2591
Test-retest repeatability of intravoxel incoherent motion (IVIM) MRI in the cervical cord at 3T1Spinal Cord Injury Center, Balgrist University Hospital, Zurich, Switzerland, 2MR Research Collaborations, Siemens Healthcare Pty Ltd, Melbourne, Australia, 3CNRS, CRMBM, Aix-Marseille Univ, Marseille, France, 4CEMEREM, APHM, Hôpital Universitaire Timone, Marseille, France, 5Max Planck Institute for Human Cognitive and Brain Sciences, Leipzig, Germany
Synopsis
Keywords: IVIM, Spinal Cord
Motivation: High precision of intravoxel incoherent motion (IVIM) MRI parameters in the cervical cord can facilitate studies targeting perfusion impairment and substantiate clinical findings.
Goal(s): To determine the test-retest repeatability of IVIM in the cervical cord using four different common model fitting approaches.
Approach: Test-retest cardiac-gated IVIM acquisitions, sensitive to perfusion, were performed at 3T in 10 healthy subjects at C1-C3 levels. Reliability was assessed using relative test-retest differences, within-subject coefficients of variation and intraclass correlation coefficients.
Results: IVIM parameters in the cervical cord showed high repeatability at the group level in the white and grey matter.
Impact: The high test-retest repeatability of IVIM parameters in the cervical cord will help the interpretation of future clinical findings and support its relevance for applications in various neurological diseases affecting the spinal cord.
Introduction
Intravoxel incoherent motion (IVIM) is a diffusion-based MRI method, indirectly sensitive to blood perfusion1. It has been applied across various organs2–4, including the spinal cord5, but its reliability remains to be evaluated in this organ for interpretation of clinical findings. IVIM parameters’ precision depends on the fitting approach, with substantial variability reported across algorithms6–9. Determining IVIM measurements’ reliability is thus essential to substantiate IVIM findings in future clinical studies. This study aimed to investigate the test-retest repeatability of IVIM parameters in the white matter (WM) and grey matter (GM) of the cervical cord obtained with different modeling approaches, using either a one-step or two-step fitting method, based either on a voxel-wise or a region of interest (ROI)-wise fit.Methods
In vivo image acquisitionData were acquired in 10 healthy volunteers (mean age: 30.0 ± 5.4 years, 4 females) on a 3T system (MAGNETOM Prisma, Siemens Healthcare, Erlangen, Germany) with a Siemens Healthcare 64-channel head/neck RF coil. Participants were scanned twice, with a 15-minute break in and out of the scanner in-between. The protocol included a sagittal T2-weighted TSE sequence to localize the cervical levels, an axial T2*-weighted 3D multi-echo GRE10 to segment WM and GM (0.5×0.5 mm2 resolution), and a vendor product cardiac-gated IVIM axial 2D-RF spin-echo EPI ZOOMit sequence with a trigger delay of 100 ms, 0.9×0.9 mm2 resolution, 9 slices, 14 b-values ranging from 0 to 650 s/mm2 with an increment of 50 s/mm2, with 20 repetitions per b-value in three in-plane diffusion encoding directions. The IVIM acquisitions were split into forward and reverse phase encoding directions (5-min acquisition time) for subsequent distortion correction16. All scans were acquired in the cervical cord covering C1-C3 levels.
