2559
Altered Gyrification in Fetal Growth Restriction with Prenatal Magnetic Resonance Images1Sagol Brain Institute, Tel Aviv Sourasky Medical Center, Tel Aviv, Israel, 2Sagol School of Neuroscience, Tel Aviv University, Tel Aviv, Israel, 3Sackler Faculty of Medicine, Tel Aviv University, Tel Aviv, Israel, 4Department of Radiology, Tel Aviv Sourasky Medical Center, Tel Aviv, Israel, 5School of Computer Science and Engineering, The Hebrew University of Jerusalem, Israel, Jerusalem, Israel, 6Children's Hospital of Eastern Ontario (CHEO), Department of Medical Imaging, University of Ottawa, Ottawa, ON, Canada
Synopsis
Keywords: Prenatal, Fetus, gyrification, fetal growth restriction
Motivation: Fetal growth restriction (FGR) is highly associated with adverse outcomes. While reduced brain volume is associated with FGR, knowledge regarding cortical developmental is scarce.
Goal(s): We aimed to quantitatively assess differences in brain volumes and cortical folding patterns between FGR and appropriate-for gestational-age (AGA) fetuses, and between FGR with normal and abnormal pulsatile-index (PI) measured by Doppler-US in the middle-cerebral-artery (MCA).
Approach: Gyrification and brain volume were computed using an automatic method based on T2-weighted MRI.
Results: Significant reduction of brain volume and gyrification were detected in FGR compared with AGA, and in gyrification in fetuses with abnormal MCA-PI.
Impact: Reduced gyrification in FGR fetuses can offer insights into the pathomechanism linking abnormal MCA-PI, cortical development, and postnatal outcomes. This may enable marker for assessing the severity of restriction and facilitate pregnancy management by determining the optimal time for delivery.
Introduction
Fetal growth restriction (FGR) is defined as a failure of the fetus to achieve its growth expectation and is associated with worse short- and long-term outcomes1–3. Placental insufficiency is the principal cause of FGR, limiting the fetus’s nutritional and oxygen supplies. To adapt to hypoxemia and protect the brain, the fetus redistributes blood flow to the cerebral circuit for oxygen and nutrient supply to the brain, a process which is called brain sparing (BS)4. In such cases abnormal pulsatile-index (PI) is detected in the middle-cerebral-artery (MCA) measured by Doppler-US. However, this does not ensure a normal brain development trajectory, putting growth-restricted fetuses at risk for adverse neurodevelopmental outcomes5–9.Several studies demonstrated differences in brain development in FGR-complicated pregnancies. These include reduced supra- and infratentorial brain volumes10, deeper insular depth with cortical volume depletion and smaller operculum11–14, and shorter corpus callosum15–18. Although folding patterns are important milestones for normal development19 , data on FGR cortical folding are scarce.The aim of this study was to quantitatively explore the differences in cortical folding patterns between FGR and appropriate-for gestational-age (AGA) fetuses, and between FGR with normal and abnormal MCA-PI measured by Doppler-US, i.e. with and without BS.Methods
A total of 113 singleton fetuses were included: 78 AGA (mean 31.9±2.4 weeks, range 27-37 weeks) pregnancies retrospectively collected, and 35 FGR-pregnancies (mean 33.2±2.2 weeks, range 26.85-37 weeks) prospectively recruited. Inform consent was obtained for all woman in the prospective cohort, and a waiver was received for the retrospective cohort. FGR was defined according to the Delphi consensus20 as: (1) EFW or abdominal circumference <10th centile with any of the following: umbilical artery pulsatile index (PI) > 95th centile, uterine artery PI > 95th centile or cerebroplacental ratio <5th centile; or (2) EFW or abdominal circumference <3rd centile. FGR fetuses were further divided into brain-sparing positive (BS+, MCA-PI<5th centile, N=14) or negative (BS-, MCA-PI≥5th centile, N=21). Coronal T2-weighted fetal barin-MRI was acquired on two 3T scanners (GE/Siemens).Gyrification parameters: Fetal gyrification quantification was performed using an automatic methodology, similar to Yehuda et al.21, In brief the method consist of the following steps: (A) brain detection with an anisotropic 3D U-Net classifier22; (B) brain sub-segmentation using an existing method23. Subtle manual corrections as needed to ensure accurate cortex segmentation; (C) gyrification indices (GI) computation based on the hemisphere contour in each slice (GIC), as the ratio of the cerebral and convex hull contours lengths. Two parameters were used to quantify fetal gyrification: (1) mean GIC=the mean value from all slices; (2) max GIC=the maximum value from all slices, representing the Sylvian fissure level. Each parameter was calculated separately for the right and left hemispheres and averaged into a single score.
