2594
Optimized 3D (b-M1-TE) Data Acquisition for Repeatable IVIM and R2 Quantification in the Liver1Radiology, University of Wisconsin-Madison, Madison, WI, United States, 2Medical Physics, University of Wisconsin-Madison, Madison, WI, United States
Synopsis
Keywords: Diffusion Acquisition, Quantitative Imaging, Liver, Perfusion, Modeling, Relaxometry, Velocity & Flow
Motivation: The intravoxel incoherent motion (IVIM) signal is known to depend on first-order motion moment (M1) and TE, which may contribute to observed poor precision of conventional (b-value only) IVIM quantification.
Goal(s): Design an optimized 3D (b-M1-TE) IVIM acquisition for precise (repeatable) IVIM and R2 quantification in the liver.
Approach: 3D (b-M1-TE) noise-optimized IVIM acquisitions were acquired using a test-retest approach. IVIM estimates were obtained using a recently proposed advanced fitting technique. Test-retest repeatability and interlobar agreement were evaluated.
Results: The optimized 3D (b-M1-TE) IVIM acquisition demonstrated moderate to good repeatability and interlobar agreement of IVIM and R2 estimates (coefficients of variation < 32.0%).
Impact: A noise-optimized 3D (b-M1-TE) IVIM acquisition is proposed for simultaneous and repeatable IVIM and R2 quantification in the liver. Accounting for M1 and TE dependencies in the IVIM signal may enable improved diagnostic performance and treatment monitoring of IVIM quantification.
Introduction
Intravoxel incoherent motion (IVIM) quantification using conventional methods suffers from fitting instability associated with separating multiple decaying signal components sampled along a single dimension (b-value). However, the IVIM signal also depends on the first-order motion moment (M1) due to perfusion effects1-3 and TE due to T2 relaxation,4-7 which