2572
Clinical assessment of whole-body MIPs as a survey tool in soft tissue disease with noise-corrected exponentially weighted DWI (niceDWI).1The Institute of Cancer Research, London, United Kingdom, 2The Royal Marsden NHS Foundation Trust, London, United Kingdom
Synopsis
Keywords: Diffusion Analysis & Visualization, Whole Body, Validation, Melanoma
Motivation: Maximum intensity projections (MIPs) generated from niceDWI could be beneficial as a survey tool in patients with soft-tissue disease, helping to save time in clinical reporting.
Goal(s): Perform a systematic clinical comparison of MIPs generated using niceDWI with MIPs generated using clinical DWI (clinDWI).
Approach: An experienced reader of whole-body MRI scored niceDWI and clinDWI MIPs in 20 patients with metastatic melanoma for SNR, CNR, artifacts, overall quality, and presence of disease in soft-tissues. ROC curves were plotted to assess disease detection.
Results: Image quality metrics were significantly worse in niceDWI, however there was no difference in ROC analysis of disease detection.
Impact: Whole-body MIPs using niceDWI did not improve disease detection in patients with soft-tissue disease, despite improved interstation homogeneity. Motion of soft-tissue lesions may limit SNR of niceDWI thus it may have higher clinical impact in surveillance of bone disease.
Introduction
Noise-corrected exponentially-weighted diffusion-weighted imaging (niceDWI) has been shown to improve interstation homogeneity in maximum intensity projections (MIPs) in whole-body DWI (WB-DWI) [1]. MIPs generated from niceDWI have been suggested as a survey tool for reference as part of clinical reporting, despite axial niceDWI not showing an improvement over clinical DWI (clinDWI) [2]. The aim of this study was to conduct a systematic clinical assessment of signal-to-noise ratio (SNR), contrast-to-noise ratio (CNR), presence of artifacts, and lesion detection in MIPs generated using niceDWI compared with MIPs generated using clinDWI in patients with metastatic melanoma (MM) with predominantly soft-tissue disease.Methods
20 patients with unresectable stage III or IV MM had WB-DWI prior to immunotherapy. Images were acquired at 1.5T (MAGNETOM Aera, Siemens Healthcare, Erlangen, Germany), with b-values 50, 600, and 900s/mm², with multi-directional diffusion-weighted gradients and 12 diffusion-encoding directions per b-value. The examination consisted of seven stations, covering from skull vertex to knees. A total of 75 lesions were identified in various tissues including: nodes (number of patients, n=10), lung (n=10), liver (n=7), brain (n=5), peritoneum (n=3), and bone (n=3)[2].clinDWI was generated by geometrically averaging the 12 acquisitions at b=900 s/mm² and niceDWI was calculated using
$$S(\mathrm{a}, b)=\exp \left(-\mathrm{a} \cdot \sigma_{\mathrm{ADC}}\right) \exp (-b\cdot \mathrm{ADC})$$
with a=2x104, b=900 s/mm², and iterative-weighted linear least-squares was used to estimate the ADC and ADC uncertainty ($$$\sigma_{\mathrm{ADC}}$$$) using DWI data at all b-values[1]. MIPs were generated from axial imaging rotating in the axial plane at 2° increments.
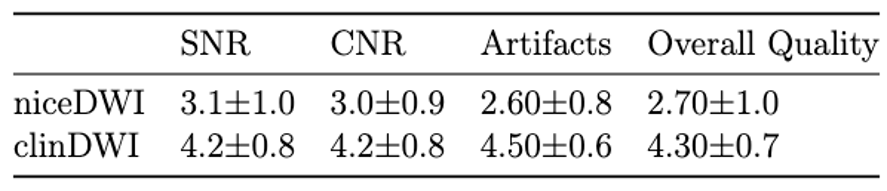
The MIPs generated with both niceDWI and clinDWI for each patient were randomised between two image reads separated by one week. A single reader, with 5 years’ experience in WB-MRI, scored the images for SNR, CNR, presence of artifacts, and overall image quality on a 1 to 5 scale (1=undiagnostic, 2=poor, 3=average, 4=good, 5=excellent). Wilcoxon signed-rank tests were conducted to assess significant differences between the two methods, with p<0.05 indicating significance.
