2590
Validation of Motion-Robust Liver Diffusion MRI in Multi-Stiffness Pulsatile Motion Phantoms1Medical Physics, University of Wisconsin - Madison, Madison, WI, United States, 2Radiology, University of Wisconsin - Madison, Madison, WI, United States, 3Mechanical Engineering, University of Wisconsin - Madison, Madison, WI, United States
Synopsis
Keywords: Simulation/Validation, Contrast Mechanisms
Motivation: Quantitative diffusion MRI is a proposed marker for assessment of liver fibrosis. However, poor reproducibility and lack of highly controlled validation of liver ADC mapping precludes its clinical utilization.
Goal(s): Introduce hydrogel liver models with pulsatile motion and varying stiffness. These enable controlled validation of ADC accuracy and reproducibility across DWI acquisition parameters and physiological-mimicking motion.
Approach: Conventional monopolar (MONO) and motion-robust M1-optimized diffusion waveforms (MODI) were used to acquire DWI of three hydrogel liver models.
Results: MODI-DWI resulted in less biased DWI and ADC maps than MONO-DWI in areas of motion. A significant inverse relationship was observed between ADC and phantom stiffness.
Impact: Quantitative diffusion MRI may enable assessment of liver fibrosis. However, the relationship between diffusion parameters and stiffness requires controlled evaluation. The proposed phantom-based approach may help validate and optimize diffusion MRI of the liver and other abdominal organs.
Introduction
Liver fibrosis is the consequence of chronic liver injury. End-stage liver fibrosis is the primary cause of liver-disease related deaths.1-2 Magnetic Resonance Elastography (MRE) is validated for non-invasive estimation of liver stiffness, an indirect measurement of fibrosis.3-4 However, MRE requires additional hardware, has limited sensitivity in detecting early-stages of fibrosis, and cannot differentiate fibrosis from concurrent liver inflammation.5-6The apparent diffusion coefficient (ADC) obtained through diffusion weighted imaging (DWI) is a proposed marker for liver fibrosis. However, DWI of the liver is limited by several technical challenges, including the sensitivity of DWI to physiological motion, low signal-to-noise (SNR), and non-uniform acquisition parameters across studies.7-9 M1-optimized diffusion imaging (MODI) gradient waveforms enable robustness to pulsatile motion of the liver and have previously been reported to improve accuracy of ADC compared to conventional monopolar gradient waveforms (MONO).10 Furthermore, MODI-DWI paired with low-resolution imaging has previously shown improved accuracy of ADC for evaluation of diffuse liver disease.11 Despite early validation of low-resolution MODI-DWI in vivo, highly controlled evaluation of diffusion acquisition parameters has yet to be conducted. Hence, the purpose of this work is to validate motion-robust liver DWI across acquisition parameters and stiffness in a highly controlled liver model with pulsatile motion.
Methods
Motion Phantom:An anthropomorphic hydrogel liver model surrounds a pulsating tube with bifurcation, while being surrounded by rigid plastic walls. This setup mimics the cardiovascular-induced compressive tissue motion in the liver. The liver model was placed into the scanner bore and water was pumped through the system (Figure 1). Water was pumped at four flow velocities (0,0.5,1.0,1.5 L/min) to introduce deformation of the tube and adjacent hydrogel liver model. Three hydrogel liver models were fabricated with varying hydrogel compositions to create differing shear stiffness, quantified via MRE.
Image Acquisition:
DW images were acquired at 3.0T (Signa Premier, GE Healthcare) using an anterior array coil (Air Coil, GE Healthcare) and a posterior embedded table coil. Three hydrogel liver models were scanned using MONO and MODI diffusion gradient waveforms. MONO images were acquired with three orthogonal diffusion directions at two b-value pairs (b = [50,500] and b = [50,800] s/mm2, NEX = [2,4]). As usual in MONO, M1 increased substantially with b-value. MODI images were acquired with the same b-values, repetitions, diffusion directions, and a fixed M1 motion moment (0.628 s/mm) for all b-values. For each type of DW acquisition, two different spatial resolutions were acquired (2.8x2.8x6 & 6x6x6 mm3).
Analysis:
For each DWI acquisition, ADC maps were generated in MATLAB (R2020a) and subsequently analyzed in Horos (v3.3.6). ROIs were drawn on the averaged b = 50 s/mm2 images. ROIs were copied onto the corresponding ADC maps for measurement. Student’s t-tests evaluated the relationship between stiffness and ADC across the hydrogel liver models, and the differences in ADC across acquisition parameters.