may contribute to observed poor precision of conventional IVIM.8-15Recently, 2D (b-M1) noise-optimized IVIM data acquisitions and M1 dependent IVIM signal models have been proposed.1,3,16,17 The 2D (b-M1) acquisitions have demonstrated improved stability,3 repeatability,3,17 and reproducibility16 of IVIM quantification in the liver compared to conventional methods. Therefore, the purpose of this work was to design an optimized 3D (b-M1-TE) IVIM acquisition for simultaneous and repeatable IVIM and R2 (=1/T2) quantification by accounting for M1 and TE dependencies in the IVIM signal.
Methods
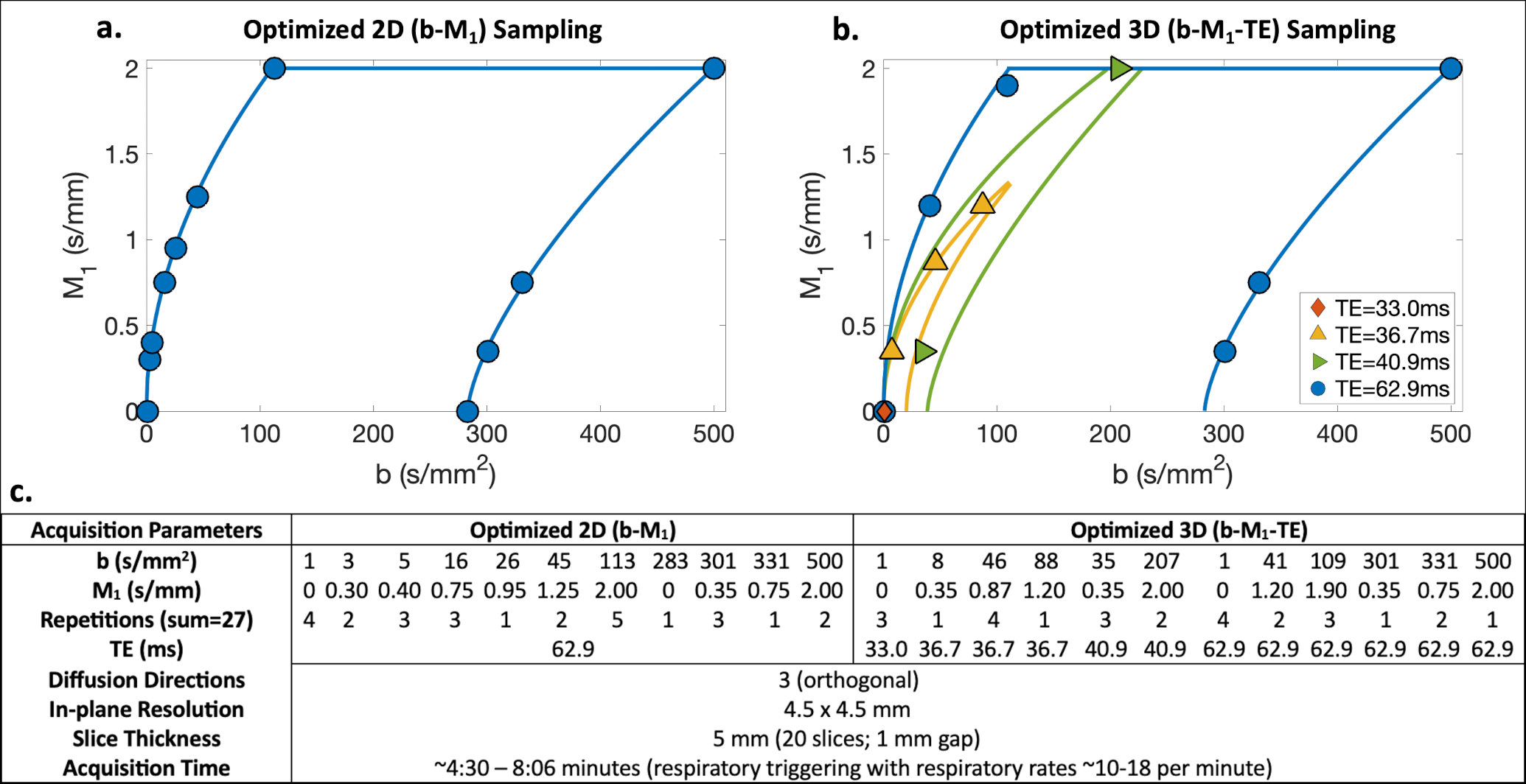
Acquisition optimization: Similar to a previously published procedure,3 Cramer-Rao lower bound optimization was performed to determine noise-optimized 2D (b-M1) and 3D (b-M1-TE) IVIM data samplings (i.e., points in b-M1-TE-space that can be realized using specifically-designed diffusion gradient waveforms) (Figure 1). Optimized samplings were determined based on the M1 dependent IVIM signal model1 with additional TE-dependent terms$$S(b,M_1,TE)=S_0[(1-F)e^{-bD}e^{-R_{2t}TE}+Fe^{-bD_b}e^{-M_1^2V_b^2/2}e^{-R_{2b}TE}]$$
where D is diffusion coefficient, F is perfusion fraction, Vb is blood velocity standard deviation, Db is diffusivity of blood (1.75x10-3 mm2/s),1,18 and R2t and R2b are tissue and blood transverse relaxation rates, respectively. During optimization, M1 was constrained to less than 2 s/mm to mitigate effects of physiological motion.
MR acquisition: With IRB approval and informed consent, five (n=5) healthy subjects underwent two liver MRI exams (3T Signa Premier, GE Healthcare) using a test-retest approach. The determined optimized 2D (b-M1) and 3D (b-M1-TE) IVIM samplings were acquired during each exam (acquisition parameters in Figure 1c).
