2583
Qualitative and quantitative assessment of accelerated liver DWI using deep learning reconstruction in oncologic patients1MRI Unit, Royal Marsden Hospital, Sutton, United Kingdom, 2Division of Radiotherapy and Imaging, The Institute of Cancer Research, London, United Kingdom, 3MR Application Predevelopment, Siemens Healthineers AG, Erlangen, Germany
Synopsis
Keywords: Diffusion Reconstruction, Liver, deep learning reconstructed Diffusion Weighted Imaging
Motivation: Deep learning (DL) reconstructions can improve image quality and/or reduce acquisition time in diffusion-weighted imaging (DWI).
Goal(s): This study aims to assess, quantitatively and qualitatively, DL-accelerated DWI in 50 patients with colorectal cancer undergoing liver examinations.
Approach: Three DWI series are compared: a moderately-accelerated DL-DWI, a corresponding standard reconstruction and a highly-accelerated DL-DWI.
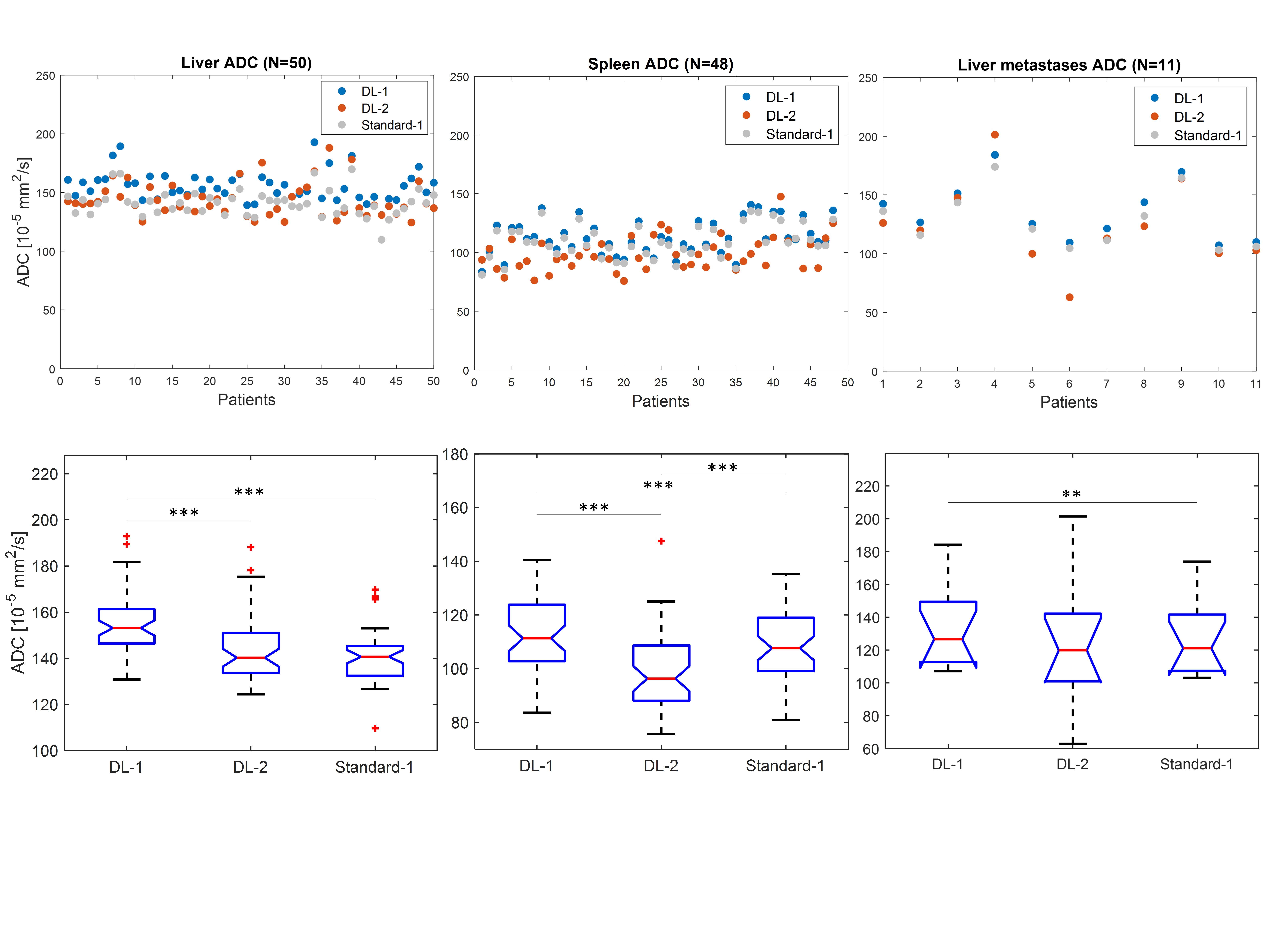
Results: The moderately-accelerated DL reconstruction method provides better image quality than a standard reconstruction. Its ADC estimates in liver, spleen and liver metastases are slightly higher than ADC estimates from the standard reconstruction.
