2568
Enhancing Diagnostic Precision in Clear Cell Renal Cell Carcinoma: A Comparative Analysis of ADC and CTRW Models1Department of Radiology, Sun Yat-Sen Memorial Hospital, Sun Yat-sen University, Guangzhou, China, 2MR Research Collaboration, Siemens Healthineers, Guangzhou, China, 3MRI clinical application customer service department, Siemens digital medical technology co.LTD, Shanghai, China
Synopsis
Keywords: Diffusion Modeling, Diffusion/other diffusion imaging techniques
Motivation: The unexplored potential of applying the continuous-time random walk (CTRW) model for clear cell renal cell carcinoma (ccRCC) grading, possibly surpassing the effectiveness of apparent diffusion coefficient (ADC).
Goal(s): To compare ADC and CTRW in diagnosing ccRCC grades via MRI.
Approach: This study involved 52 ccRCC patients and employed in-house software for CTRW and ADC maps. Statistical analysis employed Mann-Whitney U tests and ROC curves.
Results: DCTRW outperformed ADC in grading ccRCC, effectively distinguishing between low- and high-grade cases, while αCTRW and βCTRW did not.
Impact: This research has the potential to shape clinical practices, offering more accurate ccRCC diagnoses, leading to better treatment decisions, and driving advancements in renal cell carcinoma research.
Introduction
Clear cell renal cell carcinoma (ccRCC) is the predominant form of kidney cancer in adults, constituting approximately 70% of cases1. Variations in ccRCC grades lead to diverse biological behaviors and clinical outcomes2. Magnetic resonance imaging (MRI) is effective for preoperative assessment of ccRCC 3, with diffusion-weighted imaging (DWI) revealing tissue density changes and aiding in characterizing ccRCC and infiltration zones 4-12. Apparent diffusion coefficient (ADC) values offer a non-invasive approach to predicting RCC nuclear grading and histological subtypes.However, as medical imaging evolves, there is a growing demand for more precise diagnostic methods. ADC, based on water diffusion, lacks information on water diffusion in complex sub-cellular microstructures14,15. Given the intricate microstructures within ccRCC tumors16, advanced mathematical models, like the continuous-time random walk (CTRW) model using high b-values DWI, have the potential to offer more accurate water diffusion information and microstructure mapping17,18.
Although the CTRW model has shown promise in prior studies18,19, its application to ccRCC remains unexplored. Our research aims to investigate and compare the diagnostic capabilities of ADC and the CTRW model in the context of ccRCC grading.
Materials and Methods
PatientsFrom October 2021 to July 2023, 52 patients were included. They were categorized into low-grade (Fuhrman 1/2; 31 patients) and high-grade (Fuhrman 3/4; 21 patients) groups based on hematoxylin-eosin (HE) staining. A uropathologist with a decade of experience confirmed pathology results. For cases with inconsistent grades due to tumor heterogeneity, Fuhrman nuclear grading used the highest segment determined by microscopy.
Image Data Acquisition
All these patients performed A free-breath single shot echo-planar-imaging (ss-EPI) sequence scanning on a 3T MR scanner (VIDA, Siemens, Germany) using an eight-channel array body coil. The DWI acquisition parameters are as follows in the table 1.
The parametric maps of CTRW (extract anomalous diffusion coefficient, DCTRW, and temporal and spatial heterogeneity parameters, αCTRW and βCTRW) and mono-exponential model (ADC) were calculated using a unified in-house developed software called BoDiLab, which is based on Python 3.7. The corresponding mathematical expressions are shown as follows:
1) Monoexponential model:
S(b) = S0·exp. (−b·ADC)
where S0 and Sb are signal intensities at b-value = 0 s/mm2 and other b-values, respectively, and b is a diffusion sensitization factor that decides the degree of diffusion weighting in the signal intensity.