Results
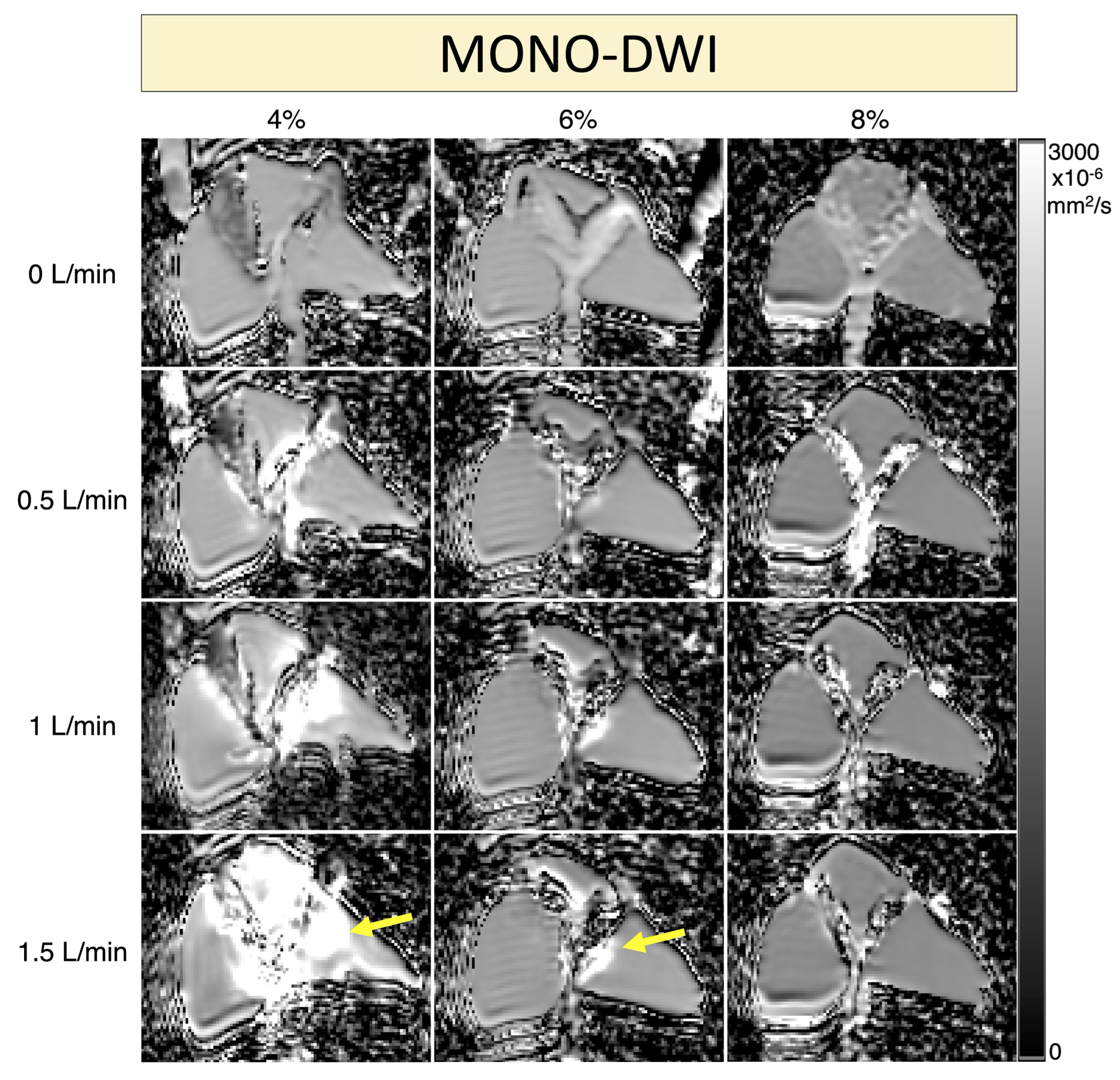
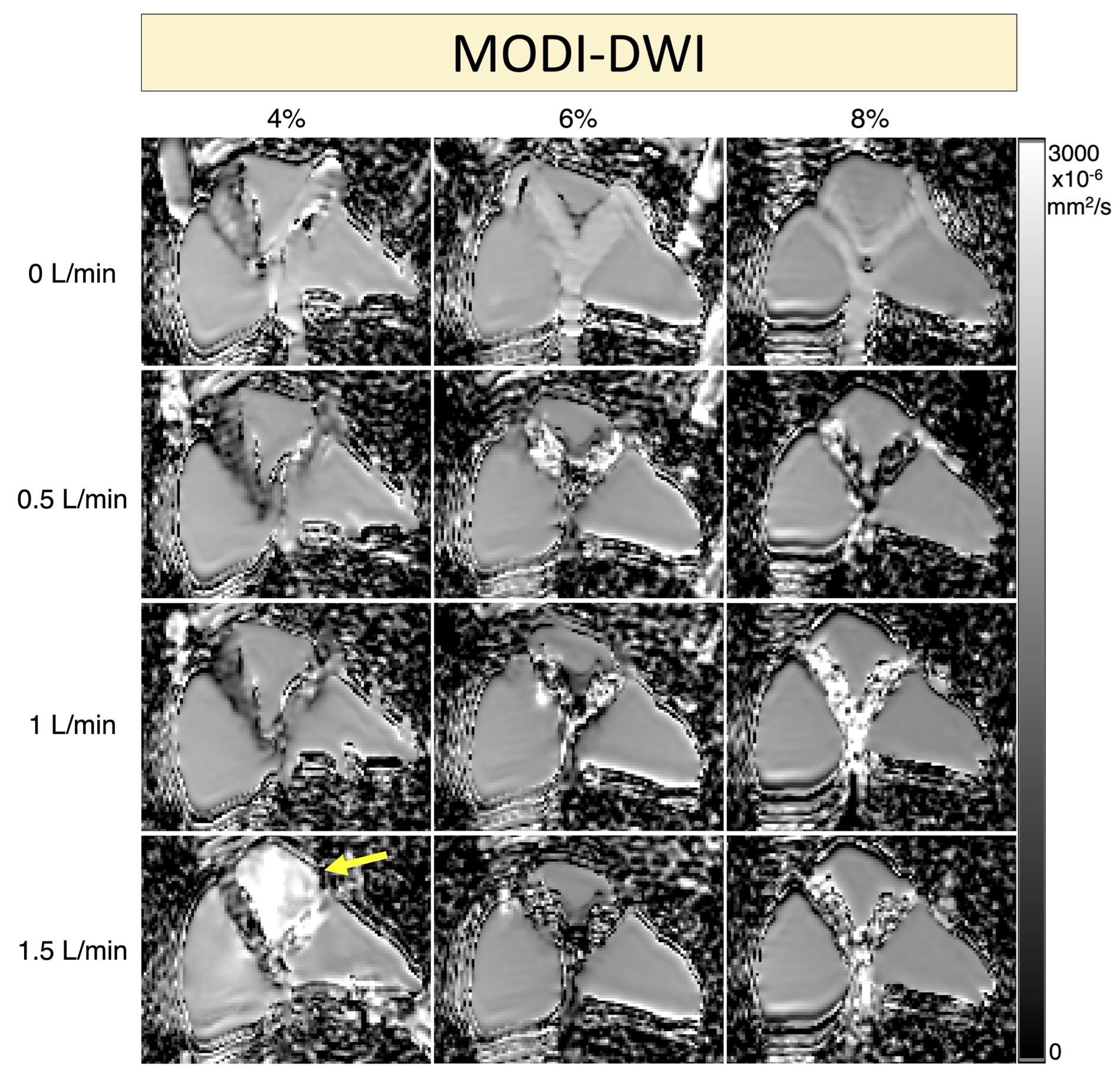
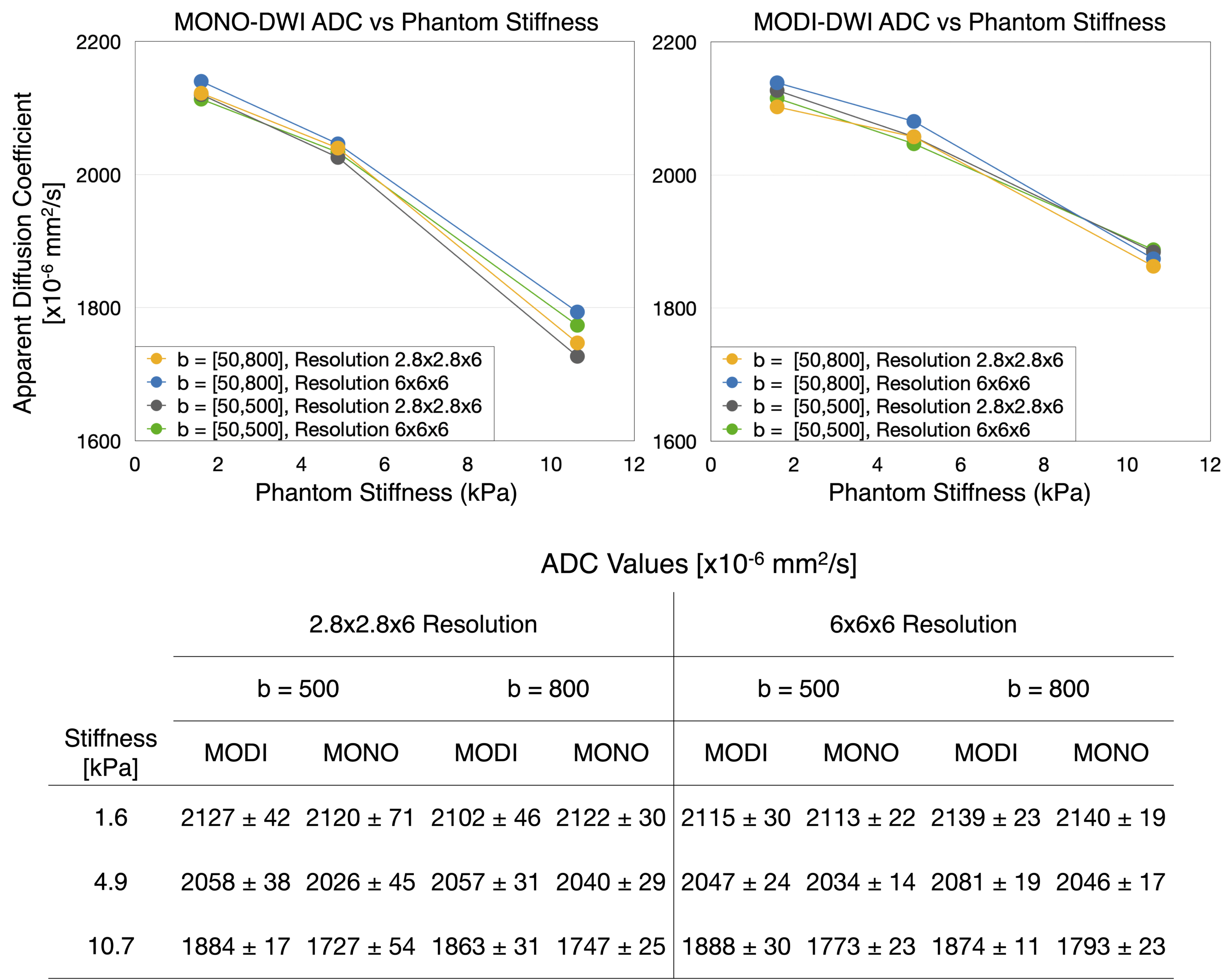
Figures 2-3 show ADC maps across flow rates and stiffness, from MONO-DWI and MODI-DWI, respectively. MONO suffered from large ADC bias at higher flow rates and in liver models with low stiffness. MODI suffered from localized ADC bias at the highest flow rate (1.5 L/min) in the lowest stiffness liver model, and minimal ADC bias in other models.Figure 4 plots MONO and MODI ADC versus phantom stiffness in the absence of flow. Each liver model exhibited different ADCs at baseline, dependent on the stiffness of the hydrogel. As stiffness increased, the ADC decreased (P = <0.01) for both MONO and MODI.