Impact: This study evaluated DL-accelerated DWI in 50 patients undergoing liver examinations by comparing three DWI series. The moderately-accelerated acquisition with DL reconstruction provided better image quality versus the standard reconstruction; its ADC was slightly higher than the standard-based ADC.
Introduction
Diffusion-weighted imaging (DWI) is used for the detection and characterisation of focal liver lesions1 and assessment of treatment response2. However, widely-used liver DWI technique suffers from low signal-to-noise ratio (SNR) due to the relatively long echo times (TE) compared with the T2 relaxation time of the liver, and long acquisition times (from multiple signal averages). Recommendations suggest using the shortest possible TE as well as parallel imaging to improve SNR3. Recent developments in deep-learning (DL) reconstruction methods might allow reduction in acquisition times whilst maintaining good image quality4.This study assessed, quantitatively and qualitatively, accelerated DWI with DL reconstruction in the liver by comparing three DWI series: a moderately-accelerated DL-DWI (DL-1), a corresponding standard reconstruction of the same data (Standard-1) and a highly-accelerated DL-DWI (DL-2).
Methods
This prospective study was performed on a 1.5T MRI scanner (MAGNETOM Sola, Siemens Healthineers, Erlangen, Germany) using a DL research application package. The study was approved by a research ethics committee and included 50 patients with colorectal cancer (mean age 62 years, range 36-88 years, 26M) that gave verbal consent for two additional DWI acquisitions. The two DL-DWI sequences were acquired, for all patients, at the end of their routine clinical liver MR examination (that included administration of a hepatobiliary-specific contrast agent).The liver DWI protocol was: free breathing, axial echoplanar imaging using 3-direction trace-weighted diffusion encoding, bipolar encoding scheme, 3 b values (0, 150, 750 s/mm2), 40 slices and voxel 1.4x1.4x5mm3. The DL-1 sequence used parallel-imaging acceleration factor 2, TE/TR=67/9500ms, and 1/1/4 signal averages per b value, acquired in 2:59 minutes. The faster sequence (DL-2), acquired in 1:43 minutes, had an acceleration factor 3, a reduced TE/TR= 63/7900ms, and 1/1/2 averages per b value. DL reconstruction5 was based on a variational network trained on DWI data acquired in healthy volunteers and which alternates between data consistency steps and learned regularization steps. The slower sequence was also reconstructed with a standard, non-DL algorithm (Standard-1) for direct comparison.