2) The CTRW model:
S/S0 = Eα(-(bD)β)
where D (mm2/s1) is an anomalous diffusion coefficient, the parameters α and β (dimensionless) are temporal and spatial fractional orders that are related to temporal and spatial diffusion heterogeneities, respectively, and Eα is a Mittag-Leffler function.
Two experienced radiologists blinded to the study independently and manually delineated the tumors’ volume of interest (VOI) along the boundary of the whole tumor on each slice of DW images (b-value = 1000 s/mm2) using 3D Slicer (version 5.0.2).
Statistical analyses were performed using SPSS (version22.0) and MedCalc software (version 15.8.0). Mann-Whitney U tests compared parameters for high and low-grade ccRCC patients. ROC curve analysis assessed diagnostic performance and established optimal cutoff values for malignancy prediction, with p < 0.05 signifying statistical significance.
Results
The study successfully obtained ADC and CTRW maps (DCTRW, αCTRW, and βCTRW) from 52 ccRCC patients (median age 53; range 29-73). These patients were classified into low grade (Fuhrman 1/2, 31 patients) and high grade (Fuhrman 3/4, 21 patients) groups. Figures 1 and 2 depict the ADC and CTRW parametric MR images of high- and low-grade ccRCC patients. High-grade ccRCC exhibited significantly lower ADC and DCTRW values compared to low-grade ccRCC (p < 0.05). In contrast, αCTRW and βCTRW showed no significant differences between the two groups (p > 0.05). Figure 3 displays ROC curves for different diffusion model distinguishing high-grade from low-grade ccRCC. DCTRW's AUC was 0.891, surpassing ADC's AUC of 0.790, suggesting its superiority in grading ccRCC.Discussion and Conclusion
In this study, both ADC and DCTRW effectively distinguished high- from low-grade ccRCC tumors with significantly lower values in high-grade cases, signifying increased cell density and decreased extracellular space, supporting their use as biomarkers. While αCTRW and βCTRW did not demonstrate significant differences between high- and low-grade ccRCC, DCTRW outperformed ADC in AUC, highlighting its advantage in capturing water diffusion in tumor microstructures, leading to a potentially more precise and sensitive tool for grading and characterizing ccRCC. Our results support previous findings of CTRW performance in evaluating brain tumors18.In summary, our study demonstrated that diffusion-related parameters (ADC, DCTRW) can be used to accurately differentiate low- and high-grade ccRCC. Moreover, CTRW may be more suitable for the grading of ccRCC compared to ADC.
Acknowledgements
No acknowledgement found.References
1. BR L, MW K. Predicting outcomes in renal cell carcinoma. Curr Opin Urol 2005; 15:289–297.
2. JC C, CM L, H Z, et al. Comparisons of outcome and prognostic features among histologic subtypes of renal cell carcinoma. Am J Surg Pathol 2003; 27:612–624.
3. M Y, KJ F, S S, et al. Quantitative multiparametric MR analysis of small renal lesions: correlation with surgical pathology. Abdom Radiology (New York) 2018; 43:3390–3399.
4. AB R, BE N, EF F, et al. Utility of the apparent diffusion coefficient for dis- tinguishing clear cell renal cell carcinoma of low and high nuclear grade. AJR Am J Roentgenol 2010; 195:W344–W351.
5. A G, R S, AS B, et al. Diffusion-weighted MRI in renal cell carcinoma: a surrogate marker for predicting nuclear grade and histological subtype. Acta Radiol 2012; 53:349–358.
6. Wang H, Cheng LX, et al. Renal cell carcinoma: diffusion-weighted MR imaging for subtype differentiation at 3.0 T. Radiology 2010; 36: 135–143.
7. J Z, YM T, L W, et al. Renal masses: characterization with diffusion- weighted MR imaging—a preliminary experience. Radiology 2008; 247:458–464.
8. X Y, M L, H O, et al. Application of ADC measurement in characterization of renal cell carcinomas with different pathological types and grades by 3.0T diffusion-weighted MRI. Eur J Radiol 2012; 81:3061–3066.
