2567
Using the MRI-ADC and clinicopathological feature nomogram to Predict microsatellite instability status in colorectal carcinomas1Gansu University of Chinese Medicine, Lanzhou, China, 2Gansu Provincial People's Hospital, Lanzhou, China, 3Philips Healthcare, Xi’an, China
Synopsis
Keywords: Diffusion Acquisition, Digestive, ADC, clinicopathological, microsatellite instability, colorectal neoplasm
Motivation: Given that microsatellite instability (MSI) detection often involves invasive pathological biopsies, it is of paramount importance to find a non-invasive, individualized detection technology for accurately and effectively predicting the MSI status of colorectal cancer (CRC) patients prior to surgery. This approach could mitigate the limitations associated with biopsies and enhance the treatment of CRC patients.
Goal(s): To investigate the value of MRI-ADC mean values and clinicopathological features in predicting MSI in colorectal cancer.
Approach: The ADC model and ADC-clinicopathologic nomogram model were established by using MRI-ADC parameters and clinicopathological features.
Results: The combined ADC-clinicopathological nomogram model was the best predictor of CRC MSI.
Impact: Pathological testing for MSI status is often invasive and comes with a higher risk of complications. In contrast, the ADC-clinical combined nomogram model provides a noninvasive, comprehensive tool for preoperative prediction of CRC MSI and for guiding clinical treatment decisions.
Introduction
The production of MSI can induce hypermutant phenotypes of tumors. At present, the detection of CRC MSI mainly relies on pathological specimen PCR and immunohistochemistry (IHC). However, invasive colonoscopy tissue specimen acquisition may lead to the risk of intestinal perfusion and perforation, and improper or insufficient tissue sampling due to the temporal and spatial heterogeneity of MSI in tumor tissues [1]. Therefore, it is important to use a non-invasive and individualized MSI detection technique to predict MSI status in CRC patients before surgery. In recent years, researchers have shown great potential in predicting CRC MSI status by using T2WI and ADC combined model, T2WI combined clinical model, and MRI multi-parameter imaging radiomics model [2-4]. However, as far as we know, there are no studies on ADC-clinicopathological features combined models to predict the status of CRC MSI. Therefore, this study used ADC values and clinicopathological features to establish a combined ADC-clinicopathological model to predict CRC MSI.Materials and methods
