2571
Degree of endometrial fibrosis evaluated using diffusion weighted imaging: initial findings1Department of Radiology, Drum Tower Hospital, Nanjing University Medical School, Nanjing, China, 2Department of Obstetrics and Gynecology, Drum Tower Hospital, Nanjing University Medical School, Nanjing, China
Synopsis
Keywords: DWI/DTI/DKI, Uterus, Endometrial fibrosis; Noninvasive evaluation
Motivation: Patients with endometrial fibrosis suffer from uterine infertility. Evaluating the degree of fibrotic endometrium can help clinicians to select the optimal treatment scheme.
Goal(s): To investigate the value of DWI in distinguishing the degree of endometrial fibrosis.
Approach: Mean intensity and standard deviation of endometrial ADC value in region of interest (ROI) (ADCROI and ADC-SDROI) and volume of interest (VOI) (ADCVOI and ADC-SDVOI) were measured and analyzed between healthy women, mild to moderate endometrial fibrosis (MMEF) patients and severe endometrial fibrosis (SEF) patients.
Results: Endometrial MRI parameters were significantly correlated to the degree of endometrial fibrosis, which can well differentiate each group.
Impact: This prospective study demonstrated the feasibility of DWI for quantitatively evaluating the degree of endometrial fibrosis, which can help clinicians to select the optimal treatment scheme and to perform dynamic follow-ups of therapy effect for patients with endometrial fibrosis.
Introduction
Endometrial fibrosis is mainly caused by endometrial injury such as curettage [1]. Patients with endometrial fibrosis always suffer from uterine infertility or recurrent abortion, which reduces the health of these patients [2]. Accurate evaluation of the degree of fibrotic endometrium can help clinicians to select the optimal treatment scheme. Diffusion-weighted imaging (DWI) can quantify the random diffusion of water molecules, which has been successfully applied to differentiate the severity of fibrosis in several organs [3, 4]. Thus, the aim of this prospective study was to investigate the value of DWI in distinguishing the degree of endometrial fibrosis.Methods
This study included 41 healthy women (median age, 27 years; interquartile range [IQR], 26-31 years), 30 patients with mild to moderate endometrial fibrosis (MMEF) (median age, 33 years; IQR, 29-36 years) and 102 patients with severe endometrial fibrosis (SEF) (median age, 33 years; IQR, 30-36 years) according to the American Fertility Society (AFS) scoring criteria [5]. MRI was conducted using a 3.0-T MRI scanner (Ingenia, Philips Medical Systems, Best, The Netherlands) with a body coil. Due to the dynamic changes of endometrium during the menstrual cycles [6], all participants underwent MRI scans during the periovulatory phase. MRI sequences include sagittal DWI and T2-weighted imaging of uterus. DWI was acquired using a single-shot echo planar imaging (EPI) turbo spin-echo (TSE) sequence with b value of 0 s/mm2 and 1000 s/mm2. ADC maps were automatically generated with the inbuilt scan software. T2-weighted imaging was acquired using a TSE sequence. MRI images was independently analyzed by two radiologists. Endometrial ADC values were measured on ADC maps using ITK-SNAP software (www.itksnap.org) [7]. The radiologists manually drew endometrial region of interest (ROI) on midsagittal ADC map to obtain the mean intensity (ADCROI) and standard deviation (ADC-SDROI) of endometrial ADC value. Endometrial volume of interest (VOI) was manually delineated slice by slice on sagittal ADC map to obtain the mean intensity (ADCVOI) and standard deviation (ADC-SDVOI) of endometrial ADC value. The ROIs and VOIs were delineated to include the whole endometrium zones of corpus uteri and exclude visible cyst areas. Final endometrial MRI parameters were defined as the mean value of the two measurements (with an interval of 2 months) by the first radiologist. The measurement of endometrial MRI parameters by the second radiologist was used to assess the inter-observer