9. JL Z, EE S, H C, et al. Variability of renal apparent diffusion coefficients: limitations of the monoexponential model for diffusion quantification. Radiology 2010; 254:783–792.
10. K S, CP S, R R, et al. Usefulness of diffusion-weighted imaging in the evaluation of renal masses. AJR Am J Roentgenol 2010; 194:438–445.
11. AA R, A F, A M, et al. Role of diffusion-weighted magnetic resonance imaging in characterization of renal tumors. J Comput Assist Tomogr 2011; 35:332–336.
12. S S, G H-P, L P, et al. Utility and limitations of 3-Tesla diffusion-weighted magnetic resonance imaging for differentiation of renal tumors. Eur J Radiol 2014; 83:909–913.
13. Y L, Z Y, H S, et al. Grading of uterine cervical cancer by using the ADC difference value and its correlation with microvascular density and vas- cular endothelial growth factor. Eur Radiol 2013; 23:757–765.
14. LB D. Molecular diffusion nuclear magnetic resonance imaging. Magn Reson Q (1991) 7(1):1–30.
15. LB D. Apparent diffusion coefficient and beyond: what diffusion Mr imaging can tell us about tissue structure. Radiology (2013) 268(2):318–22.
16. J Y, DK Y, GS M, et al. Non-Gaussian analysis of diffusion weighted imaging in head and neck at 3T: a pilot study in patients with nasopha- ryngeal carcinoma. PLoS One 2014; 9:e87024.