The clinicopathologic data of 144 patients with CRC confirmed by pathology in Gansu Provincial People's Hospital from July 2022 to August 2023 were retrospectively collected. All patients were scanned by 3.0T MRI scanner (Elition, Philips Healthcare, the Netherlands), with 16-channel torso coil. ADC maps were generated from DWI (b=0 and 1000s/mm2) sequence. The 144 patients were divided into two groups according to IHC results: patients with high MSI status (MSI-H) and patients with low MSI status (MSI-L) were classified into MSI group, and patients with stable MSI status (MSS) were classified into MSS group. The ADC values of the same ADC images were measured by two radiologists who had worked for more than 5 years experiences with abdominal diagnosis and without knowing any clinical information of the patients The averaged ADC values were used for analysis. Intraclass correlated coefficient (ICC) was used to determine the agreement of ADC measurement between two radiologists. SPSS (version 26) software was used to compare the clinical baseline data of patients, and P < 0.05 was considered statistically significant. Independent predictors were included to form a nomogram of ADC-clinicopathological combination. Receiver operating characteristic curve (ROC) was used to evaluate the predictive power of ADC model and ADC-clinicopathological model. The area under the curve (AUC) was calculated and compared by DeLong test. Calibration curves were used to evaluate the goodness of fit of the model, and decision analysis curves (DAC) and clinical impact curves (CIC) were used to evaluate the clinical utility of the model.Results
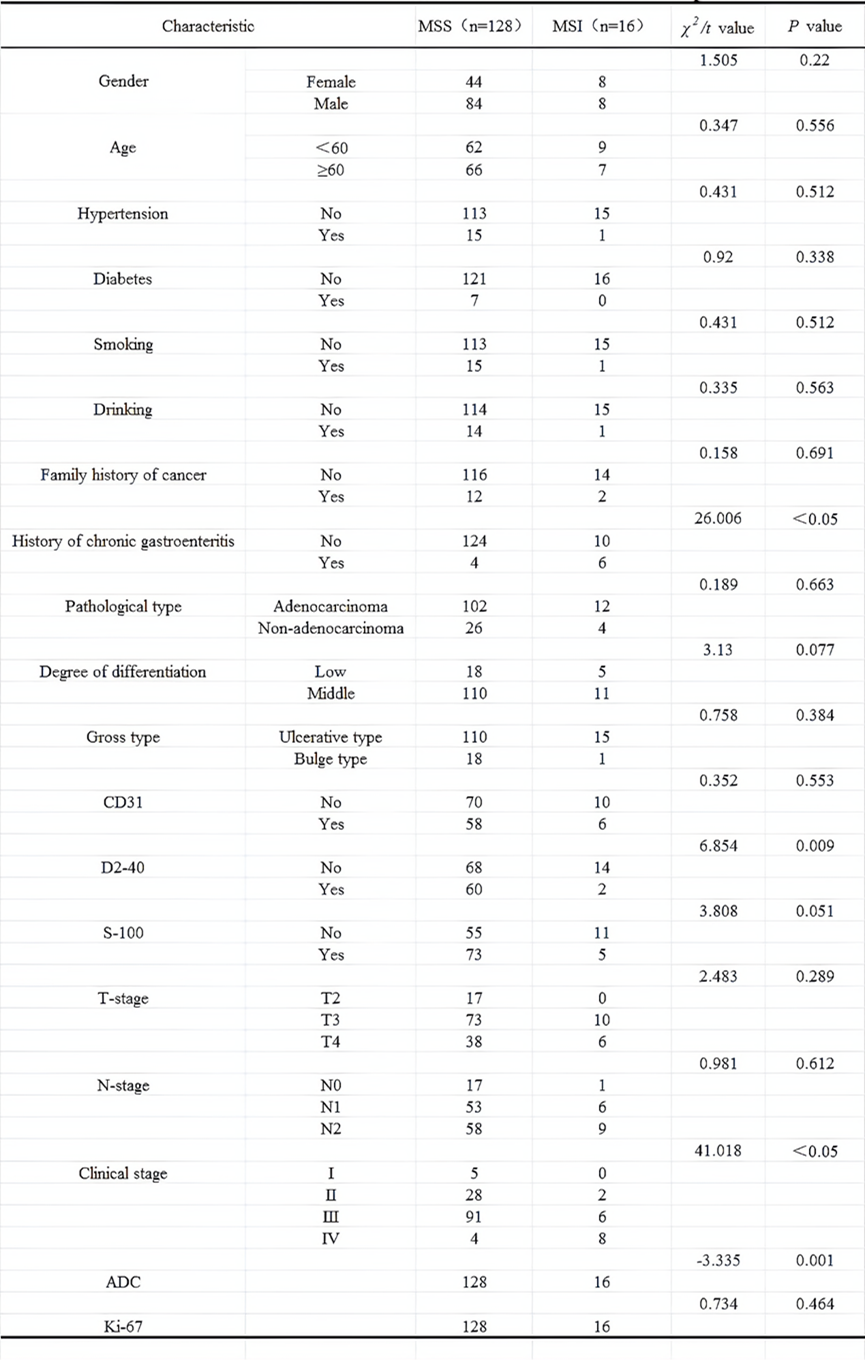
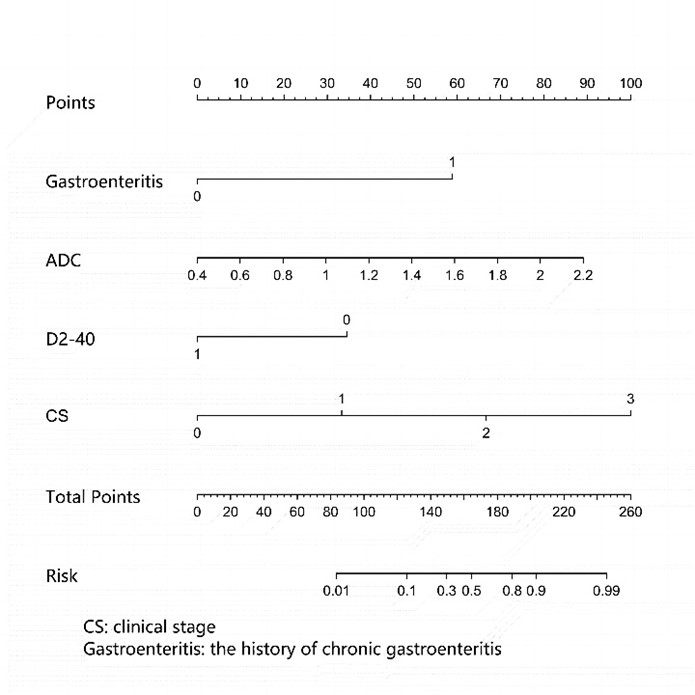
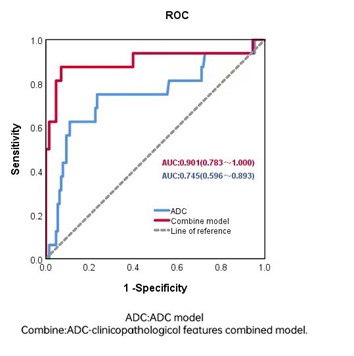
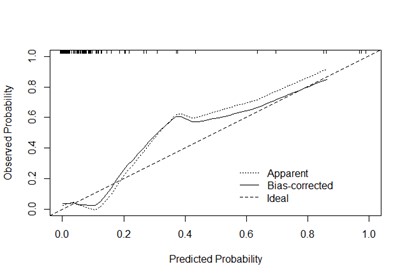
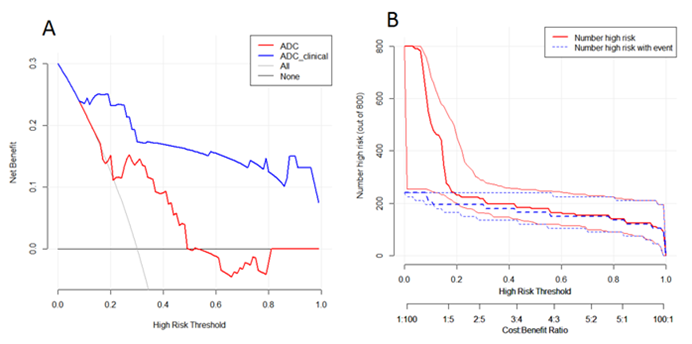
Table1 showed the demographic characteristics of the patients. There was good agreement (ICC = 0.85) between the two radiologists. ADC values in the MSI group (1.107±0.335) were higher than those in the MSS group (0.868±0.262). Among the collected clinicopathological features, the history of chronic gastroenteritis (P < 0.001), D2-40 (P=0.009), clinical stage (P < 0.001), and ADC value (P=0.001) showed statistically significant differences between MSI group and MSS group. The above four independent predictors were combined to form a nomogram (Figure 1). Among the ADC model and the ADC-clinicopathologic feature combined model, the ADC-clinicopathologic feature combined model predicted the best performance of CRC MSI, with an AUC of 0.745 (95%CI,0.596 ~ 0.893), sensitivity of 0.750, specificity of 0.766. The AUC of the combined ADC-clinicopathological model was 0.901 (95%CI,0.783 ~ 1.000), and the sensitivity and specificity were 0.875 and 0.930, respectively (Figure 2). The calibration curve has a good goodness of fit (Figure 3), the DAC and CIC have good clinical practical value (Figure 4).Discussion