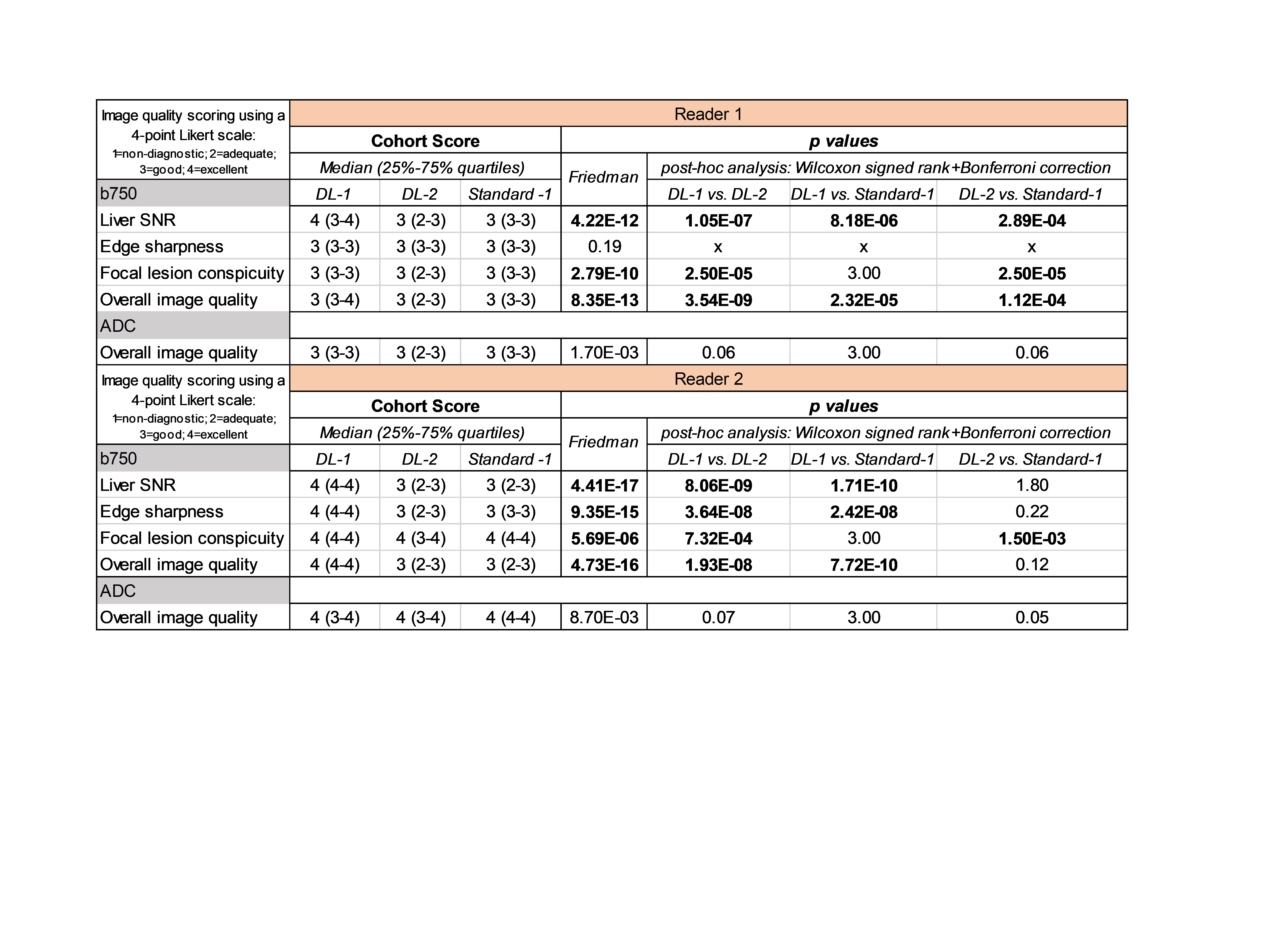
Image quality of all three series was assessed independently by two blinded radiologists using a four-point Likert scale (4=excellent). Four features were scored on b750 image (signal-to-noise ratio, sharpness, lesion conspicuity and overall quality) and one on ADC map (overall quality). Cohort median scores for each feature were calculated per series and reader. Median scores between series were compared using a Friedman non-parametric test (Matlab, R2019a, MathWorks, Natick, MA), and post-hoc analysis (pairwise Wilcoxon tests with Bonferroni correction). A p-value <0.05 was considered statistically significant.