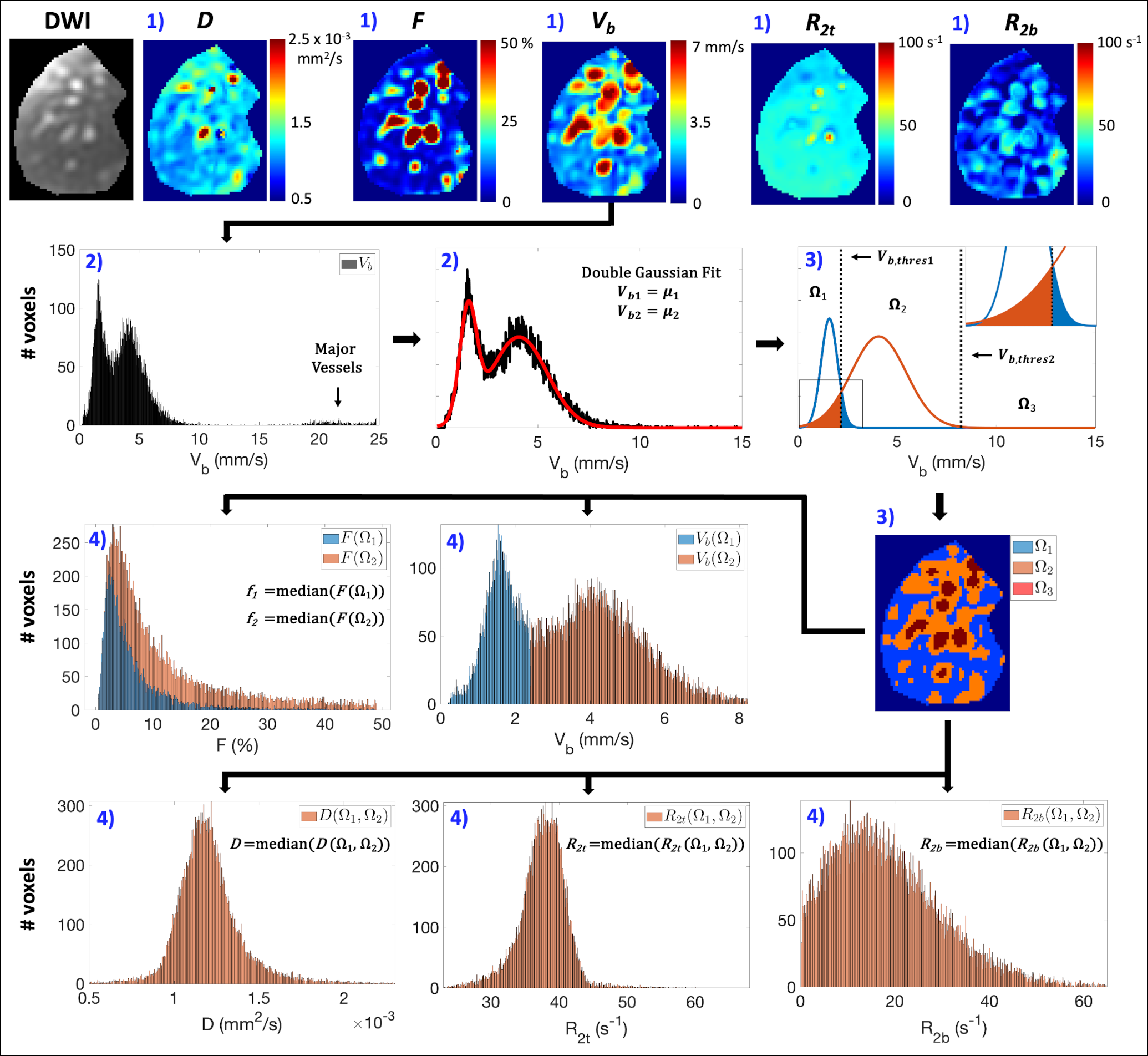
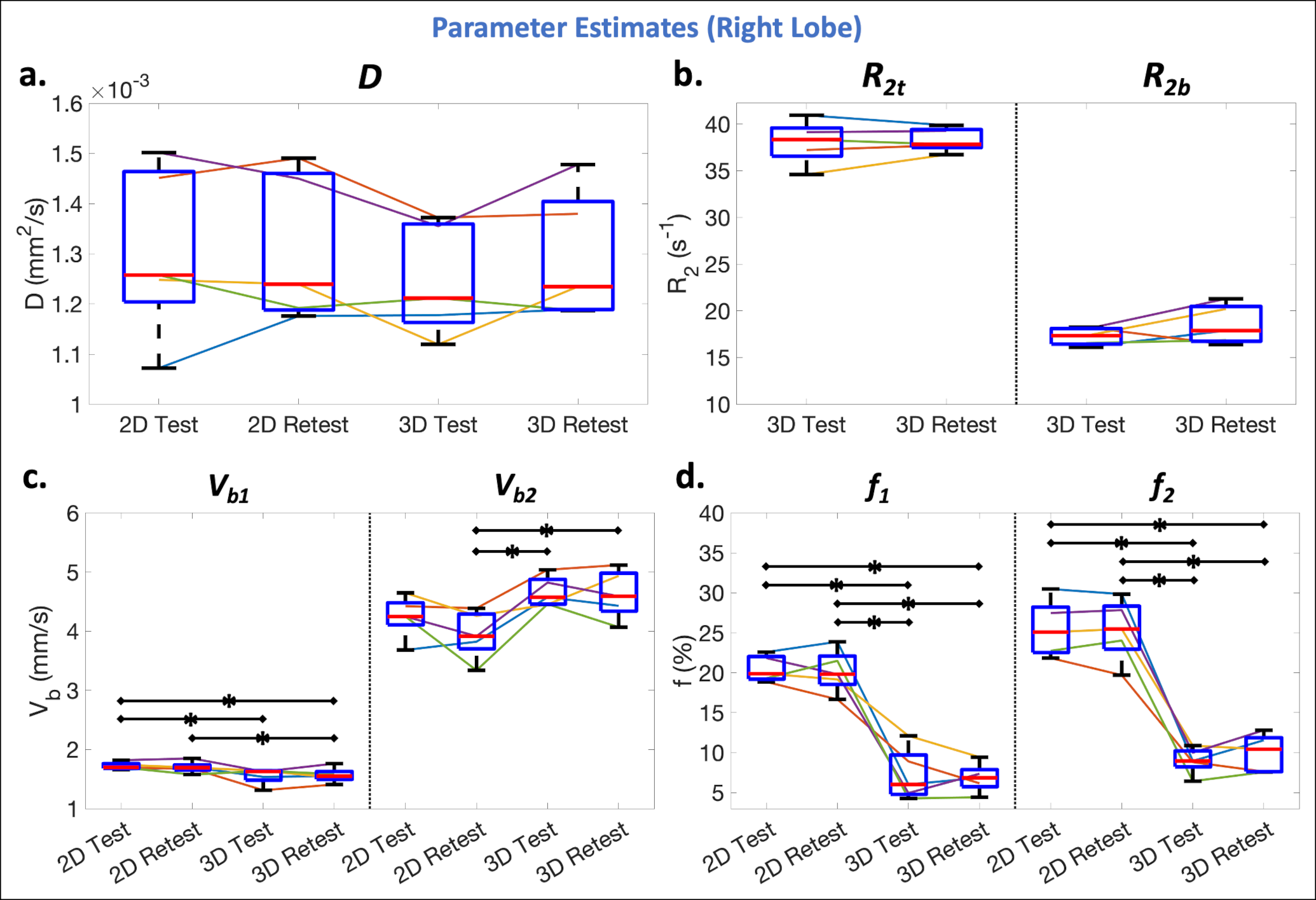
Data analysis: ROIs of the entire liver, including major vessels, were manually segmented and then divided into separate right and left lobe ROIs. For each ROI, IVIM estimates were obtained from voxelwise bi-exponential parameter maps using Blood Velocity standard deviation Distribution fitting,17 which estimates IVIM parameters within spatially distinct locations of the liver: Ω1 (slow perfusion), Ω2 (fast perfusion), and Ω3 (major vessels, excluded from further analysis) (see Figure 2 for details). IVIM estimates of Vb (Vb1 and Vb2), F (f1=median(F(Ω1) and f2=median(F(Ω2)), D (=median(D(Ω1,Ω2)), R2t (=median(R2t(Ω1,Ω2)), and R2b (=median(R2b(Ω1,Ω2)) were determined within Ω1 and Ω2.