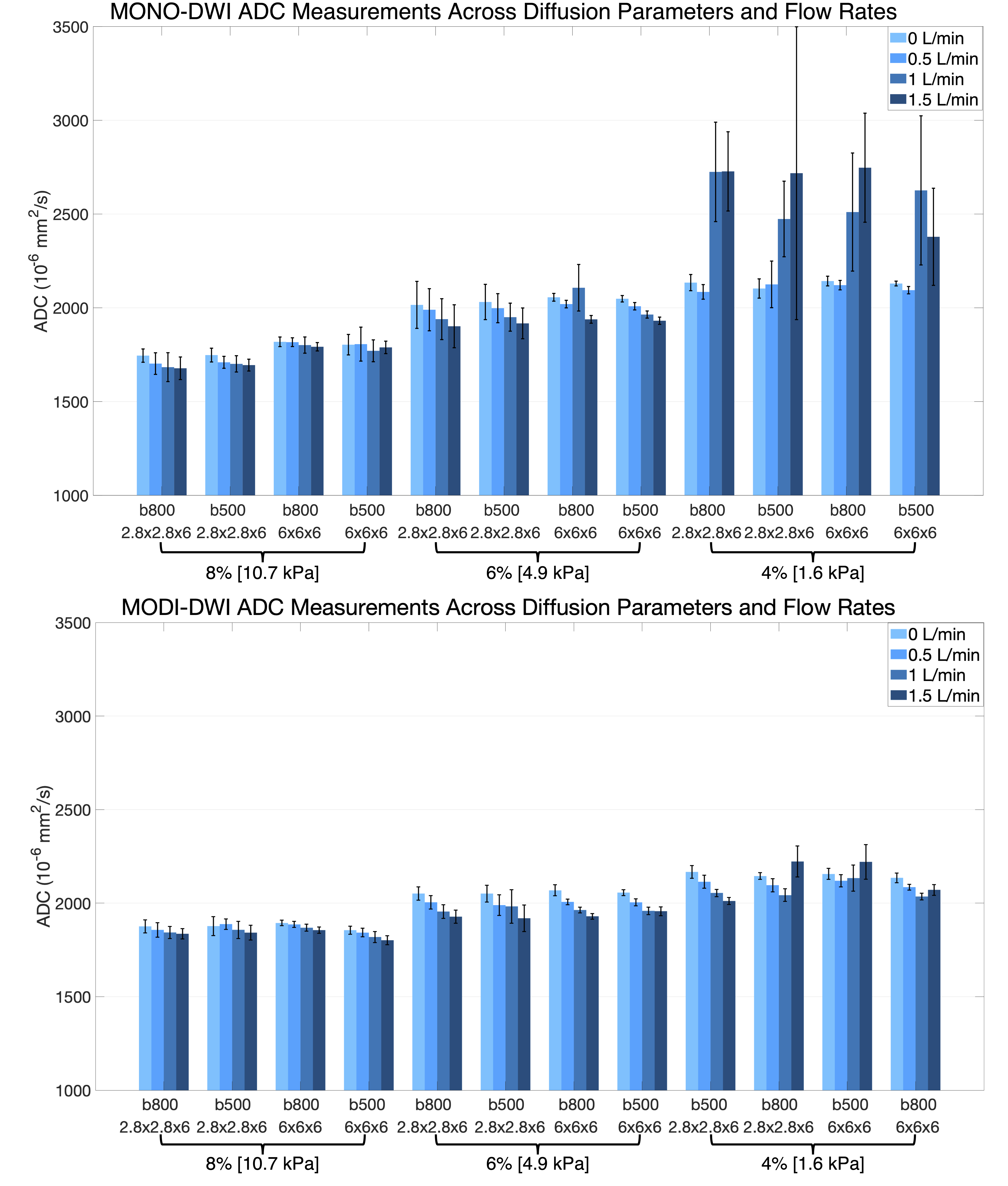
Figure 5 displays ADC values for all MONO and MODI DWI acquisitions across flow rates. MONO exhibited consistent ADC measurements at higher stiffness but suffered from large motion-induced ADC bias in the lowest stiffness hydrogel liver model. This trend was observed across b-value and resolution. MODI ADC measurements were consistent across all hydrogel liver models regardless of DW acquisition parameters.
Discussion
We validated motion-robust liver diffusion techniques in pulsatile motion phantoms with varying stiffness. We demonstrated that MODI ADC measurements in our liver model have an inverse relationship with MRE stiffness, a reduction in motion-induced ADC bias exists at higher stiffness, and improved motion-robustness using M1-optimized acquisitions. These highly controlled phantom results are well aligned with previously reported in vivo measurements.12-16Limitations of this study include the reliance of a pulsatile flow approach to induce compressive motion in the liver model, as the fluid used does not accurately mimic quantitative properties of blood.
Overall, our phantom validation approach with highly controlled compressive motion and stiffness may prove useful in development and validation of motion-robust DWI for assessment of liver fibrosis in vivo.