Presence of nodal disease, disease in the liver, lungs, brain, peritoneum, and bone was also scored on a 5-point scale (presence of disease was: 1=highly unlikely, 2=unlikely, 3=not sure, 4=likely, 5=highly likely). Receiver-operator characteristic (ROC) curves were derived for both combined and individual disease locations, and the area under the curve (AUC) was calculated with confidence intervals estimated using the 5th/95th percentile of values from 1000 bootstrap samples with replacement. Ground truth was derived from the radiologist’s report including all clinical imaging (including CT where available).
Results
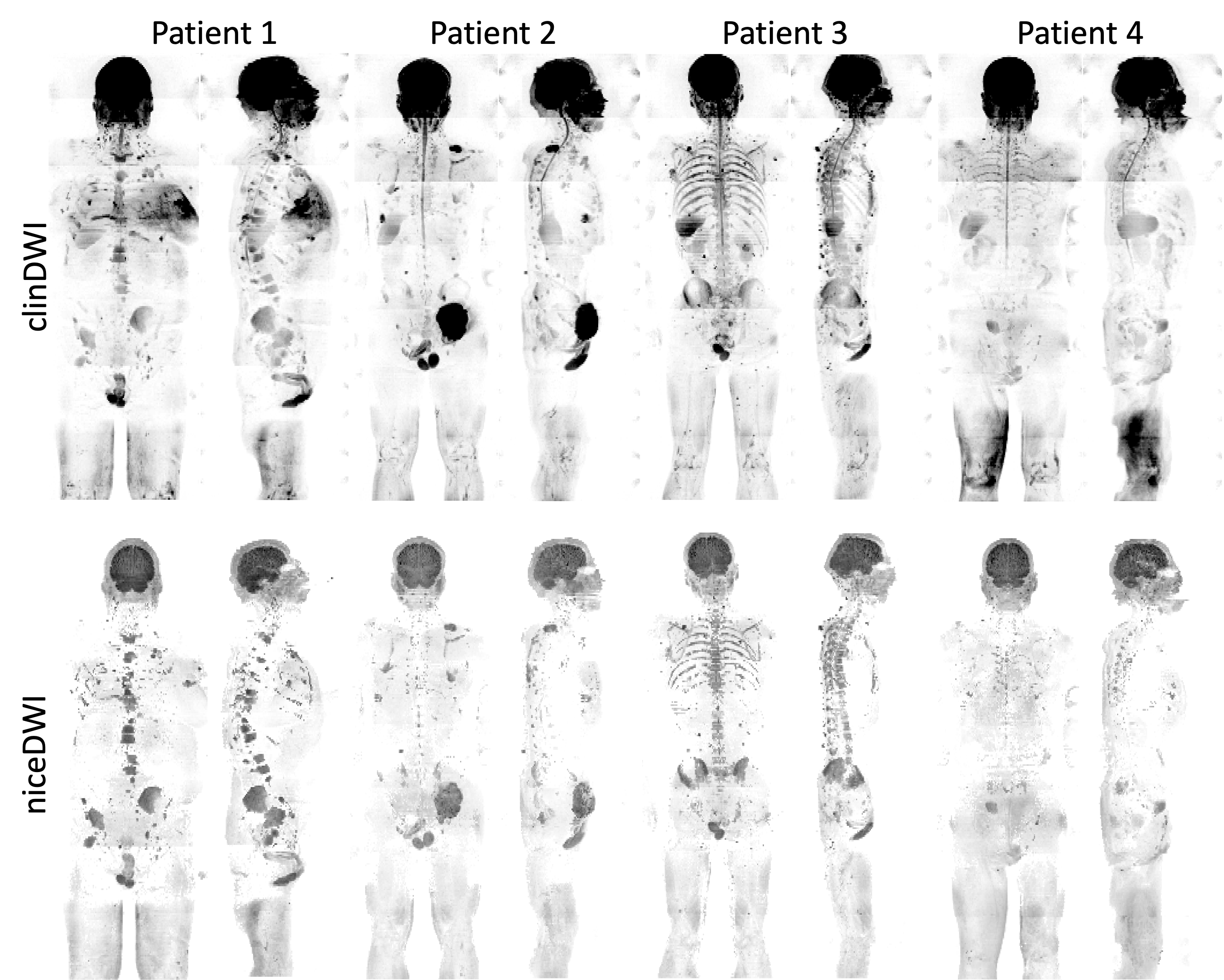
Examples of MIPs generated using clinDWI and niceDWI are shown in 4 patients with disease in a range of soft tissues (Figure 1).Clinician scores of SNR, CNR, presence of artifacts and overall image quality were significantly worse in niceDWI MIPs compared with clinDWI MIPs, Table 1 with all p-values<0.05.