reproducibility. Shapiro-Wilk test was used to analyze normal distribution. Differences of MRI parameters between each group were analyzed by Kruskal-Wallis test with Bonferroni adjustment. Spearman’s correlation coefficient (rho) was used to test the correlation between MRI parameters and the degree of endometrial fibrosis. A multivariable model was built using a binary logistic regression analysis combing endometrial ADCROI, ADC-SDROI, ADCVOI and ADC-SDVOI. Receiver operating characteristic (ROC) curve was generated to analyze the ability of MRI parameters in differentiating the degree of endometrial fibrosis. Reproducibility of MRI parameters was tested by intraclass correlation coefficient (ICC).Results
Endometrial ADCVOI and ADCROI of healthy women were significantly higher than those of MMEF patients and SEF patients. Endometrial ADC-SDVOI and ADC-SDROI of SEF patients were significantly higher than those of healthy women and MMEF patients. Endometrial ADCVOI and ADCROI were significantly negatively correlated to the degree of endometrial fibrosis (rho = -0.526 and -0.349, both P < 0.001), while endometrial ADC-SDVOI and ADC-SDROI were significantly positively correlated to the degree of endometrial fibrosis (rho = 0.729 and 0.713, both P < 0.001). Excellent performance was found for multivariable model in discriminating MMEF from normal endometrium, endometrial ADCVOI, for ADC-SDVOI, ADC-SDROI and multivariable model in distinguishing SEF from normal endometrium, and for ADC-SDVOI, ADC-SDROI and multivariable model in differentiating SEF from MMEF (all AUCs >0.800). MRI parameters, except for ADC-SDROI in MMEF patients, showed good or excellent intra- and inter-observer’s reproducibility.Discussion
A main change of fibrotic endometrium is an accumulation of collagen fibrils [2], which can reduce the random diffusion of water molecules and cause a decreased endometrial ADC value. Endometrial ADCVOI and ADCROI were negatively correlated to the degree of endometrial fibrosis. This indicates that an increased degree of endometrial fibrosis presents more accumulation of collagen fibrils in endometrium. endometrial ADC-SDVOI and ADC-SDROI were positively correlated to the degree of endometrial fibrosis. This suggests the higher degree of endometrial fibrosis, the more heterogeneity of endometrial parenchyma.Conclusion
This prospective study demonstrated the feasibility of DWI for quantitatively evaluating the degree of endometrial fibrosis, which can help clinicians to select the optimal treatment scheme and to perform dynamic follow-ups of therapy effect.Acknowledgements
No acknowledgement found.References
1. Zhou Z, Wang H, Zhang X, et al. Defective autophagy contributes to endometrial epithelial-mesenchymal transition in intrauterine adhesions. Autophagy. 2022;18(10):2427-2442.
2. Huang J, Zhang W, Yu J, et al. Human amniotic mesenchymal stem cells combined with PPCNg facilitate injured endometrial regeneration. Stem Cell Res Ther. 2022;13(1):17.
3. Sheng R, Zhang Y, Sun W, et al. Staging Chronic Hepatitis B Related Liver Fibrosis with a Fractional Order Calculus Diffusion Model. Acad Radiol. 2022;29(7):951-963.
4. Mao W, Ding X, Ding Y, et al. Evaluation of interstitial fibrosis in chronic kidney disease by multiparametric functional MRI and histopathologic analysis. Eur Radiol. 2023;33(6):4138-4147.
5. The American Fertility Society classifications of adnexal adhesions, distal tubal occlusion, tubal occlusion secondary to tubal ligation, tubal pregnancies, mullerian anomalies and intrauterine adhesions. Fertil Steril. 1988;49(6):944-955.
6. Chen L, Song T, Peng X, et al. Magnetic resonance imaging thicknesses and apparent diffusion coefficient values of the endometrium and junction zone in women of reproductive age. Acta Radiol. 2023;64(3):1263-1271.
7. Yushkevich PA, Piven J, Hazlett HC, et al. User-guided 3D active contour segmentation of anatomical structures: significantly improved efficiency and reliability. Neuroimage. 2006;31(3):1116-1128.