Acknowledgements
The authors acknowledge support from the NIH (R01 EB030497), from the University of Wisconsin-Madison Office of the Vice Chancellor for Research and Graduate Education with funding from the Wisconsin Alumni Research Foundation, as well as from the UW Departments of Radiology, Medical Physics, Mechanical Engineering. Also, GE Healthcare provides research support to the University of Wisconsin-Madison.
Research reported in this publication was supported by the National Cancer Institute of the National Institutes of Health under Award Number T32CA009206. The content is solely the responsibility of the authors and does not necessarily represent the official views of the National Institutes of Health.
References
1. Ge PS, Runyon BA. Treatment of Patients with Cirrhosis. N Engl J Med. 2016;375(8):767-777.
2. Sepanlou SG, Safiri S, Bisignano C, et al. The global, regional, and national burden of cirrhosis by cause in 195 countries and territories, 1990–2017: a systematic analysis for the Global Burden of Disease Study 2017. The Lancet Gastroenterology & Hepatology. 2020;5(3):245-266.
3. Huwart L, Peeters F, Sinkus R, et al. Liver fibrosis: non-invasive assessment with MR elastography. NMR in Biomedicine. 2006;19(2):173-179.
4. Huwart L, Sempoux C, Vicaut E, et al. Magnetic resonance elastography for the noninvasive staging of liver fibrosis. Gastroenterology. 2008;135(1):32-40.
5. Yin M, Woollard J, Wang X, et al. Quantitative assessment of hepatic fibrosis in an animal model with magnetic resonance elastography. Magn Reson Med. 2007;58(2):346-353.
6. Wegrzyniak O, Rosestedt M, Eriksson O. Recent Progress in the Molecular Imaging of Nonalcoholic Fatty Liver Disease. Int J Mol Sci. 2021;22(14):7348.
7. Dietrich O, Heiland S, Sartor K. Noise correction for the exact determination of apparent diffusion coefficients at low SNR. Magn Reson Med. 2001, 45(3), 448–453.
8. Kwee TC, Takahara T, Niwa T,et al. Influence of cardiac motion on diffusion-weighted magnetic resonance imaging of the liver. Magnetic Resonance Materials in Physics, Biology and Medicine, 2009, 22(5), 319-325.
9. Sasaki M, Yamada K, Watanabe Y, et al. Variability in absolute apparent diffusion coefficient values across different platforms may be substantial: a multivendor, multi-institutional comparison study. Radiology, 2009, 249(2), 624–630.
10. Zhang Y, Peña-Nogales Ó, Holmes JH, Hernando D. Motion-robust and blood-suppressed M1-optimized diffusion MR imaging of the liver. Magnetic resonance in medicine, 2019, 82(1), 302–311.
11. Volety S, Hernando D, Pirasteh A. Low Resolution Diffusion Weighted Imaging for the Assessment of Diffuse Liver Disease. Proc. Intl. Soc. Mag. Reson. Med. 31 (2022) Abstract 310.
12. Peña-Nogales Ó, Zhang Y, Wang X, et al. Optimized Diffusion-Weighting Gradient Waveform Design (ODGD) formulation for motion compensation and concomitant gradient nulling. Magnetic resonance in medicine, 2019, 81(2), 989–1003.
13. Aliotta E, Wu HH, Ennis DB. Convex optimized diffusion encoding (CODE) gradient waveforms for minimum echo time and bulk motion-compensated diffusion-weighted MRI. Magnetic resonance in medicine, 2017, 77(2), 717–729.
14. Shin MK, Song JS, Hwang SB, Hwang HP, Kim YJ, Moon WS. Liver Fibrosis Assessment with Diffusion-Weighted Imaging: Value of Liver Apparent Diffusion Coefficient Normalization Using the Spleen as a Reference Organ. Diagnostics (Basel, Switzerland), 2019, 9(3), 107.
15. Hennedige TP, Wang G, Leung FP, Alsaif HS, Teo LL, Lim SG, Wee A, Venkatesh SK. Magnetic Resonance Elastography and Diffusion Weighted Imaging in the Evaluation of Hepatic Fibrosis in Chronic Hepatitis B. Gut and liver, (2017), 11(3), 401–408.
16. Nasu K, Kuroki Y, Fujii H, Minami M. Hepatic pseudo-anisotropy: a specific artifact in hepatic diffusion-weighted images obtained with respiratory triggering. Magma (New York, NY, 2007), 20(4), 205–211.
