-Myers Squibb Company; CereSpir, Inc.; Cogstate; Eisai Inc.; Elan Pharmaceuticals, Inc.; Eli Lilly and Company; EuroImmun; F. Hoffmann-La Roche Ltd and its affiliated company Genentech, Inc.; Fujirebio; GE Healthcare; IXICO Ltd.; Janssen Alzheimer Immunotherapy Research & Development, LLC.; Johnson & Johnson Pharmaceutical Research & Development LLC.; Lumosity; Lundbeck; Merck & Co., Inc.; Meso Scale Diagnostics, LLC.; NeuroRx Research; Neurotrack Technologies; Novartis Pharmaceuticals Corporation; Pfizer Inc.; Piramal Imaging; Servier; Takeda Pharmaceutical Company; and Transition Therapeutics. The Canadian Institutes of Health Research is providing funds to support ADNI clinical sites in Canada. Private sector contributions are facilitated by the Foundation for the National Institutes of Health (www.fnih.org). The grantee organization is the Northern California Institute for Research and Education, and the study is coordinated by the Alzheimer’s Therapeutic Research Institute at the University of Southern California. ADNI data are disseminated by the Laboratory for Neuro Imaging at the University of Southern California.References
1. Mestre H, Mori Y, Nedergaard M. The Brain's Glymphatic System: Current Controversies. Trends in neurosciences 2020; 43:458-466.
2. Ringstad G, Vatnehol SAS, Eide PK. Glymphatic MRI in idiopathic normal pressure hydrocephalus. Brain 2017; 140:2691-2705.
3. Hsu JL, Wei YC, Toh CH, et al. Magnetic Resonance Images Implicate That Glymphatic Alterations Mediate Cognitive Dysfunction in Alzheimer Disease. Annals of neurology 2023; 93:164-174. 4. Taoka T, Ito R, Nakamichi R, et al. Reproducibility of diffusion tensor image analysis along the perivascular space (DTI-ALPS) for evaluating interstitial fluid diffusivity and glymphatic function: CHanges in Alps index on Multiple conditiON acquIsition eXperiment (CHAMONIX) study. Jpn J Radiol 2022; 40:147-158.
5. Taoka T, Masutani Y, Kawai H, et al. Evaluation of glymphatic system activity with the diffusion MR technique: diffusion tensor image analysis along the perivascular space (DTI-ALPS) in Alzheimer's disease cases. Jpn J Radiol 2017; 35:172-178.
6.Kamagata K, Andica C, Takabayashi K, et al. Association of MRI Indices of Glymphatic System With Amyloid Deposition and Cognition in Mild Cognitive Impairment and Alzheimer Disease. Neurology 2022; 99:e2648-2660.
Figures