Image processing
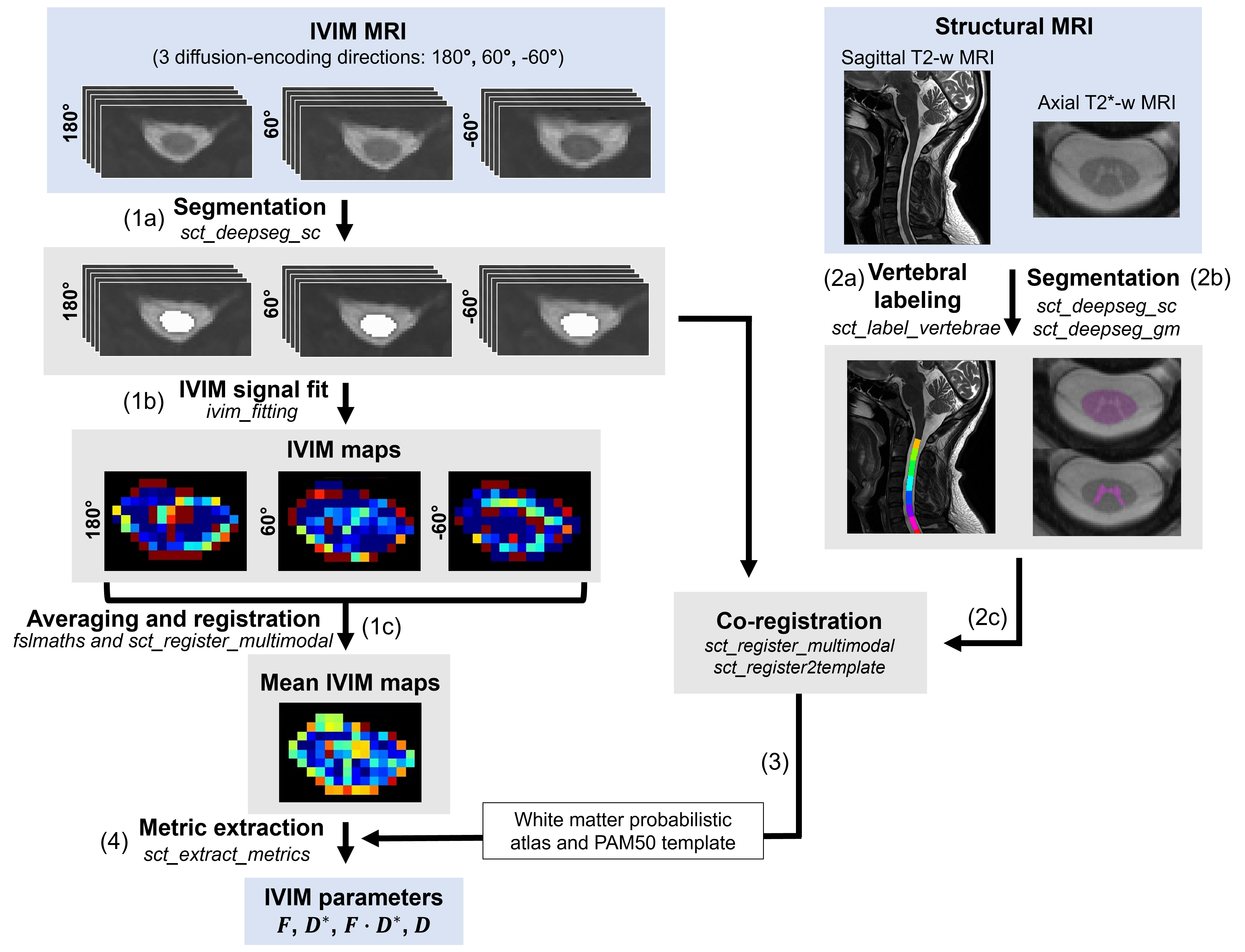
IVIM maps were generated with the IVIM toolbox5. Denoising11, removal of Gibbs artefacts12,13 (DIPY14), motion (sct_dmri_moco15) and distortion correction (FSL topup16) were conducted. The IVIM signal was described by the biexponential IVIM model1: $$S(b)=S_{0}e^{-bD}(Fe^{-bD^*}+1-F)$$ where $$$F$$$ is the microvascular volume fraction, $$$D^*$$$ is the pseudo-diffusion coefficient (providing information about blood velocity), $$$D$$$ is the diffusion coefficient, while $$$F·D^*$$$ has been shown to be sensitive to blood flow17.