Figures
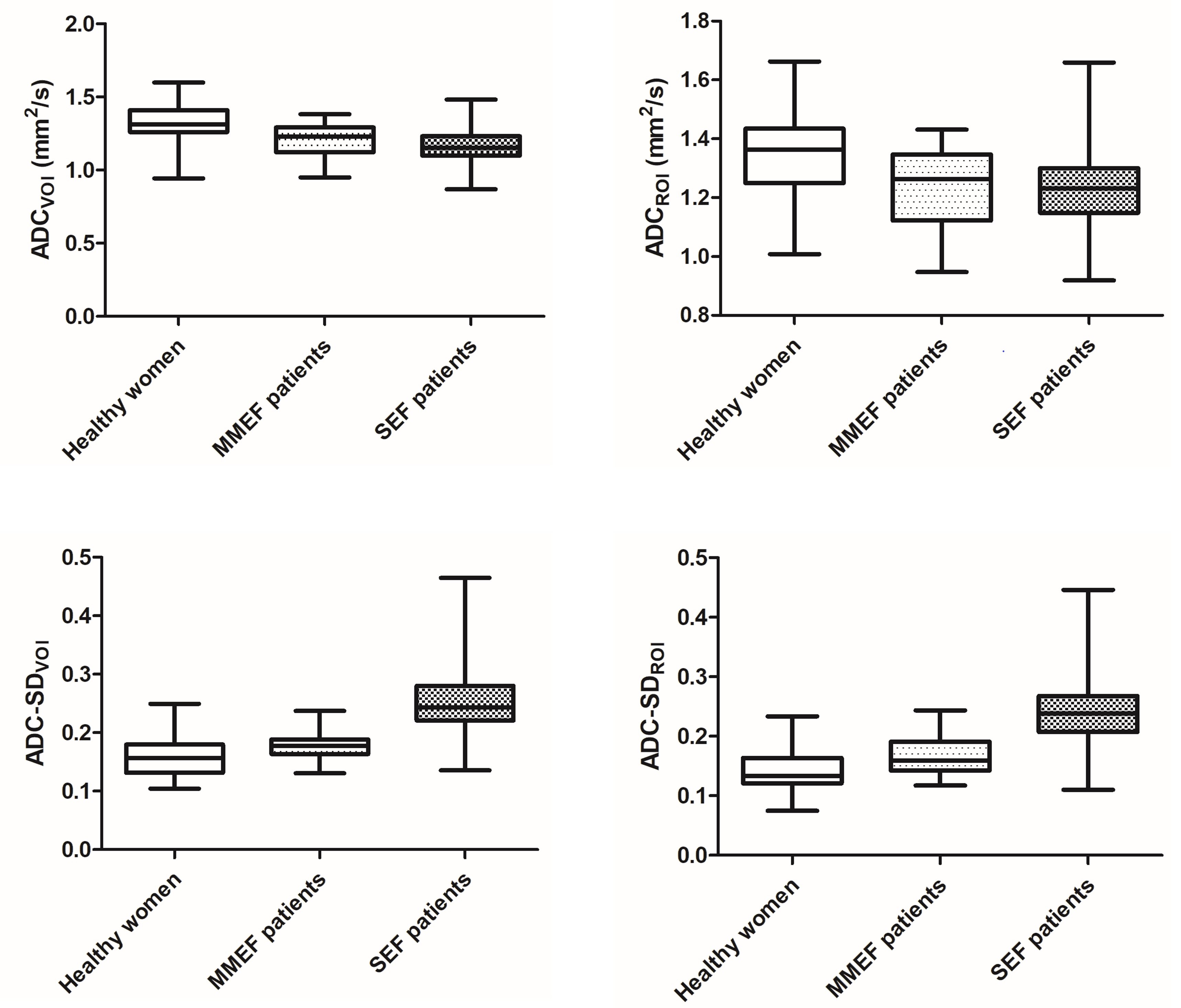
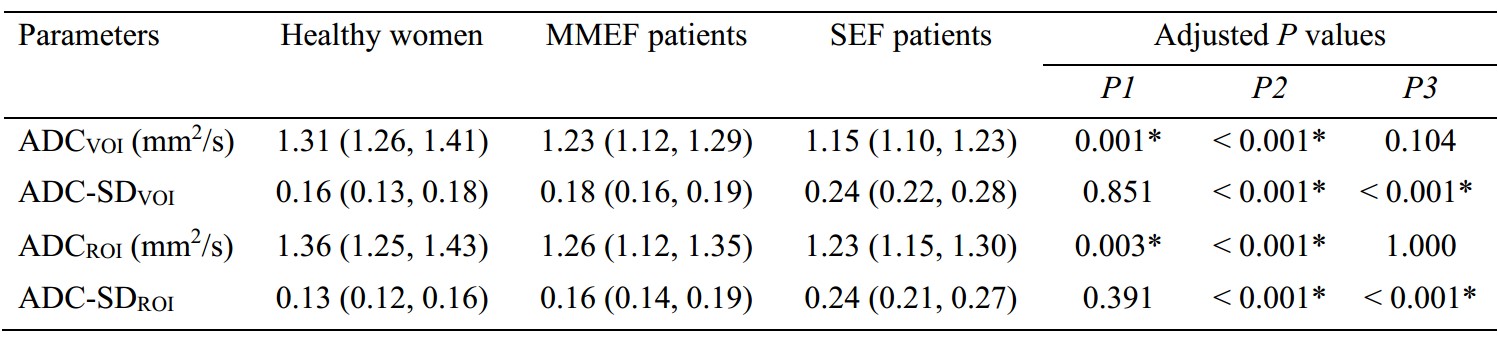
Table 1: Differences of endometrial MRI parameters between each group
Note: MMEF, mild to moderate endometrial fibrosis; SEF, severe endometrial fibrosis; ADCVOI and ADC-SDVOI, the mean intensity and standard deviation of endometrial ADC value in volume of interest; ADCROI and ADC-SDROI, the mean intensity and standard deviation of endometrial ADC value in region of interest. P1, P2, and P3 represented healthy women compared with MMEF patients, healthy