17. I C, M RL, CP L, et al. On random walks and entropy in diffusion-weighted magnetic resonance imaging studies of neural tissue. Magn Reson Med (2014) 71(2):617–27.
18. K MM, Si Y, W H, et al. Differentiating low- and high-grade pediatric brain tumors using a continuous-time random-walk diffusion model at high b-values. Magn Reson Med (2016) 76(4):1149–57.
19. C H, W D, L Y, et al. Evaluation of breast cancer malignancy, prognostic factors and molecular subtypes using a continuous-time random-walk MR diffusion model. Eur J Radiol. 2023 Sep;166:111003.
Figures
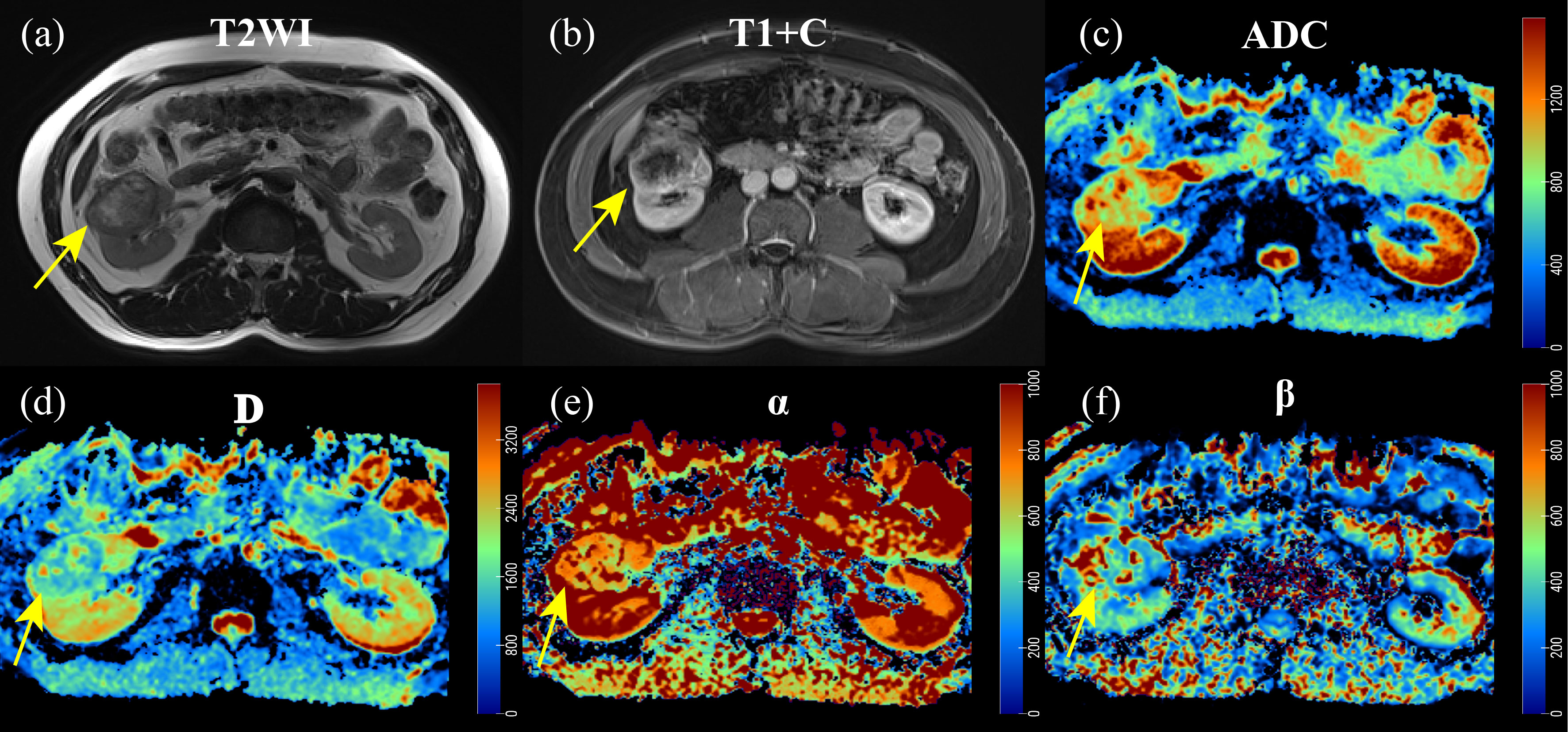
Figure 1 A 54-year-old man with pathologically confirmed ccRCC (high grade) in the right kidney. a: T2-weighted image; b: post-contrast T1W image (excretory phase); c: ADC map; d-f: D, α and β maps of CTRW
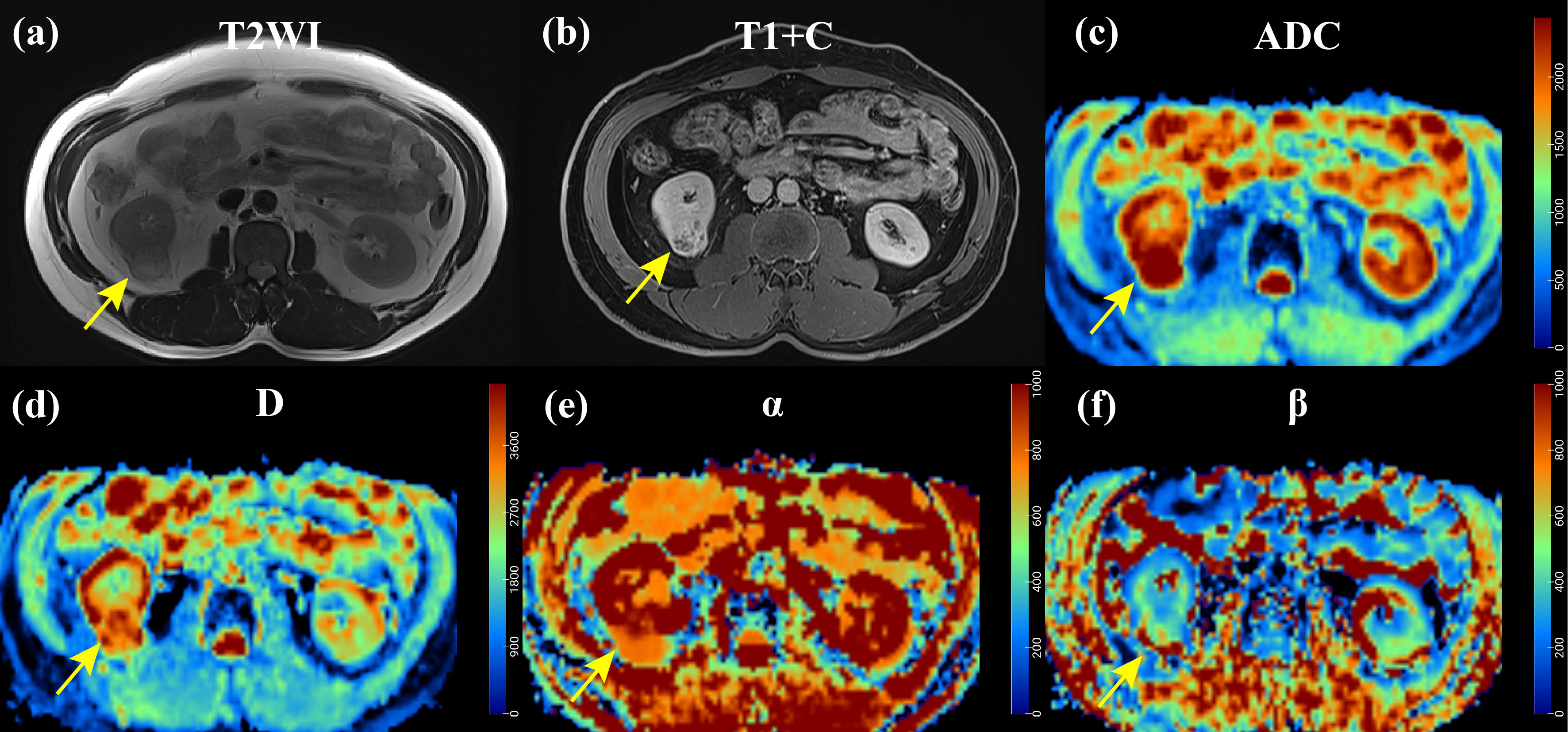
Figure 2 A 44-year-old man with pathologically confirmed ccRCC (low grade) in the right kidney. a: T2-weighted image; b: post-contrast T1W image (excretory phase); c: ADC map; d-f: D, α and β maps of CTRW
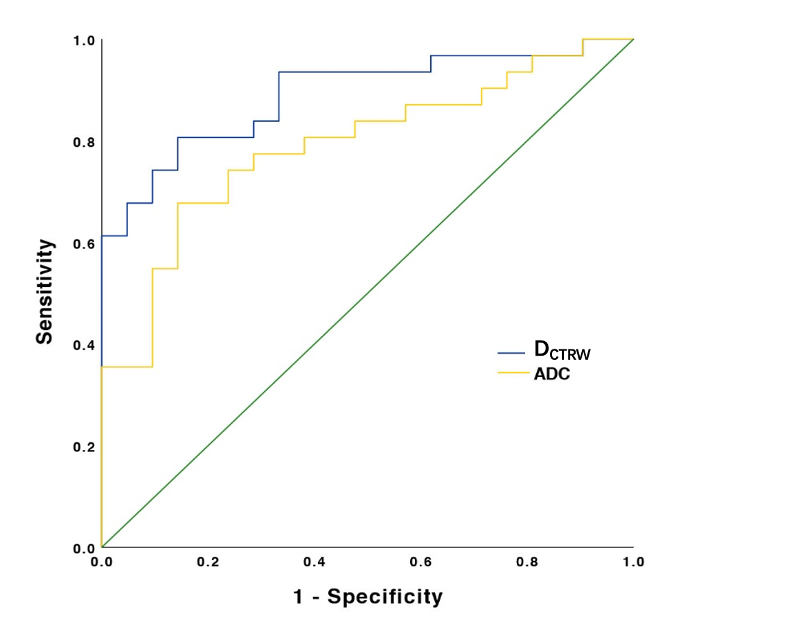
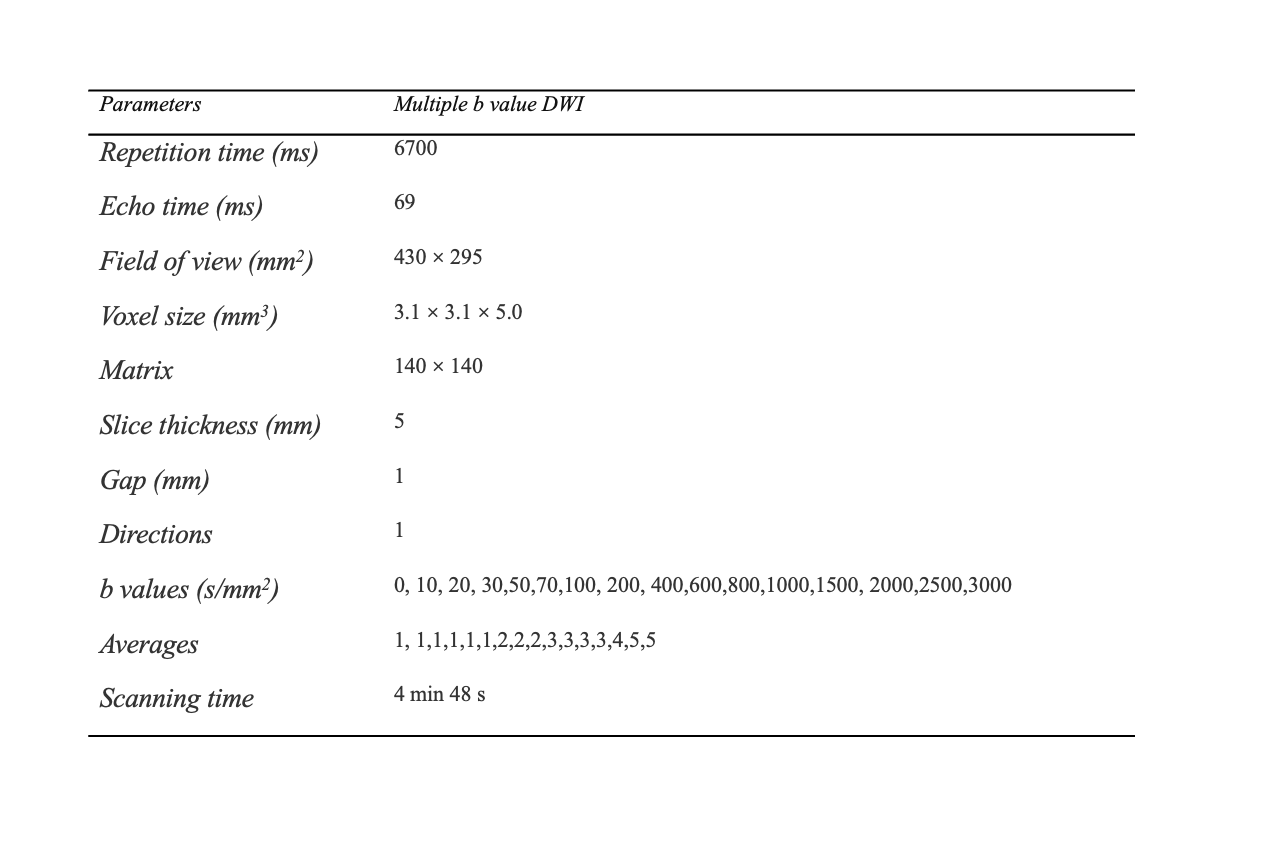
Table 1 MR parameters of Multiple b value DWI sequence