Four different modeling methods were investigated, the one-step (estimation of all IVIM parameters based on all b-values) and two-step fit (estimation of $$$D$$$ first based on b-values above 400 s/mm2, followed by the fit of $$$F$$$ and $$$D^*$$$ in a second step), based on a voxel-wise (IVIM signal fitted in each voxel of the spinal cord segmentation) and ROI-wise fitting approach (IVIM signal averaged in the WM and GM separately and then fitted).
The IVIM images and maps were registered to the PAM50 template18/white matter atlas19 using the WM/GM segmentation from the T2*-weighted image, and IVIM parameters were extracted in subject space across C1-C3 levels (averaged across slices) in WM/GM (Figure 1).
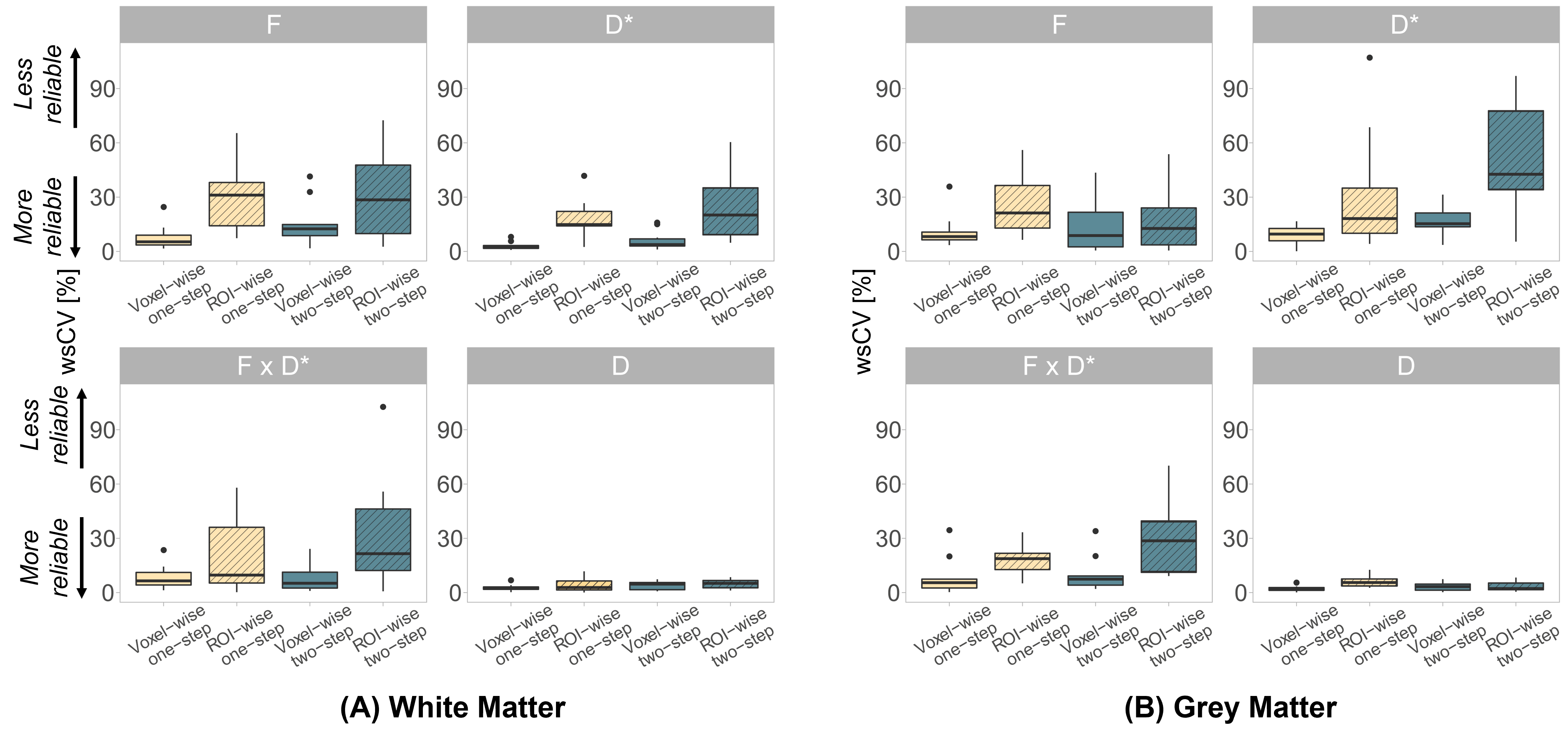
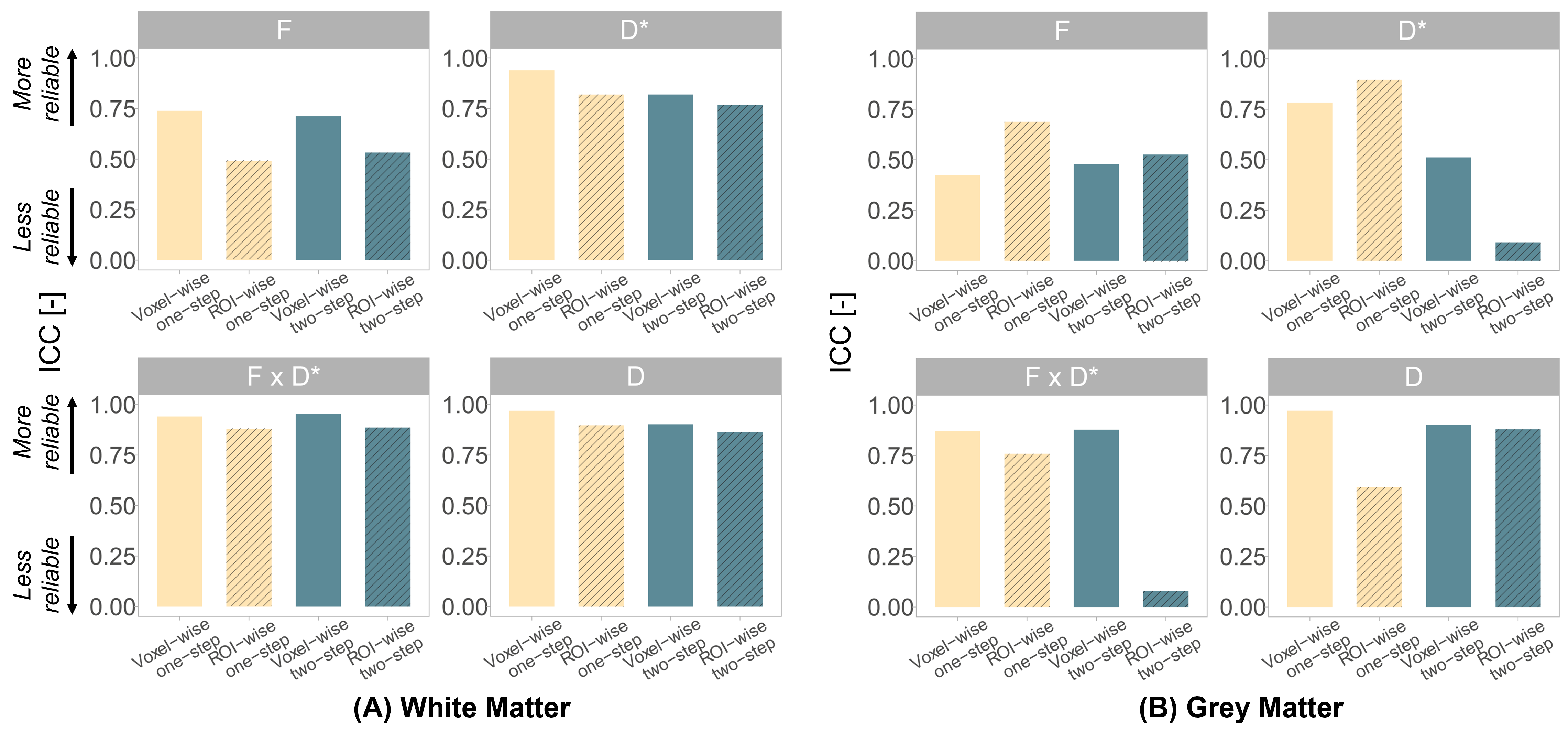
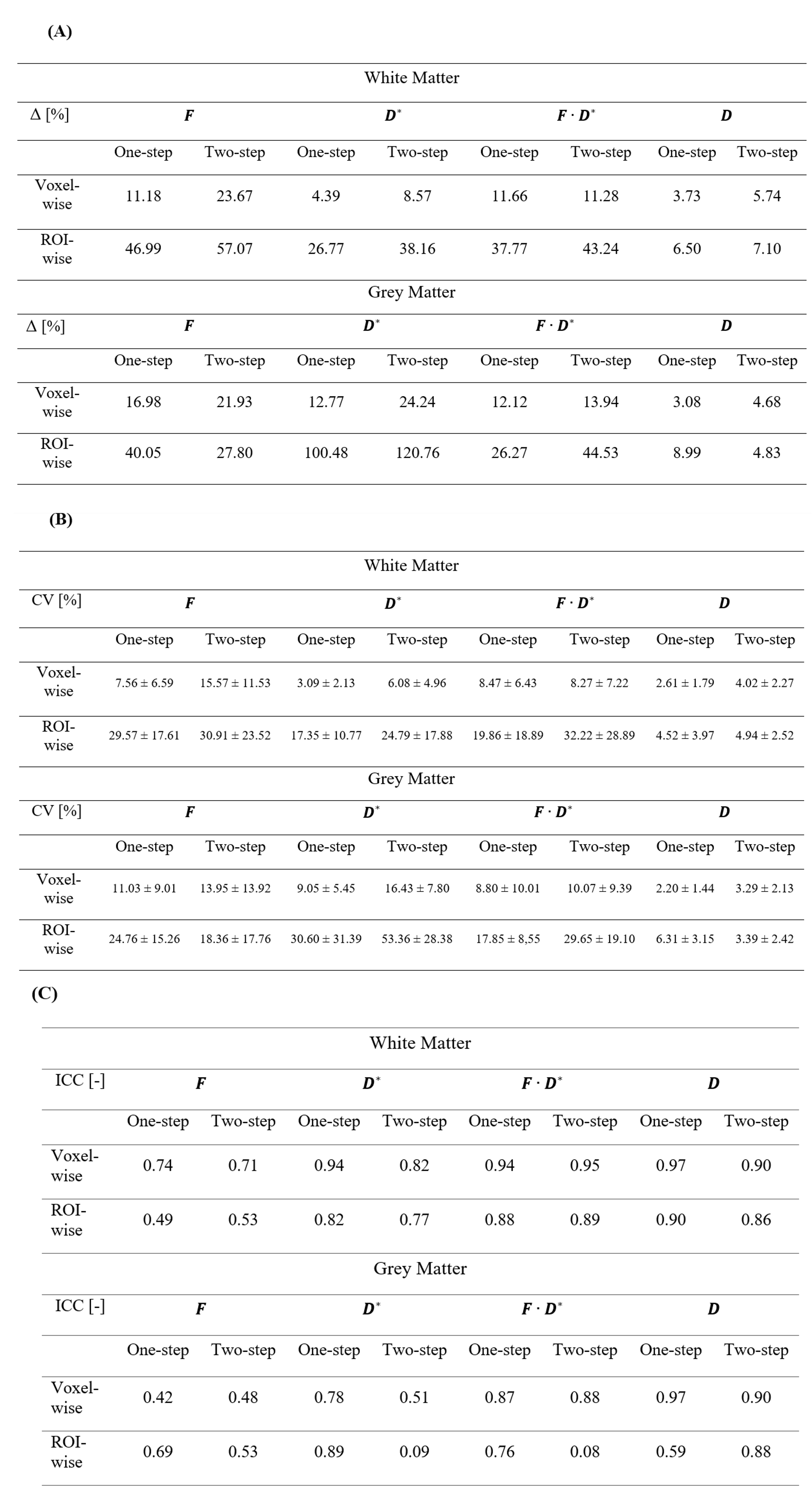
The reliability of the IVIM parameters was determined using relative test-retest differences, within-subject coefficients of variation (CV) and intraclass correlation coefficients (ICC)20, using the following scale for the ICC interpretation21–23: poor < 0.4 < fair < 0.6 < good < 0.75 < excellent. The statistical difference in CVs obtained with the different methods was assessed with a two-way ANOVA.