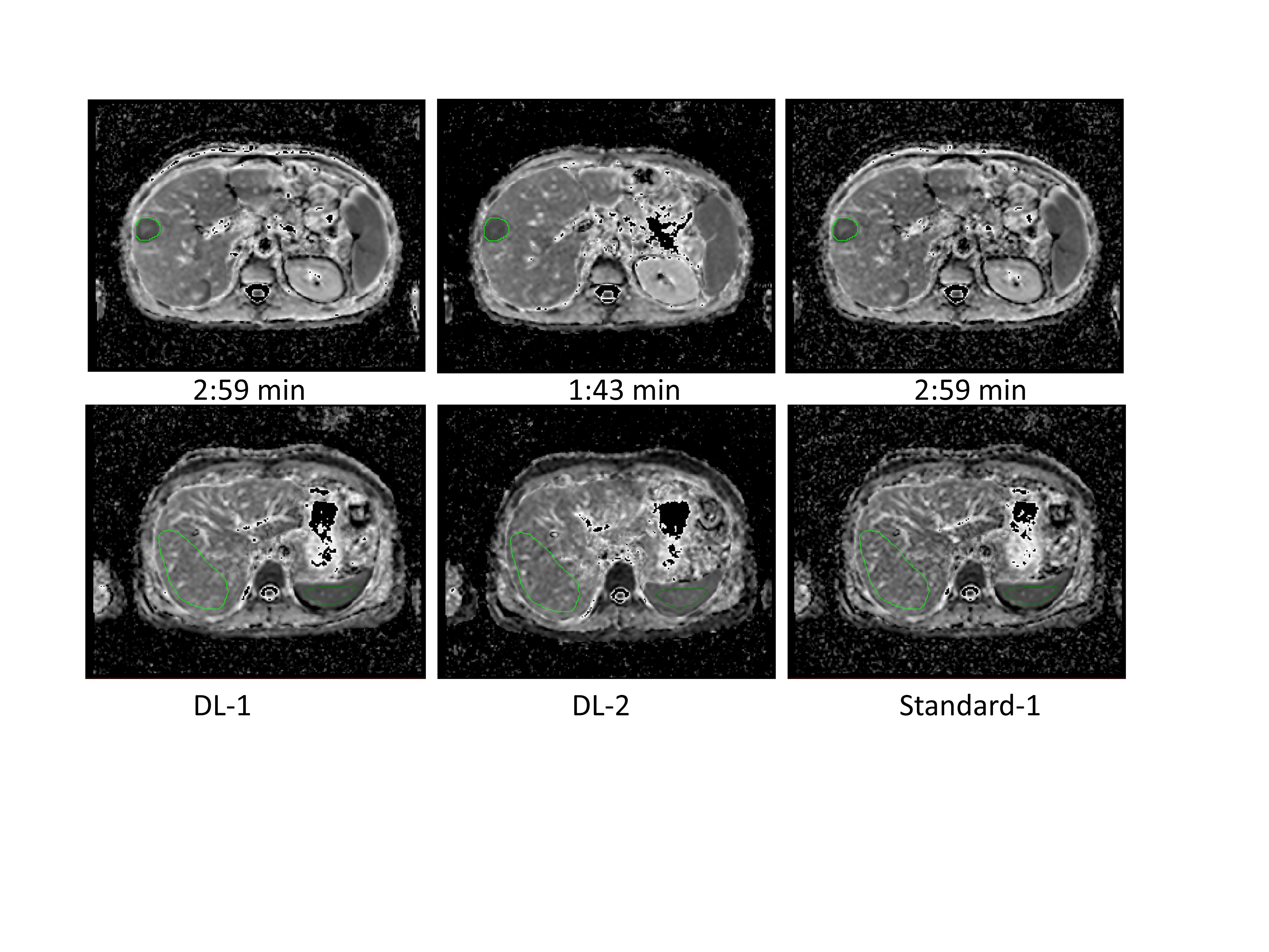
Region of interest (ROI) based ADC measurements for all three series were performed at three locations: liver, spleen and liver metastases. ADC measurements in liver/spleen were derived from a single slice that allowed ROI delineation for both organs in an area that was least impacted by motion, large blood vessels or tumoral tissue (Fig.1). Volumetric tumour ADC (average over multiple slices) was measured from patients with a lesion diameter ≥2cm; one single lesion per patient has been considered in an area not affected by motion. Patient-specific ROIs were matched across the three ADC maps for each organ location. Differences in median values of ADC across the three DWI series were assessed, for each anatomical location, using the Friedman test and post-hoc analysis.