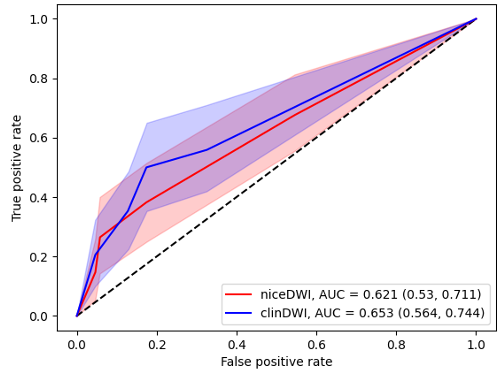
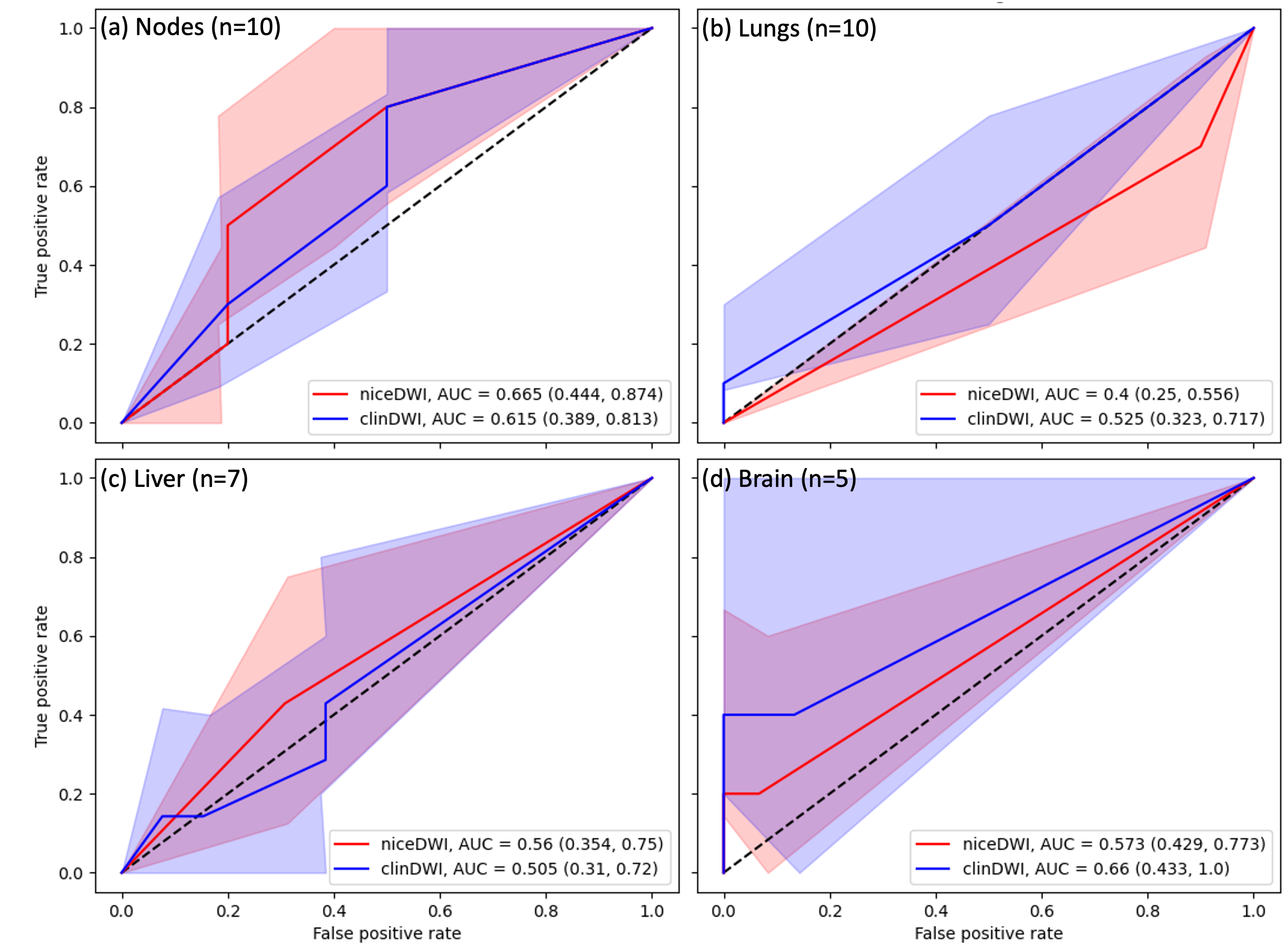
ROC curves are presented in Figure 2 for all tissues combined, excluding lung lesions due to known poor performance of DWI in this organ, and in Figure 3 for individual tissues where 5 or more patients showed evidence of disease (nodes, liver, lungs, brain). Diagnostic accuracy for individual lesions was not assessed. Marginal evidence was observed for all regions combined, though still small (AUC < 0.7).
Discussion
MIPs generated with niceDWI were clinically assessed to have significantly poorer image quality compared to clinDWI. One explanation for this may be high ADC uncertainty in soft-tissue regions due to organ motion, leading to low SNR.There was no significant difference in AUCs calculated using either technique, though diagnostic accuracy of both cases was poor indicating that review of the source axial DWI images is essential for clinical diagnosis of soft-tissue disease. This is especially true in the liver and lungs where the AUCs are around 0.5.
Although these results show that niceDWI MIPs demonstrate no advantage over clinDWI MIPs for disease detection in soft-tissues, assessment in bone disease may still be worthwhile. A systematic comparison in bone lesions using this data was not feasible as only 3 patients with bone metastases have been included in this analysis. Future work should also explore results incorporating more expert readers as image quality metrics are subjective.
Conclusion
A systematic comparison of MIPs generated using clinDWI with niceDWI showed no advantage to using niceDWI MIPs as a survey tool in patients with predominantly soft-tissue disease, despite improved inter-station homogeneity. Future analysis should evaluate clinical applications in bone disease.Acknowledgements
This study represents independent research funded by the National Institute for Health and Care Research (NIHR) Biomedical Research Centre at The Royal Marsden NHS Foundation Trust and The Institute of Cancer Research, London, and by the Royal Marsden Cancer Charity. The views expressed are those of the author(s) and not necessarily those of the NIHR or the Department of Health and Social Care.References
1. Blackledge MD, Tunariu N, Zugni F, et al (2020) Noise-Corrected, Exponentially Weighted, Diffusion-Weighted MRI (niceDWI) Improves Image Signal Uniformity in Whole-Body Imaging of Metastatic Prostate Cancer. Front Oncol 10:704.
2. Knill A, Blackledge M, Winfield J, et al (2023) Clinical assessment of noise corrected exponentially weighted diffusion weighted MRI (niceDWI) for imaging patients with metastatic melanoma. In: Proc Int Soc Magnet Reson Med. p 1496
Figures