Results
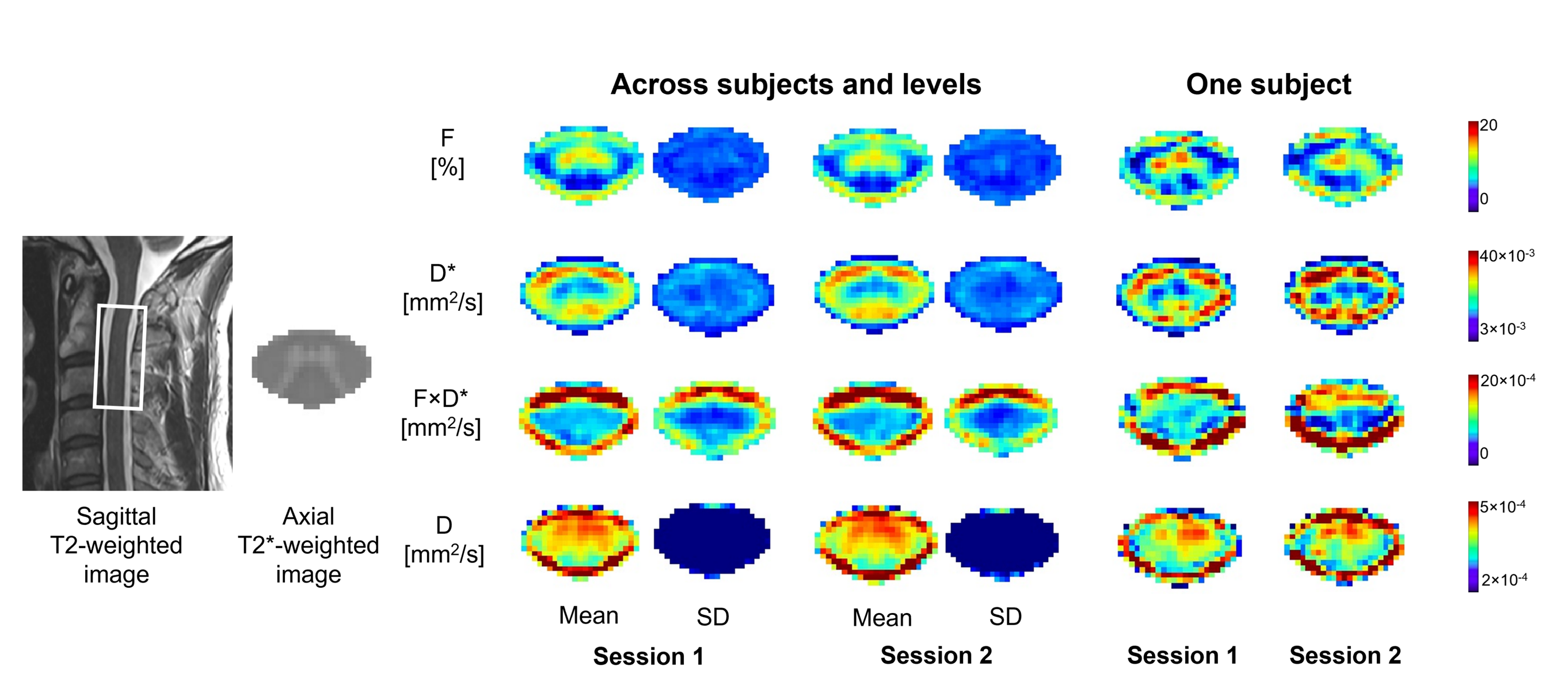
IVIM mean maps, averaged across subjects and levels, qualitatively indicated a good repeatability at the group level compared to the single subject maps (Figure 2). Average relative test-retest differences ranged between 3.73 and 23.67% in WM and 3.08% and 24.24% in GM with the voxel-wise fit ($$$F$$$:11.18%, $$$D^*$$$: 4.39% in WM; $$$F$$$: 16.98%, $$$D^*$$$: 12.77% in GM with voxel-wise one-step) (Table 1). A two-way ANOVA showed significantly lower within-subject CVs obtained using the voxel-wise fit compared to ROI-wise fit, whereas there was no significant difference between one-step or two-step method (Figure 3). The voxel-wise fit yielded higher ICC compared to the ROI-wise fit in the WM (Figure 4).Discussion
Higher GM intensity on average $$$F$$$ maps highlights the greater GM vascularization, in line with microangiography data24 and previous in-vivo reports5. Reduced ROI-wise fit repeatability may be attributed to inherent IVIM value variations, which may be more effectively addressed using a voxel-wise fit. Future work will aim at enhancing the efficiency of the protocol, by refining the b-values selection and number of repetitions, while maintaining accuracy.Conclusion
This study determined high repeatability of IVIM measurements in the cervical cord using four fitting approaches. The voxel-wise fit showed higher repeatability of IVIM parameters, independently of using the one-step or two-step algorithm. Robust IVIM metrics can facilitate studies targeting perfusion impairment and substantiate future clinical findings.Acknowledgements
The authors would like to thank all the participants who volunteered to take part in this study. This work is based on experiments performed at the Swiss Center for Musculoskeletal Imaging, SCMI, Balgrist Campus AG, Zurich, and methodological developments performed at the Centre de Résonance Magnétique Biologique et Médicale, CRMBM-CEMEREM, Aix-Marseille University/CNRS, Marseille, France. This project has received funding from the Wings for Life charity (No WFL-CH-19/20), Balgrist Stiftung 2021, International Foundation for Research (IRP-158), and from Hurka Wilhelm foundation UZH.References
1. Le Bihan D, Breton E, Lallemand D, Aubin ML, Vignaud J, Laval-Jeantet M. Separation of diffusion and perfusion in intravoxel incoherent motion MR imaging. Radiology. 1988;168(2):497-505. doi:10.1148/radiology.168.2.3393671