MSI CRC patients have significantly higher survival and prognosis than MSS CRC patients and the probability of lymphatic metastasis and distant metastasis is also less[5]. D2-40 is an important marker of lymphatic vessel infiltration, and positive D2-40 indicates the higher the malignant degree of the tumor. Our study incorporated independent predictors of chronic intestinal history, D2-40, clinical stage, and ADC values into the nomogram to significantly improve the model's performance in predicting CRC MSI. Since the additional cost of PCR and IHC methods is not required, ADC combined with clinicopathological features can improve the cost-effectiveness ratio. Our results showed that the combined ADC value, D2-40 and clinical features of the nomogram model is more effective in predicting MSI status in colorectal cancer patients. It also shows the great potential of the joint model to predict the CRC MSI.Conclusion
This study showed that the ADC model and the ADC-clinicopathological features combined nomogram model had good predictive performance for CRC MSI, and the ADC-clinicopathological combined nomogram model had the best performance. This study can provide a personalized, non-invasive method for predicting CRC MSI.Acknowledgements
No acknowledgement found.References
[1] PEI Q, YI X, CHEN C, et al. Pre-treatment CT-based radiomics nomogram for predicting microsatellite instability status in colorectal cancer [J]. Eur Radiol, 2022, 32(1): 714-724.
[2] LI Z, DAI H, LIU Y, et al. Radiomics Analysis of Multi-Sequence MR Images For Predicting Microsatellite Instability Status Preoperatively in Rectal Cancer [J]. Front Oncol, 2021, 11: 697497.
[3] ZHANG W, YIN H, HUANG Z, et al. Development and validation of MRI-based deep learning models for prediction of microsatellite instability in rectal cancer [J]. Cancer Med, 2021, 10(12): 4164-4173.
[4] LEFEBVRE T L, UENO Y, DOHAN A, et al. Development and Validation of Multiparametric MRI–based Radiomics Models for Preoperative Risk Stratification of Endometrial Cancer [J]. Radiology, 2022, 305(2): 375-386.
[5] PETRELLI F, GHIDINI M, CABIDDU M, et al. Microsatellite Instability and Survival in Stage II Colorectal Cancer: A Systematic Review and Meta-analysis [J]. Anticancer Res, 2019, 39(12): 6431-6441.
Figures