Results
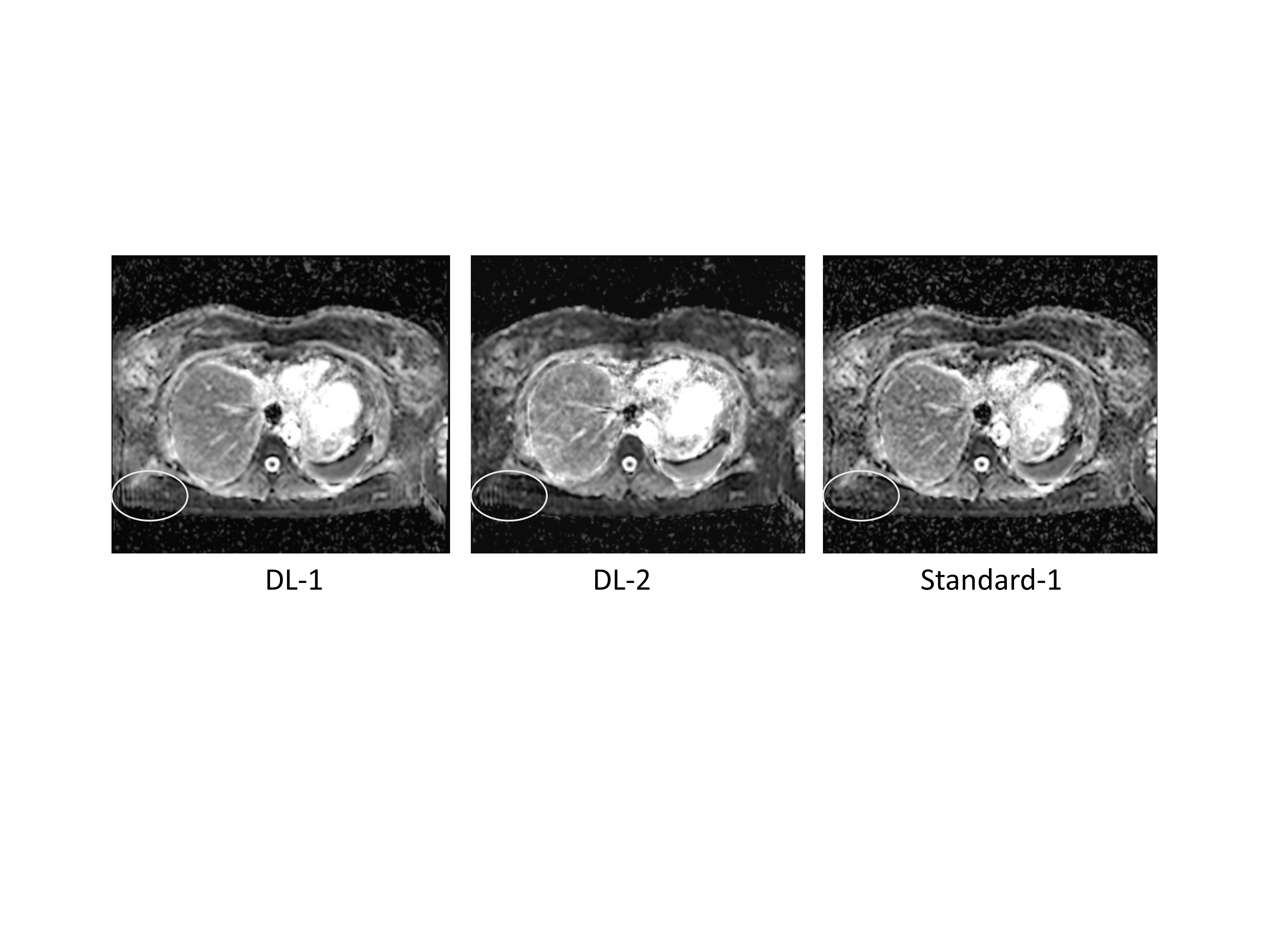
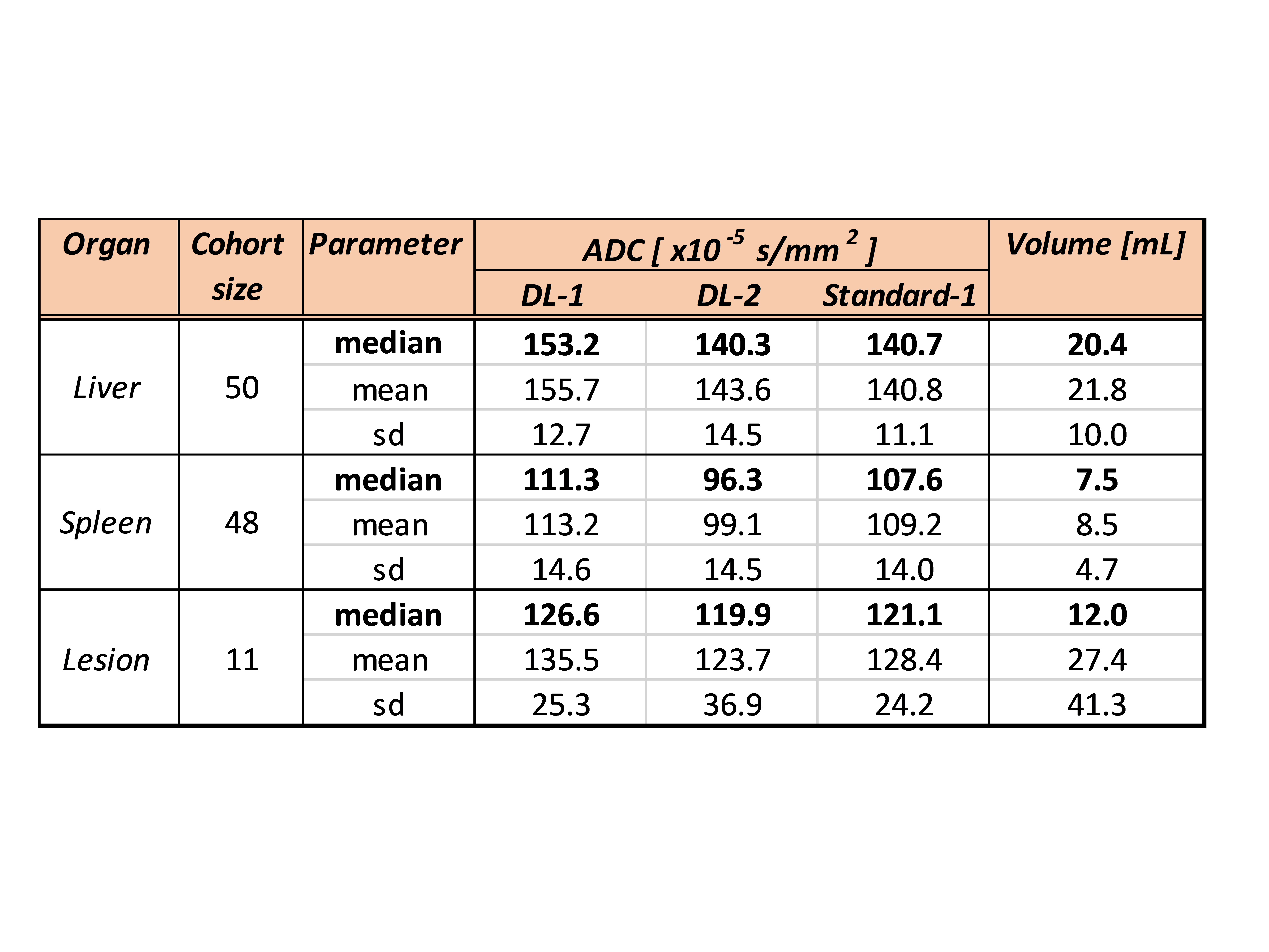
All 50 patients were successfully imaged and 11/50 patients had measurable hepatic lesions; 2 patients did not have spleen. One DL-related artefact (vertical striations in Fig.2) was observed on several random images for 38/50 patients for both DL series. The cohort median scores were good (3) or excellent (4) for all methods (Fig.3). Across both readers, DL-1 method scored best for 5/8 features on the b750 image (p<<0.05). All methods scored similarly on ADC maps. The faster sequence (DL-2) reduced the acquisition time from 2:59 to 1:43min but exhibited the lowest image quality. Quantitative ADC results are presented in Fig.4.Discussion
Measured ADCs were significantly different between DL-1 and standard reconstructed series across all three organs, with DL-1-based ADC being always higher (Fig.5). Although statistically significant, the relative difference of DL-1-based ADC compared with Standard-1 were <10% overall (8.9%, 3.4% and 4.5% for