2. Lemke A, Laun FB, Klau M, et al. Differentiation of Pancreas Carcinoma From Healthy Pancreatic Tissue Using Multiple b-Values. Invest Radiol. 2009;44(12):769-775. doi:10.1097/RLI.0b013e3181b62271
3. Notohamiprodjo M, Chandarana H, Mikheev A, et al. Combined intravoxel incoherent motion and diffusion tensor imaging of renal diffusion and flow anisotropy. Magn Reson Med. 2015;73(4):1526-1532. doi:10.1002/mrm.25245
4. Seif M, Mani LY, Lu H, et al. Diffusion tensor imaging of the human kidney: Does image registration permit scanning without respiratory triggering? Journal of Magnetic Resonance Imaging. 2016;44(2):327-334. doi:10.1002/jmri.25176
5. Lévy S, Rapacchi S, Massire A, et al. Intravoxel Incoherent Motion at 7 Tesla to quantify human spinal cord perfusion: limitations and promises. Magn Reson Med. 2020;84(3):1198-1217. doi:10.1002/mrm.28195
6. Barbieri S, Donati OF, Froehlich JM, Thoeny HC. Impact of the calculation algorithm on biexponential fitting of diffusion-weighted MRI in upper abdominal organs. Magn Reson Med. 2016;75(5):2175-2184. doi:10.1002/mrm.25765
7. Meeus EM, Novak J, Withey SB, Zarinabad N, Dehghani H, Peet AC. Evaluation of intravoxel incoherent motion fitting methods in low‐perfused tissue. Journal of Magnetic Resonance Imaging. 2017;45(5):1325-1334. doi:10.1002/jmri.25411
8. Spinner GR, Federau C, Kozerke S. Bayesian inference using hierarchical and spatial priors for intravoxel incoherent motion MR imaging in the brain: Analysis of cancer and acute stroke. Med Image Anal. 2021;73:102144. doi:10.1016/j.media.2021.102144
9. Wang X, Song J, Zhou S, et al. A comparative study of methods for determining Intravoxel incoherent motion parameters in cervix cancer. Cancer Imaging. 2021;21(1):12. doi:10.1186/s40644-020-00377-0
10. Büeler S, Yiannakas MC, Damjanovski Z, Freund P, Liechti MD, David G. Optimized multi-echo gradient-echo magnetic resonance imaging for gray and white matter segmentation in the lumbosacral cord at 3 T. Sci Rep. 2022;12(1):16498. doi:10.1038/s41598-022-20395-1
11. Manjón J V., Coupé P, Concha L, Buades A, Collins DL, Robles M. Diffusion Weighted Image Denoising Using Overcomplete Local PCA. PLoS One. 2013;8(9):e73021. doi:10.1371/journal.pone.0073021
