2588
The utility of diffusion kurtosis imaging in assessing immunoglobulin G4-related kidney disease: a feasibility study1Department of Radiology, Peking Union Medical College Hospital, Chinese Academy of Medical Sciences and Peking Union Medical College, Beijing, China, 2Department of Nephrology, Peking Union Medical College Hospital, Chinese Academy of Medical Sciences and Peking Union Medical CollegeDepartment of Nephrology, Peking Union Medical College Hospital, Chinese Academy of Medical Sciences and Peking Union Medical College, Beijing, China, 3MR Research Collaboration, Siemens Healthineers Ltd., Beijing, China, 4MR Application Predevelopment, Siemens Healthcare GmbH, Erlangen, Germany
Synopsis
Keywords: DWI/DTI/DKI, Rare disease, Immunoglobulin G4; IgG4-related kidney disease
Motivation: Clinical diagnosis and assessment of immunoglobulin G4 (IgG4)-related disease is difficult. We explored whether diffusion kurtosis imaging (DKI) can resolve this difficulty.
Goal(s): To explore the feasibility of using DKI in the assessment of IgG4-related kidney disease (IgG4-RKD)
Approach: We measured the apparent diffusion coefficient (ADC) and DKI-derived parameters of the renal parenchyma, cortex, and medulla, then analyzed correlations between quantitative image parameters and clinical indicators.
Results: DKI-derived quantitative parameters were correlated with clinical indicators and demonstrated feasibility in the assessment of IgG4-RKD.
Impact: The DKI technique can help to detect IgG4-RKD lesions. DKI-derived quantitative parameters can assess IgG4-RKD clinical activity and facilitate evaluation of IgG4-RKD prognosis.
Introduction
Immunoglobulin G4 (IgG4)-related disease (IgG4-RD) is a chronic, inflammatory, fibrotic autoimmune disease that was first described in 2003 1-3. IgG4-related kidney disease (IgG4-RKD) is an important manifestation of IgG4-RD, which affects 7.0-24.6% of patients with IgG4-RD4, 5. Clinical manifestations in patients with IgG4-RKD are diverse and diagnosis is difficult5, 6. Imaging manifestations play an important role in confirming the diagnosis. Multiple studies have revealed that magnetic resonance imaging (MRI) is beneficial in the diagnosis of IgG4-RKD because of its high soft tissue resolution and multiparametric imaging features7, 8. However, conventional MRI sequences can only provide assessments of anatomical changes; they cannot provide quantitative data regarding changes in tissue microstructure. Diffusion kurtosis imaging (DKI) is an emerging imaging biomarker that can assess renal disease at the microstructural level9, 10. As an extension of conventional diffusion-weighted imaging (DWI), DKI uses non-Gaussian models for noninvasive assessment of tissue water diffusion coefficients11. DKI introduces a kurtosis parameter that represents the extent to water molecule diffusion in a tissue or lesion deviates from a Gaussian distribution11. This preliminary study was performed to explore the utility of DKI in assessing IgG4-RKD.Method
This study included 23 patients with IgG4-RKD who underwent bilateral renal MRI with conventional T1-weighted imaging (T1WI), conventional T2-weighted imaging (T2WI), and DKI sequences on a 3T scanner (MAGNETOM Skyra, Siemens Healthcare, Erlangen, Germany). Axial T1WI, T2WI, and DKI sequences were performed. DKI (with b-values of 0, 400, 800, 1200, and 1600 s/mm2) of both kidneys was performed in the axial plane using a research simultaneous multi-slice accelerated DWI sequence. The following parameters were used: repetition time=3000 ms, echo time=68 ms, field of view=400×325 mm2, slice thickness=4.0 mm, matrix=128×104, reconstructed voxel size=1.6×1.6×4.0 mm3, and acceleration factor=4 (generalized autocalibrating partially parallel acquisition [GRAPPA] acceleration factor=2 and slice acceleration factor=2). Two radiologists evaluated MR images to determine the renal lesion distribution patterns and signal intensities. The apparent diffusion coefficient (ADC) and DKI-derived parameters (mean kurtosis [MK] and mean diffusivity [MD]) of the renal parenchyma, cortex, and medulla were computed using a research software application (MR Body Diffusion Toolbox; Siemens Healthcare, Erlangen, Germany). For each parameter map, ROI mean values were measured by freehand delineation of the highest-level region of interest through the renal hilum. Correlations with clinical indicators (e.g., creatinine, estimated glomerular filtration rate [eGFR], IgG4, IgG, complement, and erythrocyte sedimentation rate [ESR]) were analyzed, and interclass correlation coefficients were used to evaluate measurement consistency.Result