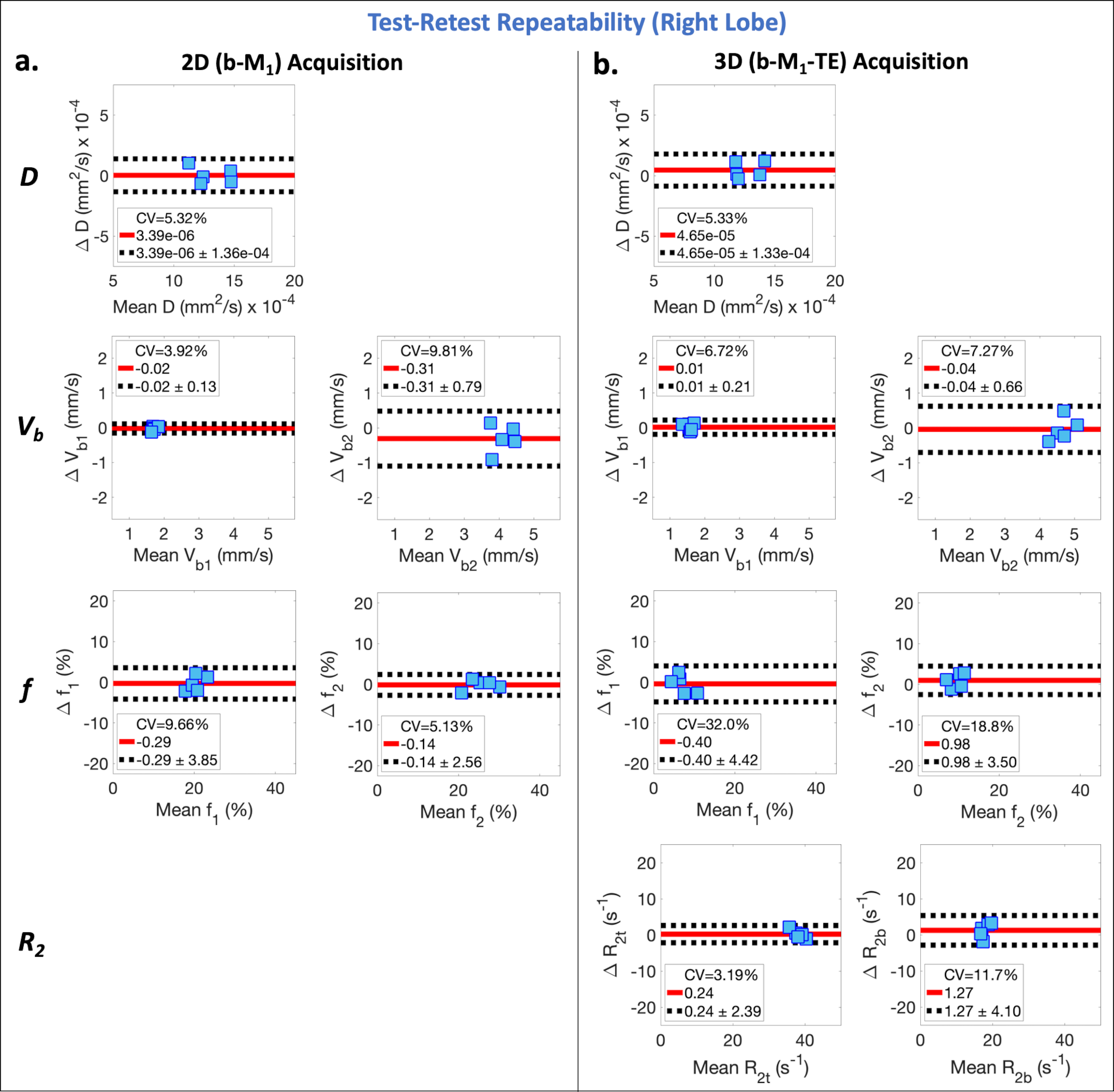
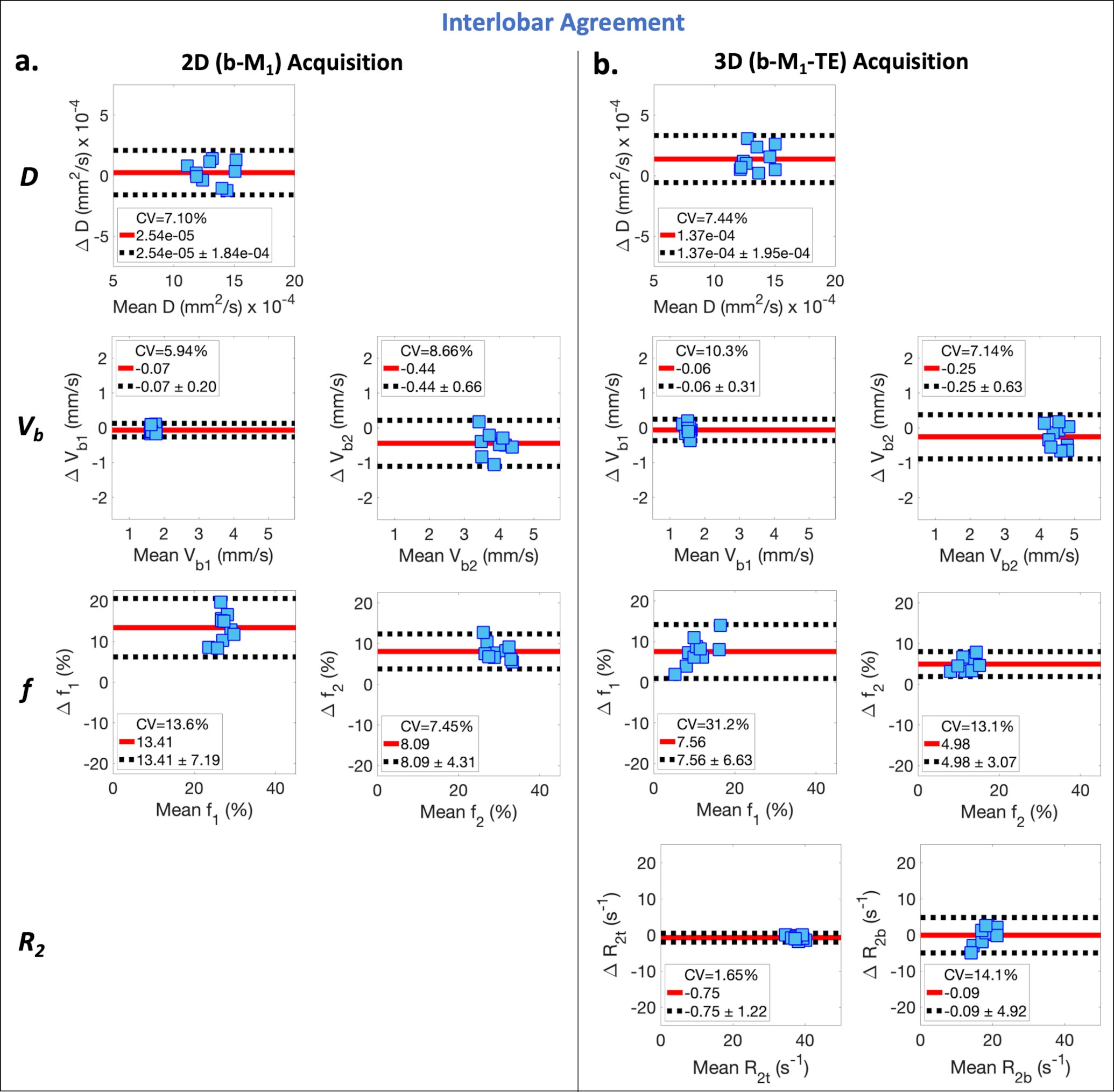
Test-retest repeatability and interlobar agreement were evaluated using Bland-Altman analysis (coefficients of variation (CV); mean differences (MDs)). Paired sample t-tests (significance level ⍺=0.05) were used to compare IVIM estimates across acquisitions (2D vs 3D; test vs retest).
Results
For the 2D and 3D acquisitions, good test-retest repeatability (Figure 3) and interlobar agreement (Figure 4) were observed in estimates of D (CV<7.44%; MD<1.95x10-4 mm2/s), Vb1 and Vb2 (CV<10.3%; MD<0.44 mm/s), and R2t and R2b (CV<14.1%; MD<1.27 s-1). Superior repeatability was observed for f1 and f2 using 2D acquisition (CV<9.66%; MD<0.29%) compared to 3D (CV>18.8%; MD>0.40%), and larger estimates were observed in the left lobe compared to the right lobe for both acquisitions (MD>4.98%).Comparing 2D and 3D estimates, lower Vb1 (p=0.02-0.11), higher Vb2 (p≤0.01-0.09), and lower f1 and f2 (p<0.001) were observed for the 3D acquisition (Figure 5).
