2584
Characterization of Myocardial Microstructure using DT-CMR with Ultra-High-Performance Gradient Scanner in Healthy Subjects1Cardiovascular Innovation Research Center, Heart Vascular Thoracic Institute, Cleveland Clinic, Cleveland, OH, United States, 2Cardiovascular Medicine, Heart Vascular Thoracic Institute, Cleveland Clinic, Cleveland, OH, United States, 3Imaging Institute, Cleveland Clinic, Cleveland, OH, United States, 4Department of Biomedical Engineering, Case Western Reserve University and Cleveland Clinic, Cleveland, OH, United States
Synopsis
Keywords: Microstructure, Diffusion Tensor Imaging, Cardiac MRI, Healthy, Quantitative imaging
Motivation: DT-CMR has emerged as a promising tool for in vivo use in cardiovascular disease diagnosis, but there is currently a lack of reporting on the normal values for comparison.
Goal(s): Our goal was to evaluate the possibility of performing DT-CMR with an ultra-high-performance gradient MR scanner and provide normal ranges of quantitative DT-CMR measures.
Approach: Seventy healthy subjects underwent DT-CMR, and the results were compared between men and women.
Results: It is feasible to perform in vivo DT-CMR with a maximum gradient strength of 200 mT/m. The MD, FA and HAT for healthy subjects are (1.54±0.02) x10-3mm2/s, 0.33±0.005 and -0.81±0.02 º/% respectively.
Impact: Our study reports on the initial experience of conducting DT-CMR on a new investigational ultra-high-performance gradient scanner. The normal ranges of quantitative DT-CMR values are instrumental to establish baseline and distinguish the diseased from healthy in the future.
Introduction
Diffusion tensor cardiac MR (DT-CMR) is a promising imaging technique providing noninvasive measures of myocardial microstructure by mapping the diffusion of water molecules to quantify mean diffusivity (MD), fractional anisotropy (FA) and helix angle transmurality (HAT)1, 2. The knowledge of normal values for DT-CMR is crucial to the interpretation of results and future utilization of DT-CMR for patients with cardiovascular diseases3. With the recent introduction of an investigational MR system capable of achieving ultra-high maximum gradient strengths of up to 200 mT/m, there is new potential to enhance myocardial tissue characterization with DT-CMR, which would result in significant clinical impact. In this study, we aim to investigate the normal values of DT-CMR for men and women with data acquired on the new 3T MR system with ultra-high-performance gradients.Methods
Seventy healthy subjects (mean age 36 years, 35 female), recruited with approval from the institutional review board of Cleveland Clinic, were scanned using a 3T ultra-high-performance MR system (MAGNETOM Cima.X, Siemens Healthcare AG, Erlangen, Germany) with maximum possible gradient strength of 200 mT/m. All subjects were scanned under free-breathing conditions with a DT-CMR protocol consisting of a 2DRF zoomed diffusion prepared spin echo, FOV=350 mm, matrix=128 x 48, 5 slices, 8 mm slice thickness, TR=500 ms, 1 b0=50 s/mm2 acquisition, 12 diffusion directions at b=500 s/mm2, and 8 averages. Cardiac Function was analyzed with Segment (Medviso) and indexed to each subject’s body surface area. Global MD, FA and HAT values, calculated over the entire LV, were compared between men and women. Statistical analysis was performed with GraphPad Prism (v 9.5.1) and significance threshold for the analysis was determined at p < 0.05.Results
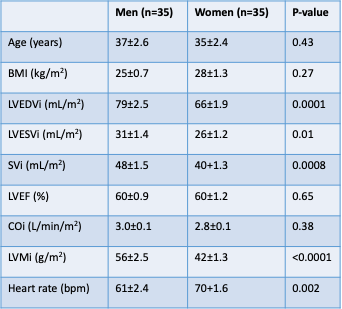
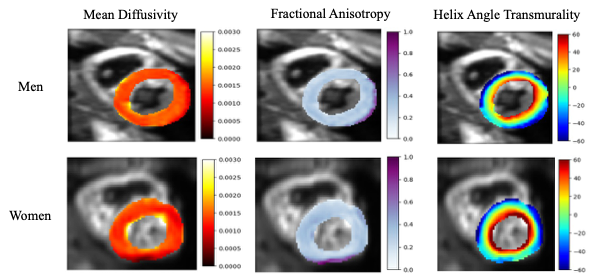
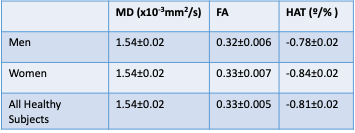
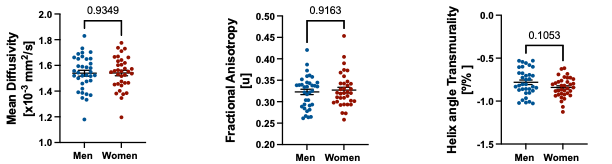
The baseline characteristics and CMR data of the study population are shown in Table 1. Women had significantly lower LVEDVi, LVESVi, SVi, and LVMi (66±1.9 mL/m2, 26±1.2 mL/m2, 40±1.3 mL/m2, and 42±1.3 g/m2, respectively) compared to men (79±2.5 mL/m2, 31±1.4 mL/m2, 48±1.5 mL/m2, and 56±2.5 g/m2, respectively). On the other hand, women are reported to have higher heart rate than men (70±1.6 bpm, and 61±2.4 bpm, respectively).Representative MD, FA and HAT maps are shown in Figure 1. MD, FA and HAT maps do not show significant differences between men and women. Table 2 reports the values of MD, FA and HAT for the healthy subjects as (1.54±0.02) x10-3mm2/s, 0.33±0.005 and -0.81±0.02 º/% respectively. Figure 2 is a quantitative comparison of DT-CMR parameters for men and women. MD, FA and HAT values for men are (mean ± SEM) (1.54±0.02) x10-3mm2/s, 0.32±0.006, and -0.78±0.02 º/% respectively, and (1.54±0.02) x10-3mm2/s, 0.33±0.007, and -0.84±0.02 º/% respectively for women. Men and women are found to have comparable MD, FA and HAT values.