IgG4-RKD showed bilateral (90.91%), multiple (95.24%), and wedge- or round-shaped renal parenchymal lesions (90.91%) with iso-intensity on T1WI (80.96%), hypo-intensity on T2WI (85.71%), and hyperintensity on ultrahigh b-value images (b=1600 s/mm2) (95.24%). ADC, MK, and MD values did not differ between left and right kidneys. There were no significant differences in MK and ADC values in the renal parenchyma, renal cortex, or renal medulla; however, MD values were higher in the renal cortex. There was a strongly negative correlation between eGFR and renal cortical MK (r=-0.66, p=0.002), a moderately positive correlation between IgG and renal parenchymal MK (r=0.50, p=0.023), and a weakly positive correlation between IgG4/IgG and parenchymal ADC (r=0.37, p=0.038). C4 was moderately positively correlated with MD in the renal parenchymal (r=0.51, p=0.118), and ESR was moderately positively correlated with renal parenchymal MK (r=0.58, p=0.005). With the exception of renal medullary MD, DKI parameters exhibited moderate to good agreement.Discussion
This study investigated imaging findings in patients with IgG4-RKD using conventional MRI sequences and DKI; it also assessed the utility of DKI quantitative parameters in assessing IgG4-RKD. The results showed that, in both kidneys, IgG4-RKD lesions tended to manifest as multiple wedge-shaped T1WI isointense and T2WI hypointense lesions, with restricted diffusion on DKI. Moreover, the DKI-derived renal parenchymal and renal cortical MK values were correlated with multiple clinical indicators, including eGFR, IgG, C4, and ESR. These findings suggested that DKI can facilitate comprehension of clinical status in patients with IgG4-RKD; it may assist with clinical decisions and prognosis prediction for such patients.Conclusion
This preliminary study evaluated MRI features of IgG4‑RKD and explored the utility of quantitative DKI metrics in assessing IgG4‑RKD. DKI could facilitate detection of kidney lesions, and DKI-derived quantitative parameters were correlated with multiple clinical indicators; knowledge of these relationships may facilitate assessments of disease activity or predictions of treatment prognosis.Acknowledgements
NoReferences
1 T. Saeki, S. Nishi, N. Imai, et al. Clinicopathological characteristics of patients with IgG4-related tubulointerstitial nephritis. Kidney international. 2010; 78(10):1016-23.
2 M. Lanzillotta, G. Mancuso, E. Della-Torre. Advances in the diagnosis and management of IgG4 related disease. BMJ. 2020; 369m1067.
3 H. Ren, N. Mori, S. Sato, et al. American College of Rheumatology and the European League Against Rheumatism classification criteria for IgG4-related disease: an update for radiologists. Jpn J Radiol. 2022; 40(9):876-893.
4 M. Kawano, T. Saeki, Y. Ubara, et al. Recent Advances in IgG4-Related Kidney Disease. Mod Rheumatol. 2022.
5 M. Salvadori, A. Tsalouchos. Immunoglobulin G4-related kidney diseases: An updated review. World J Nephrol. 2018; 7(1):29-40.
6 N. Seo, J.H. Kim, J.H. Byun, et al. Immunoglobulin G4-Related Kidney Disease: A Comprehensive Pictorial Review of the Imaging Spectrum, Mimickers, and Clinicopathological Characteristics. Korean J Radiol. 2015; 16(5):1056-67.
7 J. Ling, H. Wang, W. Pan, et al. Clinical and imaging features of IgG4-related kidney disease. Abdom Radiol (NY). 2020; 45(6):1915-1921.
8 B. Kim, J.H. Kim, J.H. Byun, et al. IgG4-related kidney disease: MRI findings with emphasis on the usefulness of diffusion-weighted imaging. Eur J Radiol. 2014; 83(7):1057-1062.
9 Y. Liu, G.M. Zhang, X. Peng, et al. Diffusion kurtosis imaging as an imaging biomarker for predicting prognosis in chronic kidney disease patients. Nephrol Dial Transplant. 2022; 37(8):1451-1460.
10 Y. Liu, G.M. Zhang, X. Peng, et al. Diffusional kurtosis imaging in assessing renal function and pathology of IgA nephropathy: a preliminary clinical study. Clin Radiol. 2018; 73(9):818-826.
11 A.B. Rosenkrantz, A.R. Padhani, T.L. Chenevert, et al. Body diffusion kurtosis imaging: Basic principles, applications, and considerations for clinical practice. J Magn Reson Imaging. 2015; 42(5):1190-202.