Discussion
In this work, the optimized 3D (b-M1-TE) IVIM acquisition demonstrated moderate to good repeatability of IVIM quantification in the liver, while simultaneously quantifying R2 estimates in the same acquisition time as 2D (b-M1) acquisition and providing R2-corrected perfusion fraction estimates. Corrected perfusion fraction estimates were less repeatable likely due to the additional R2 estimation.Using conventional (b-value only) IVIM acquisitions and signal modeling, pseudo-diffusion estimates may depend on MR gradient hardware (e.g., maximum gradient strength) due to differences in M1,19 and perfusion fraction estimates may depend on the patient population (e.g. iron overload and/or contrast agent administration) due to differences in R2t and/or R2b. Further, signal dephasing caused by cardiac-induced compressive tissue motion leads to bias in IVIM estimates in the left lobe using conventional acquisitions.3,15,17,20 The proposed motion-robust (low M1), 3D (b-M1-TE) IVIM acquisition and signal modeling addresses these confounding factors and may enable improved diagnostic performance and treatment monitoring of IVIM quantification. However, possible confounding effects of diffusion encoding duration21-24 were not considered in this work, which may contribute to observed differences in Vb between the 2D and 3D acquisitions.
Limitations of this work include a small sample size of healthy volunteers only and large voxel sizes, which may be adequate for evaluation of diffuse liver disease, but inadequate for focal disease.
Conclusion
Optimized 3D (b-M1-TE) IVIM acquisition for simultaneous IVIM and R2 quantification demonstrated moderate to good repeatability and interlobar agreement in the liver.Acknowledgements
The authors acknowledge support from the NIH (R01-EB030497), the University of Wisconsin-Madison Office of the Vice Chancellor for Research and Graduate Education with funding from the Wisconsin Alumni Research Foundation, as well as from the UW Departments of Radiology and Medical Physics. GE Healthcare also provides research support to the University of Wisconsin.References
1. Ahlgren A, Knutsson L, Wirestam R, et al. Quantification of microcirculatory parameters by joint analysis of flow‐compensated and non‐flow‐compensated intravoxel incoherent motion (IVIM) data. NMR in Biomedicine. 2016;29(5):640-649.
2. Moulin K, Aliotta E, Ennis DB. Effect of flow‐encoding strength on intravoxel incoherent motion in the liver. Magnetic resonance in medicine. 2019;81(3):1521-1533.
3. Simchick G, Geng R, Zhang Y, Hernando D. b value and first‐order motion moment optimized data acquisition for repeatable quantitative intravoxel incoherent motion DWI. Magnetic Resonance in Medicine. 2022;87(6):2724-2740.
4. Jerome NP, d’Arcy JA, Feiweier T, et al. Extended T2-IVIM model for correction of TE dependence of pseudo-diffusion volume fraction in clinical diffusion-weighted magnetic resonance imaging. Physics in Medicine & Biology. 2016;61(24):N667.
5. Lemke A, Laun FB, Simon D, Stieltjes B, Schad LR. An in vivo verification of the intravoxel incoherent motion effect in diffusion‐weighted imaging of the abdomen. Magnetic resonance in medicine. 2010;64(6):1580-1585.
6. Führes T, Riexinger AJ, Loh M, et al. Echo time dependence of biexponential and triexponential intravoxel incoherent motion parameters in the liver. Magnetic resonance in medicine. 2022;87(2):859-871.
7. Riexinger AJ, Martin J, Rauh S, et al. On the field strength dependence of bi‐and triexponential intravoxel incoherent motion (IVIM) parameters in the liver. Journal of Magnetic Resonance Imaging. 2019;50(6):1883-1892.
8. Li YT, Cercueil J-P, Yuan J, Chen W, Loffroy R, Wáng YXJ. Liver intravoxel incoherent motion (IVIM) magnetic resonance imaging: a comprehensive review of published data on normal values and applications for fibrosis and tumor evaluation. Quantitative imaging in medicine and surgery. 2017;7(1):59.