12. Kellner E, Dhital B, Kiselev VG, Reisert M. Gibbs-ringing artifact removal based on local subvoxel-shifts. Magn Reson Med. 2016;76(5):1574-1581. doi:10.1002/mrm.26054
13. Perrone D, Aelterman J, Pižurica A, Jeurissen B, Philips W, Leemans A. The effect of Gibbs ringing artifacts on measures derived from diffusion MRI. Neuroimage. 2015;120:441-455. doi:10.1016/j.neuroimage.2015.06.068
14. Garyfallidis E, Brett M, Amirbekian B, et al. Dipy, a library for the analysis of diffusion MRI data. Front Neuroinform. 2014;8:1-17. doi:10.3389/fninf.2014.00008
15. De Leener B, Lévy S, Dupont SM, et al. SCT: Spinal Cord Toolbox, an open-source software for processing spinal cord MRI data. Neuroimage. 2017;145:24-43. doi:10.1016/j.neuroimage.2016.10.009
16. Andersson JLR, Skare S, Ashburner J. How to correct susceptibility distortions in spin-echo echo-planar images: application to diffusion tensor imaging. Neuroimage. 2003;20(2):870-888. doi:10.1016/S1053-8119(03)00336-7
17. Le Bihan D, Turner R. The capillary network: a link between ivim and classical perfusion. Magn Reson Med. 1992;27(1):171-178. doi:10.1002/mrm.1910270116
18. De Leener B, Fonov VS, Collins DL, Callot V, Stikov N, Cohen-Adad J. PAM50: Unbiased multimodal template of the brainstem and spinal cord aligned with the ICBM152 space. Neuroimage. 2018;165:170-179. doi:10.1016/j.neuroimage.2017.10.041
19. Lévy S, Benhamou M, Naaman C, Rainville P, Callot V, Cohen-Adad J. White matter atlas of the human spinal cord with estimation of partial volume effect. Neuroimage. 2015;119:262-271. doi:10.1016/j.neuroimage.2015.06.040
20. McGraw KO, Wong SP. Forming inferences about some intraclass correlation coefficients. Psychol Methods. 1996;1(1):30-46. doi:10.1037/1082-989X.1.1.30
21. Cicchetti D V. Guidelines, criteria, and rules of thumb for evaluating normed and standardized assessment instruments in psychology. Psychol Assess. 1994;6(4):284-290. doi:10.1037/1040-3590.6.4.284
22. Cicchetti D V, Sparrow SA. Developing criteria for establishing interrater reliability of specific items: applications to assessment of adaptive behavior. Am J Ment Defic. 1981;86(2):127-137.
23. Fleiss J. Statistical Methods for Rates and Proportions. 2nd ed.; 1981.
24. Hassler O. Blood Supply to Human Spinal Cord. Arch Neurol. 1966;15(3):302. doi:10.1001/archneur.1966.00470150080013
Figures