Figures
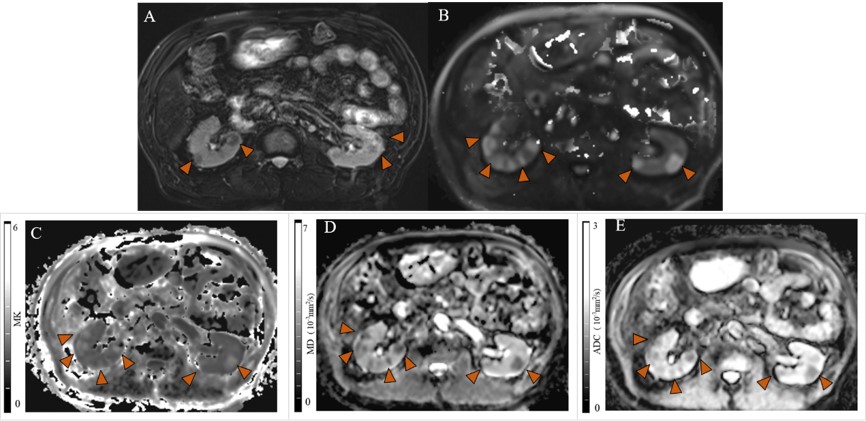
Figure 1 Representative images of IgG4-RKD lesions in a 66-year-old man. Multiple round lesions were evident in bilateral kidneys with hypo-intensity on T2WI (A) and hyperintensity on ultrahigh b-value images (b=1600 s/mm2) (B). The MK values of the lesions were increased (C); the MD and ADC values were decreased (D, E). The ultrahigh b-value images generated by DKI revealed more lesions than the results of T2WI.
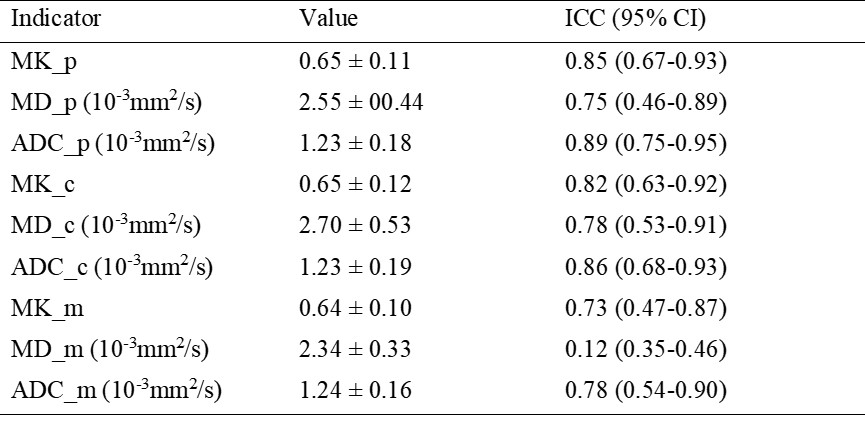
Figure 2 Mean values of quantitative renal image parameters and interobserver consistency for each parameter
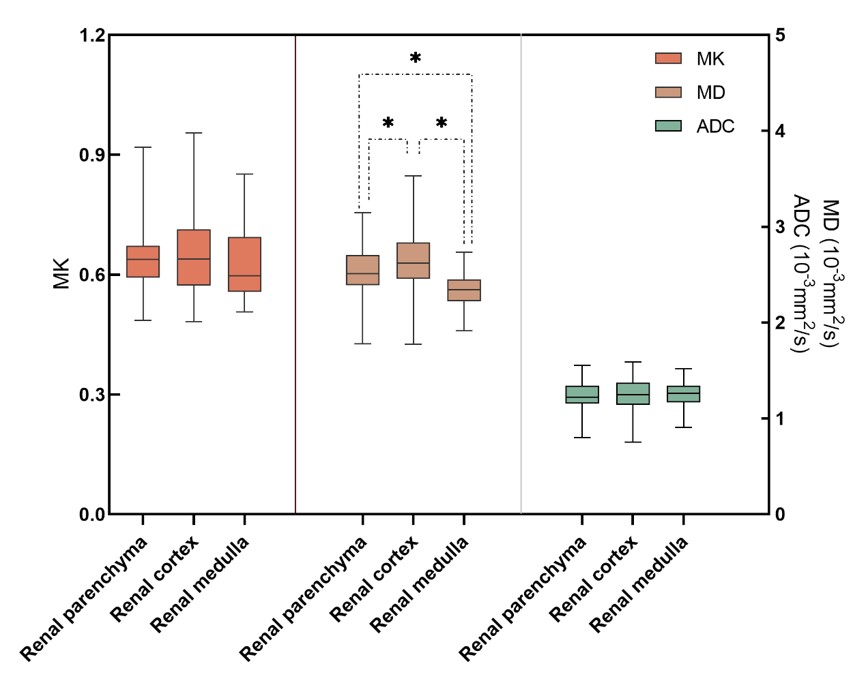
Figure 3 Comparison of ADC and various DKI parameters among renal parenchyma, cortex, and medulla. MK and ADC values did not significantly differ among renal cortex, renal parenchyma, and medulla. MD values were higher in renal cortex than in parenchyma or medulla. *p<0.05.