liver/spleen/metastases respectively) and may not be clinically relevant against the expected measurement repeatability of ADC. The heterogeneity of the liver ROIs might explain the higher discrepancy for the liver location. DL-2 series generated the lowest ADC, but also with a small relative difference (-10%).Conclusion
In this 50-patient cohort assessing liver DWI, a moderately-accelerated DL reconstruction method provided better image quality than a standard reconstruction. DL-derived ADC was slightly higher compared with ADC estimates from a standard reconstruction across liver/spleen/metastases.Acknowledgements
This study represents independent research funded by the National Institute for Health and Care Research (NIHR) Biomedical Research Centre at The Royal Marsden NHS Foundation Trust and The Institute of Cancer Research, London, and by the Royal Marsden Cancer Charity. The views expressed are those of the author(s) and not necessarily those of the NIHR or the Department of Health and Social Care.References
1. Parikh T, Drew SJ, Lee VS et al. Focal liver lesion detection and characterization with diffusion-weighted MR imaging: comparison with standard breath-hold T2-weighted imaging. Radiology. 2008;246:812-822.
2. Koh DM, Scurr E, Collins D et al. Predicting response of colorectal hepatic metastasis: value of pretreatment apparent diffusion coefficients. American Journal of Roentgenology. 2007;188:1001-1008.
3. Taouli B, Beer AJ, Chenevert T et al. Diffusion-weighted imaging outside the brain: Consensus statement from an ISMRM-sponsored workshop. J Magn Reson Imaging. 2016;44:521-540.
4. Bae SH, Hwang J, Hong SS et al. Clinical feasibility of accelerated diffusion weighted imaging of the abdomen with deep learning reconstruction: Comparison with conventional diffusion weighted imaging. Eur J Radiol. 2022;154:110428. doi: 10.1016/j.ejrad.2022.110428. Epub 2022 Jun 30. PMID: 35797791.
5. Hammernik K, Klatzer T, Kobler E et al. Learning a variational network for reconstruction of accelerated MRI data. Magn Reson Med 2018;79(6):3055-3071.
Figures