Figures
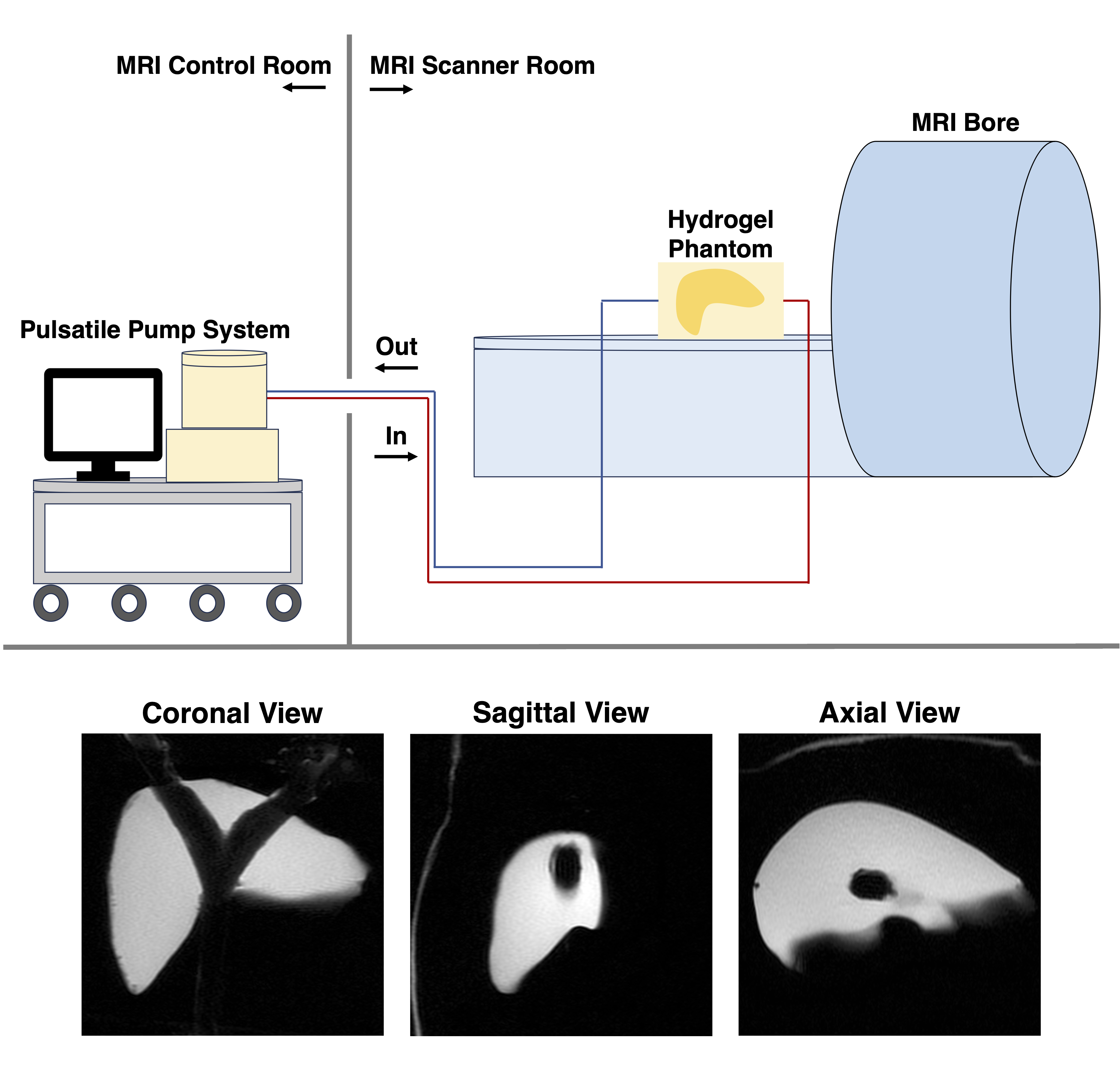
Figure 1: an anthropomorphic, in-vitro, MRI compatible hydrogel model of the liver. Setup in MRI room with a pulsatile flow circuit. Water is pumped through the system to induce pulsation from the inner tube, leading to compressive motion of the hydrogel model. T2-weighted images display appearance of phantom in three orthogonal planes.