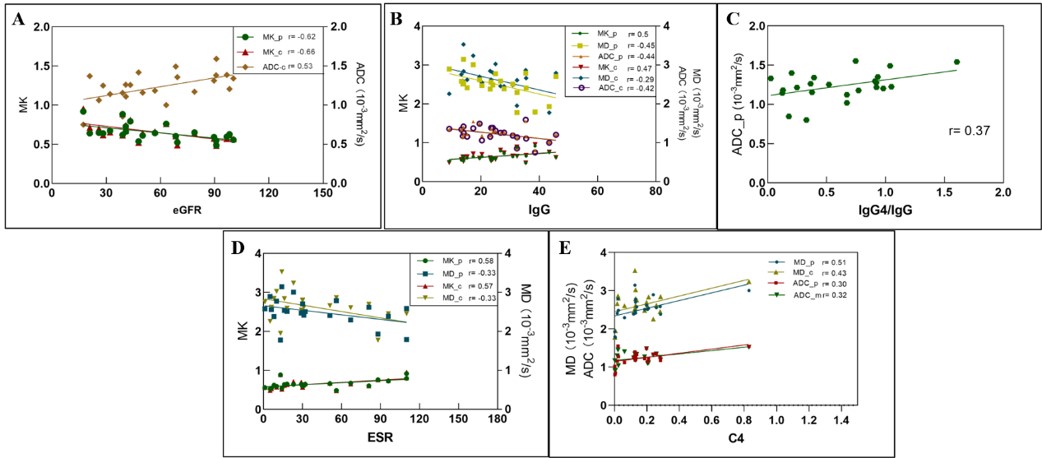
Figure 4 Scatterplots with regression lines showing correlations between clinical parameters and renal quantitative imaging parameters. MK_p: mean kurtosis in renal parenchyma; MD_p: mean diffusivity in renal parenchyma; ADC_p: apparent diffusion coefficient in renal parenchyma; MK_c: MK in renal cortex; MD_c: MD in renal cortex; ADC_c: ADC in renal cortex; ADC_m: ADC in renal medulla.
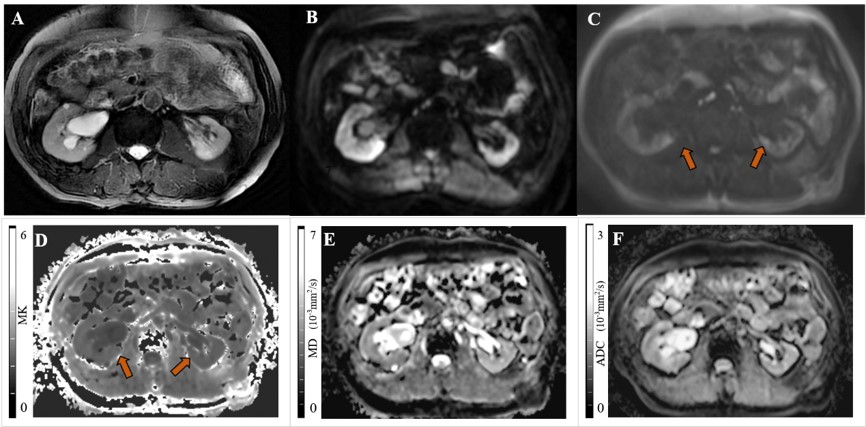
Figure 5 Comparison of lesion detection ability between DWI (b=800 s/mm2) and ultrahigh b-value images (b=1600 s/mm2) in a 60-year-old man. We found no abnormal lesions on T2WI (A), a suspicious locally increased signal on DWI (B), and a clearer patchy hyperintense signal on ultrahigh b-value images (C). The MK (D) value was slightly elevated, but the MD (E) and ADC (F) values were not significantly reduced.