women compared with SEF patients, and MMEF patients compared with SEF patients, respectively.
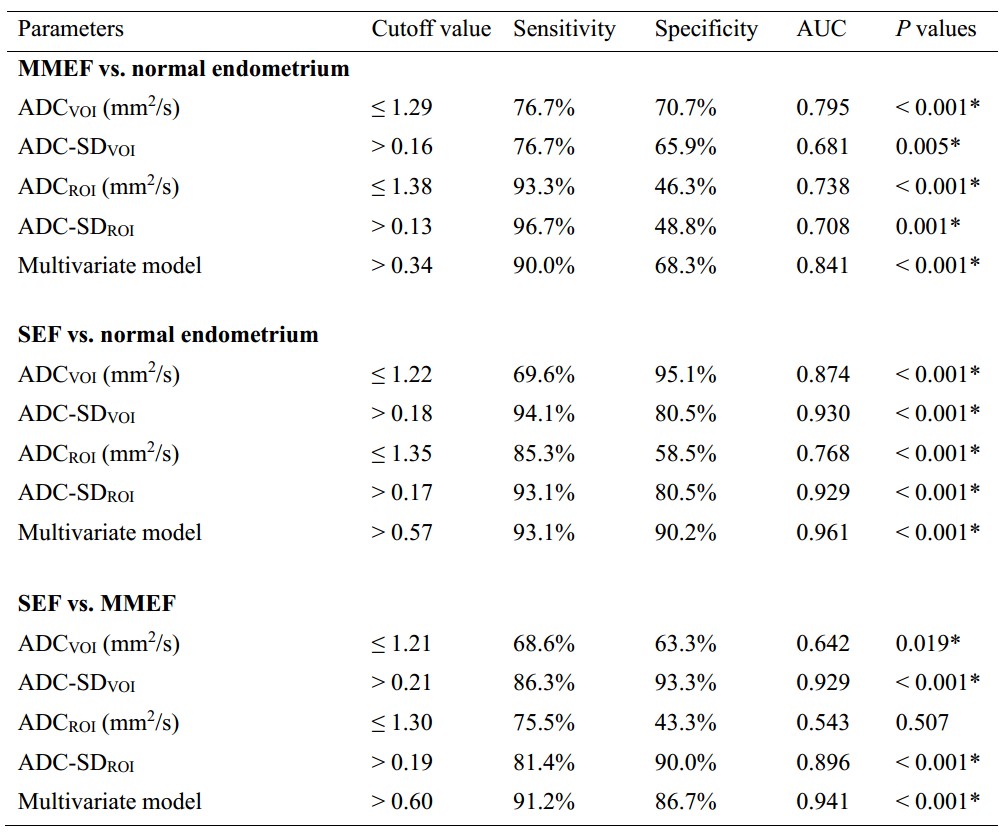
Table 2: Performance of endometrial MRI parameters in diagnosing endometrial fibrosis
Note: MMEF, mild to moderate endometrial fibrosis; SEF, severe endometrial fibrosis; ADCVOI and ADC-SDVOI, the mean intensity and standard deviation of endometrial ADC value in volume of interest; ADCROI and ADC-SDROI, the mean intensity and standard deviation of endometrial ADC value in region of interest.
