2570
Time-Dependent Diffusion MRI for Quantitative Microstructural Mapping of Intestinal Fibrosis in Patient with Crohn’s disease1The First Affiliated Hospital, Sun Yat-Sen University, Guangzhou, China, 2MR Research Collaboration, Siemens Healthineers, Beijing, China
Synopsis
Keywords: DWI/DTI/DKI, Microstructure
Motivation: Microstructural characteristics of intestinal fibrosis is a crucial determinant impacting the selection of therapeutic strategies and prognosis of patients with Crohn’s disease (CD).
Goal(s): To evaluate the feasibility and efficacy of time-dependent diffusion MRI (TD-dMRI) based microstructural mapping for noninvasive characterization of intestinal fibrosis in intestinal strictures in CD.
Approach: TD-dMRI was performed in consecutive CD patients scheduled for surgery. TD-dMRI-based microstructural parameters acquired were compared with conventional apparent diffusion coefficient (ADC) and verified by histopathogical measures.
Results: Multiparametric TD-dMRI-based microstructural mapping correlates with pathological findings and demonstrates promise for characterizing intestinal fibrosis in CD.
Impact: Time-dependent diffusion MRI-based microstructural mapping demonstrates promise for noninvasively characterizing intestinal fibrosis of CD, with high accuracy against histopathologic standard, thus guiding treatment and predicting clinical outcome.
Methods: This prospective observational study enrolled 13 CD patients with 45 resected intestinal strictures between May 2023 and October 2023, who underwent TD-dMRI and were scheduled for surgery within 4 weeks. TD-dMRI were acquired by using a combination of pulsed and oscillating gradient spin-echo sequences (Siemens research sequence) at an equivalent diffusion time of 4.2-12.0 msec on a 3T MR scanner (MAGNETOM Prisma, Siemens Healthcare, Erlangen, Germany). TD-dMRI-based microstructural parameters, including cell diameter, extracellular