9. Wu H, Liang Y, Jiang X, et al. Meta-analysis of intravoxel incoherent motion magnetic resonance imaging in differentiating focal lesions of the liver. Medicine. 2018;97(34)
10. Andreou A, Koh DM, Collins DJ, et al. Measurement reproducibility of perfusion fraction and pseudodiffusion coefficient derived by intravoxel incoherent motion diffusion-weighted MR imaging in normal liver and metastases. European radiology. 2013;23:428-434.
11. Cui Y, Dyvorne H, Besa C, Cooper N, Taouli B. IVIM Diffusion-weighted Imaging of the Liver at 3.0 T: Comparison with 1.5 T. European journal of radiology open. 2015;2:123-128.
12. Dyvorne HA, Galea N, Nevers T, et al. Diffusion-weighted imaging of the liver with multiple b values: effect of diffusion gradient polarity and breathing acquisition on image quality and intravoxel incoherent motion parameters—a pilot study. Radiology. 2013;266(3):920-929.
13. Cieszanowski A, Pasicz K, Podgórska J, et al. Reproducibility of intravoxel incoherent motion of liver on a 3.0 T scanner: free-breathing and respiratory-triggered sequences acquired with different numbers of excitations. Polish Journal of Radiology. 2018;83:437-445.
14. Chevallier O, Zhou N, He J, Loffroy R, Wáng YXJ. Removal of evidential motion-contaminated and poorly fitted image data improves IVIM diffusion MRI parameter scan–rescan reproducibility. Acta Radiologica. 2018;59(10):1157-1167.
15. Lee Y, Lee SS, Kim N, et al. Intravoxel incoherent motion diffusion-weighted MR imaging of the liver: effect of triggering methods on regional variability and measurement repeatability of quantitative parameters. Radiology. 2015;274(2):405-415.
16. Simchick G, Allen T, Hernando D. Multi-Scanner Reproducibility of IVIM Quantification in the Liver using Pseudo-Diffusion and Physical IVIM Signal Models. In Proceedings of the 31th Annual Meeting of ISMRM, Toronto. 2023.
17. Simchick G, Hernando D. Precision of region of interest‐based tri‐exponential intravoxel incoherent motion quantification and the role of the Intervoxel spatial distribution of flow velocities. Magnetic Resonance in Medicine. 2022;88(6):2662-2678.
18. Stanisz GJ, Li JG, Wright GA, Henkelman RM. Water dynamics in human blood via combined measurements of T2 relaxation and diffusion in the presence of gadolinium. Magnetic resonance in medicine. 1998;39(2):223-233.
19. Simchick G, Hernando D. Reproducibility of IVIM Quantification Across Diffusion Gradient Waveforms using Pseudo-Diffusion and Physical IVIM Signal Models. In Proceedings of the 30th Annual Meeting of ISMRM, London. 2022.
20. Li J, Zhang C, Cui Y, et al. Intravoxel incoherent motion diffusion-weighted MR imaging of the liver using respiratory-cardiac double triggering. Oncotarget. 2017;8(55):94959.
21. Wetscherek A, Stieltjes B, Laun FB. Flow‐compensated intravoxel incoherent motion diffusion imaging. Magnetic resonance in medicine. 2015;74(2):410-419.
22. Gurney‐Champion OJ, Rauh SS, Harrington K, Oelfke U, Laun FB, Wetscherek A. Optimal acquisition scheme for flow‐compensated intravoxel incoherent motion diffusion‐weighted imaging in the abdomen: An accurate and precise clinically feasible protocol. Magnetic resonance in medicine. 2020;83(3):1003-1015.
23. Iima M, Nobashi T, Imai H, et al. Effects of diffusion time on non-Gaussian diffusion and intravoxel incoherent motion (IVIM) MRI parameters in breast cancer and hepatocellular carcinoma xenograft models. Acta radiologica open. 2018;7(1):2058460117751565.
24. Wu D, Zhang J. Evidence of the diffusion time dependence of intravoxel incoherent motion in the brain. Magnetic resonance in medicine. 2019;82(6):2225-2235.
Figures