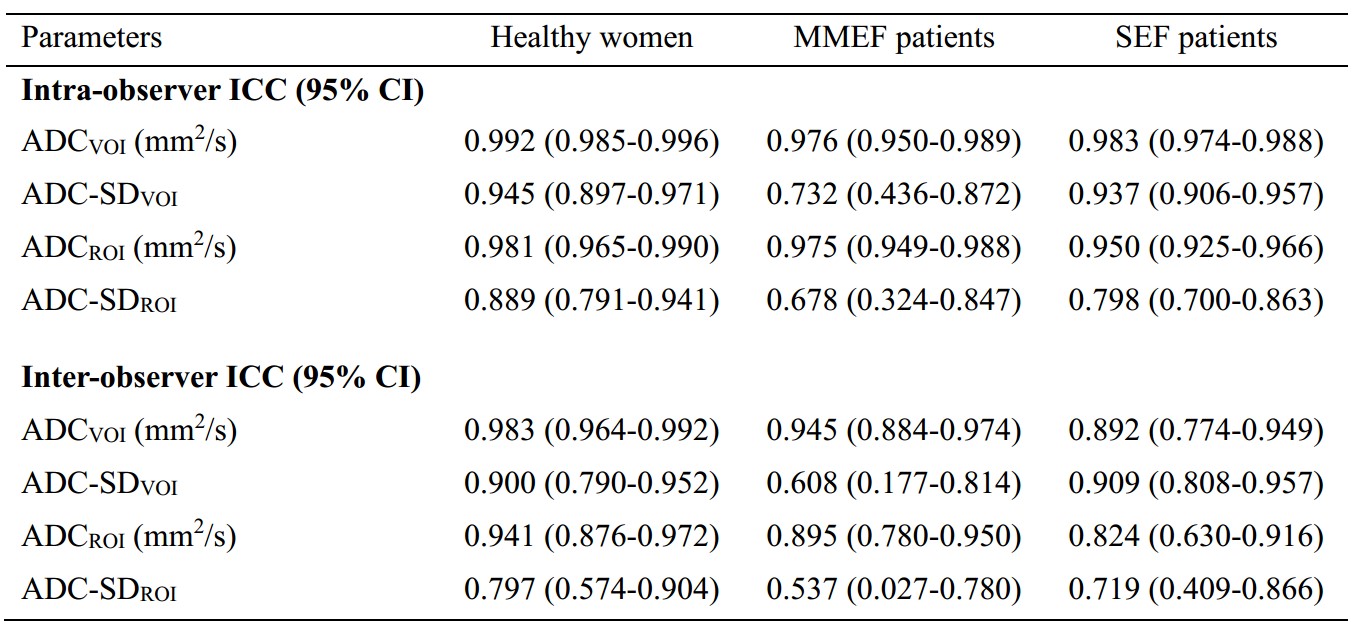
Table 3: Reproducibility of endometrial MRI Parameters in each group
Note: MMEF, mild to moderate endometrial fibrosis; SEF, severe endometrial fibrosis; ICC, intraclass correlation coefficient; CI, confidence interval; ADCVOI and ADC-SDVOI, the mean intensity and standard deviation of endometrial ADC value in volume of interest; ADCROI and ADC-SDROI, the mean intensity and standard deviation of endometrial ADC value in region of interest.