diffusivity, intracellular volume fraction, cellularity, and diffusivities with different effective diffusion time, were estimated using a two-compartment (limited spectrally edited diffusion, IMPULSED) model of the least square curve fitting toolbox in MATLAB (MathWorks, Inc.). Conventional ADC was also calculated for comparison with these parameters. Region-by-region correlations with the surgical specimens were performed to determine the histologic degree of fibrosis. The accuracy of these microstructural imaging parameters was confirmed through their correlations with histopathologic measurements. One-way analysis of variance test, Spearman rank correlation, and receiver operating characteristic curve were used for statistical analysis.
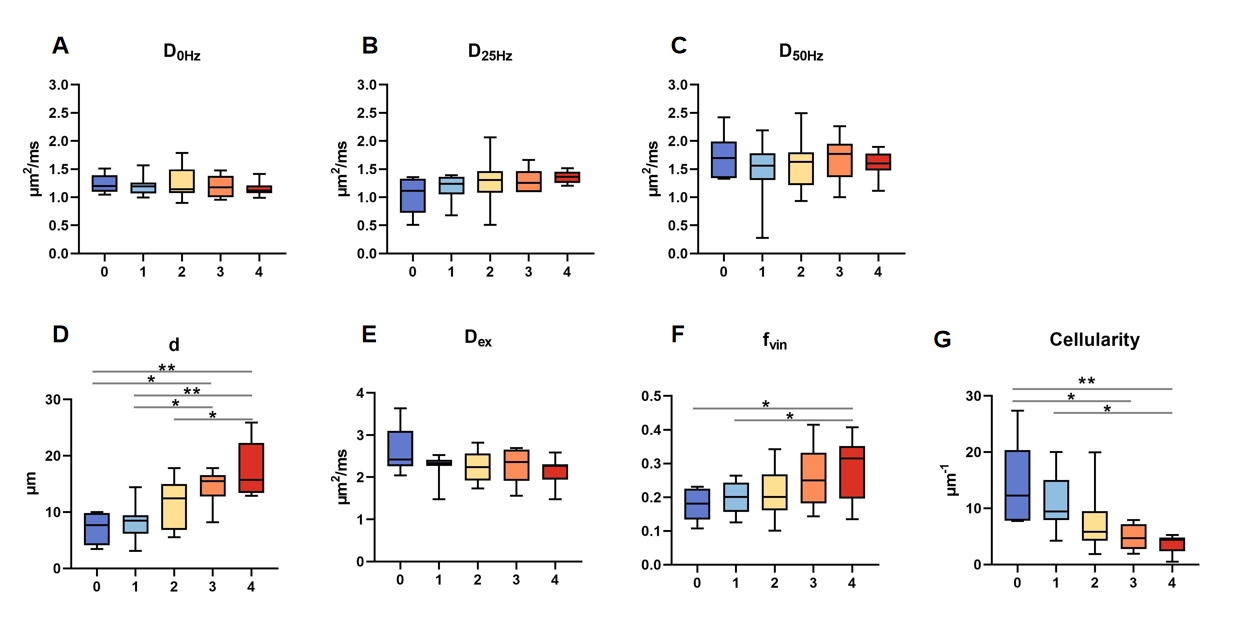
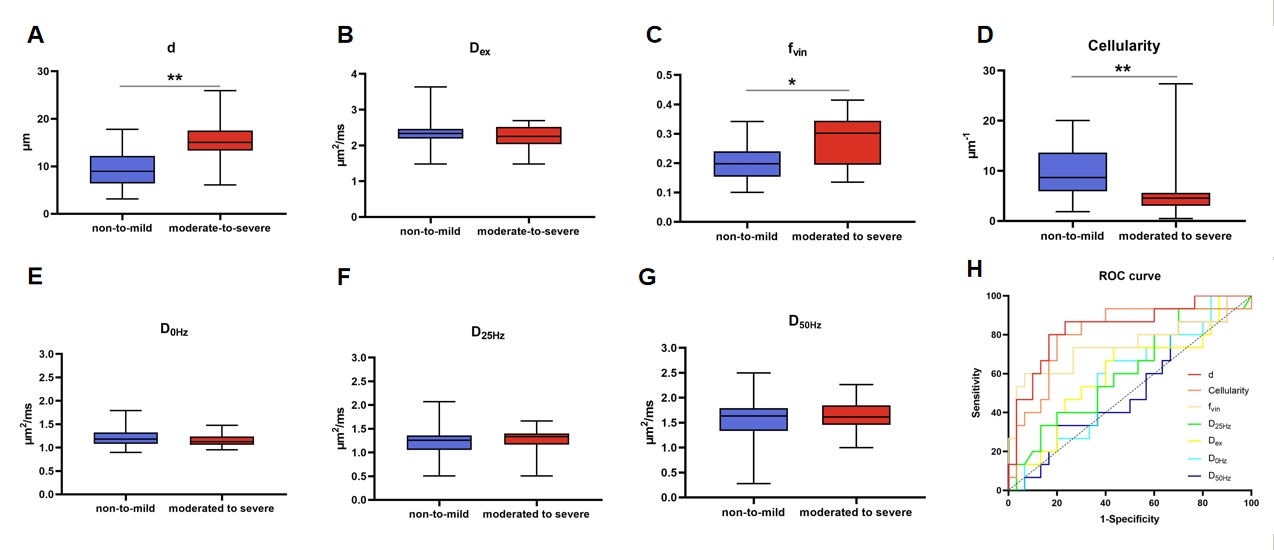
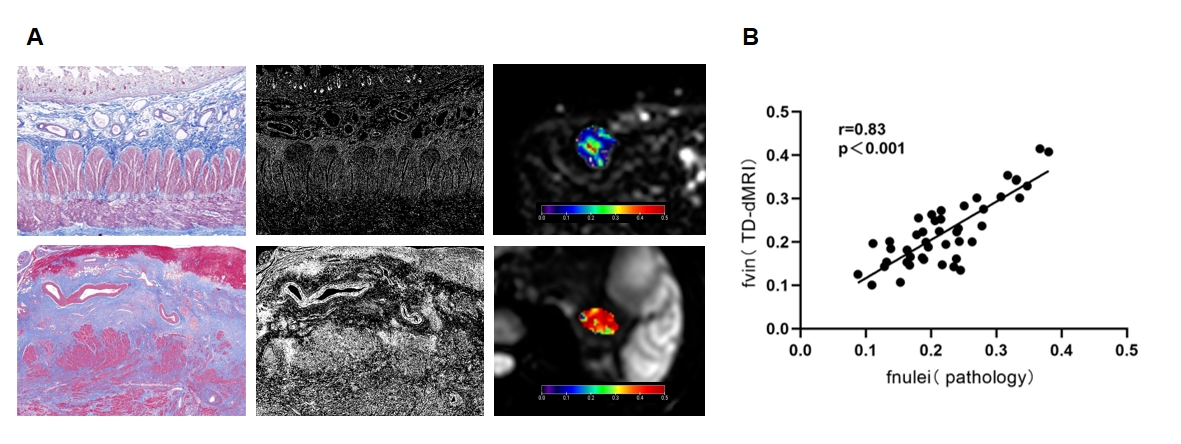
Results: According to TD-dMRI measurements, there were significant correlations of higher cell diameter (mean cell diameter=6.47, 8.03, 11.30, 14.56, and 17.31 μm for fibrosis scores 0-4, respectively; r=0.53; p<0.001), increased intracellular volume fraction (mean intracellular volume fraction=0.17, 0.19, 0.21, 0.25, and 0.29 for fibrosis scores 0-4, respectively; r=0.34; p<0.01), and decreased cellularity (mean cellularity=16.15, 11.04, 7.79, 4.87, and 3.66, respectively; r=0.55; p<0.01) with elevated pathological fibrosis scores. Among all measurements derived from TD-dMRI, cell diameter achieved the highest diagnostic performance with an area under the receiver operating characteristic curve (AUC) of 0.87 (p<0.001) in discriminating moderate-to-severe fibrosis from non-to-mild fibrosis, followed by cellularity (AUC=0.82, p=0.001), intracellular volume fraction (AUC=0.75, p<0.01), diffusivity at oscillating frequencies of 25 Hz (AUC=0.62, p=0.21), extracellular diffusivity (AUC=0.61, p=0.24), diffusivity at oscillating frequencies of 50Hz (AUC=0.51, p=0.93) and ADC (AUC=0.45, p=0.50). Microstructural mapping was supported by positive correlations between TD-dMRI-based and pathologic examination-based intracellular volume fraction (r=0.83, p<0.001).