Discussion
Our results suggest that while women have smaller LVEDVi, LVESVi, SVi, LVMi and higher heart rate compared to men, there are no significant differences in LVEF between sexes. The findings are consistent with existing literature that women have smaller hearts and higher heart rate than men4. This is important because it suggests that there are fundamental differences in cardiac anatomy between men and women.Furthermore, we did not find any significant differences in cardiac microstructure between healthy men and women specifically in global MD, FA and HAT. A limitation of this study could be that the number of individuals may not be large enough to reach significance. While other studies have reported similar MD, FA and HAT in healthy subjects, to the best of our knowledge, no studies have directly compared the effects of sex on cardiac microstructure in healthy individuals5. Moreover, we are the first to characterize myocardial microstructure with ultra-high maximum gradient strengths of up to 200 mT/m in healthy subjects. The findings of this study can be used as normal values for further comparison and exploration of cardiac microstructural changes in various myocardial disease states.
Conclusion
This study is the first to investigate the feasibility of DT-CMR in healthy subjects performed with an ultra-high-performance gradient MR system. Although no significant difference is discovered in MD, FA and HAT between men and women, the results are crucial to provide normal values for future clinical use. Future work will focus on continued assessment of the myocardial microstructure beyond MD, FA and HAT measures of patients and healthy subjects with this ultra-high-performance gradient scanner.Acknowledgements
They study is sponsored by NIHLBI (R01 HL151704, R01 HL159010) and NIBIB (R01 EB033853). In addition, I would like to thank the Imaging Institute and Cardiovascular Innovation Research Center for the support of this study.References
1. Gorodezky M, Scott AD, Ferreira PF, Nielles-Vallespin S, Pennell DJ, Firmin DN. Diffusion tensor cardiovascular magnetic resonance with a spiral trajectory: An in vivo comparison of echo planar and spiral stimulated echo sequences. Magn Reson Med. 2018;80(2):648-54. Epub 20171219. doi: 10.1002/mrm.27051. PubMed PMID: 29266435.
2. Nguyen CT, Buckberg G, Li D. Magnetic Resonance Diffusion Tensor Imaging Provides New Insights Into the Microstructural Alterations in Dilated Cardiomyopathy. Circulation: Cardiovascular Imaging. 2016;9(10):e005593. doi: 10.1161/circimaging.116.005593.
3. Kawel-Boehm N, Hetzel SJ, Ambale-Venkatesh B, Captur G, Francois CJ, Jerosch-Herold M, Salerno M, Teague SD, Valsangiacomo-Buechel E, Van Der Geest RJ, Bluemke DA. Reference ranges (“normal values”) for cardiovascular magnetic resonance (CMR) in adults and children: 2020 update. Journal of Cardiovascular Magnetic Resonance. 2020;22(1). doi: 10.1186/s12968-020-00683-3.
4. Prabhavathi K, Selvi KT, Poornima KN, Sarvanan A. Role of biological sex in normal cardiac function and in its disease outcome - a review. J Clin Diagn Res. 2014;8(8):BE01-4. Epub 20140820. doi: 10.7860/JCDR/2014/9635.4771. PubMed PMID: 25302188; PMCID: PMC4190707.
5. Scott AD, Nielles-Vallespin S, Ferreira PF, Khalique Z, Gatehouse PD, Kilner P, Pennell DJ, Firmin DN. An in-vivo comparison of stimulated-echo and motion compensated spin-echo sequences for 3 T diffusion tensor cardiovascular magnetic resonance at multiple cardiac phases. J Cardiovasc Magn Reson. 2018;20(1):1. Epub 20180103. doi: 10.1186/s12968-017-0425-8. PubMed PMID: 29298692; PMCID: PMC5753538.
Figures