Conclusion: TD-dMRI allows for the characterization of microstructural features of intestinal strictures in CD patients, especially those related to fibrosis. Cell diameter shows great potential as a promising biomarker for noninvasive detection of varying degrees of bowel fibrosis.
Acknowledgements
No acknowledgement found.References
1. Rieder F, Zimmermann EM, Remzi FH, Sandborn WJ. Crohn's disease complicated by strictures: a systematic review. Gut 2013;62(7):1072-1084. doi: 10.1136/gutjnl-2012-3043532.
2. Latella G, Di Gregorio J, Flati V, Rieder F, Lawrance IC. Mechanisms of initiation and progression of intestinal fibrosis in IBD. Scand J Gastroenterol 2015;50(1):53-65. doi: 10.3109/00365521.2014.9688633.
3. Caruso A, Angriman I, Scarpa M, D'Incà R, Mescoli C, Rudatis M, Sturniolo GC, Schifano G, Lacognata C. Diffusion-weighted magnetic resonance for assessing fibrosis in Crohn's disease. Abdom Radiol (NY) 2020;45(8):2327-2335. doi: 10.1007/s00261-019-02167-05.
4. Tielbeek JA, Ziech ML, Li Z, Lavini C, Bipat S, Bemelman WA, Roelofs JJ, Ponsioen CY, Vos FM, Stoker J. Evaluation of conventional, dynamic contrast enhanced and diffusion weighted MRI for quantitative Crohn's disease assessment with histopathology of surgical specimens. Eur Radiol 2014;24(3):619-629. doi: 10.1007/s00330-013-3015-76.
5. Gore JC, Xu J, Colvin DC, Yankeelov TE, Parsons EC, Does MD. Characterization of tissue structure at varying length scales using temporal diffusion spectroscopy. NMR Biomed 2010;23(7):745-756. doi: 10.1002/nbm.15317.
6. Wu D, Jiang K, Li H, Zhang Z, Ba R, Zhang Y, Hsu YC, Sun Y, Zhang YD. Time-Dependent Diffusion MRI for Quantitative Microstructural Mapping of Prostate Cancer. Radiology 2022;303(3):578-587. doi: 10.1148/radiol.211180
Figures