Brain component volumes: All anatomical boundaries were determined according to the brain sub-segmentation23, with three components: left hemisphere, right hemisphere, and cerebellum with brain-steam. Volume analysis was divided to the Supratentorial volume, defined as the left and right hemispheres, and to the combined Cerebellum & Brainstem volume.
Statistical analysis: Correlation between brain component volumes and gyrification parameters to GA was done using Spearman’s coefficient. Comparisons between groups were performed using ANOVA, with control for GA.
Results
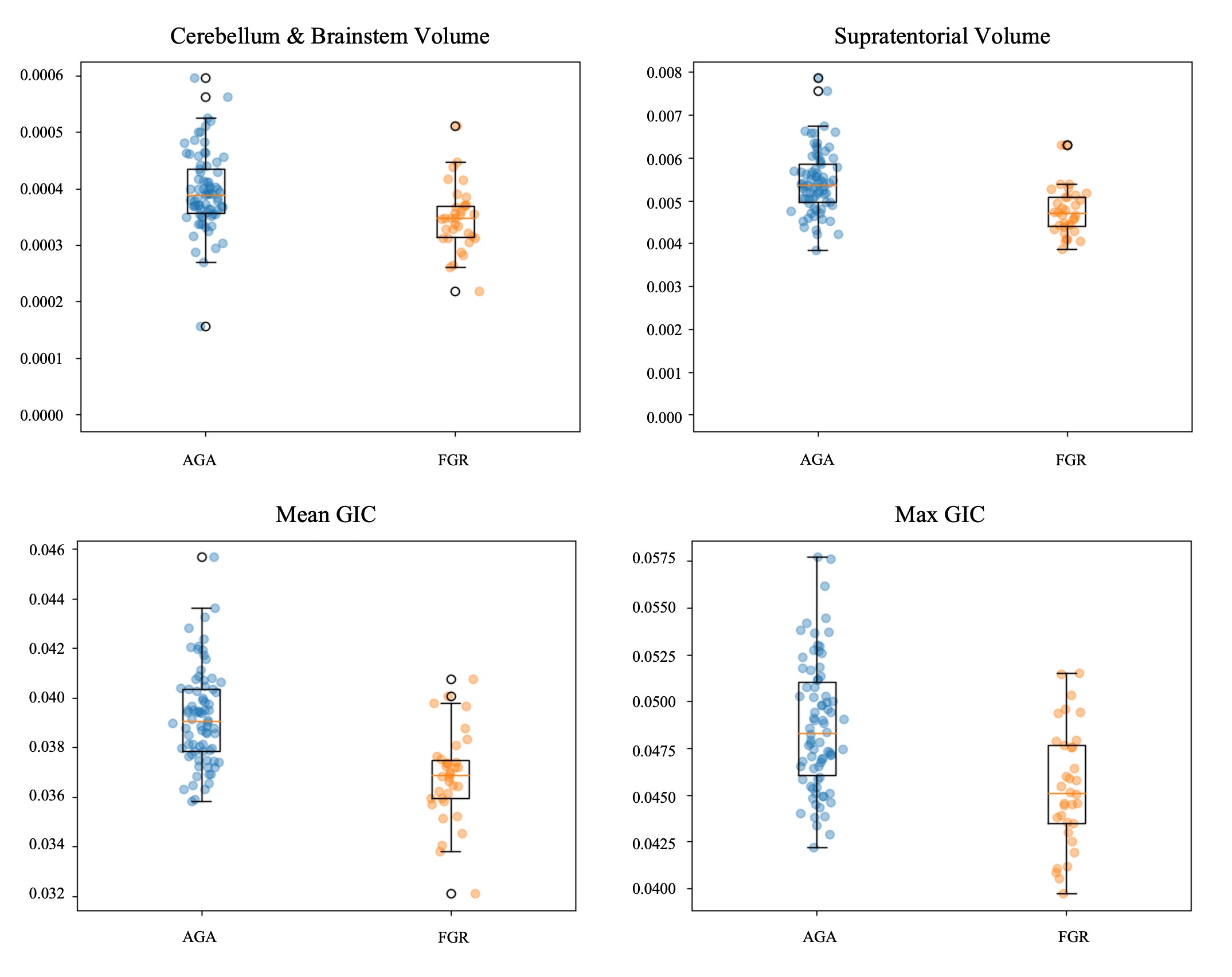
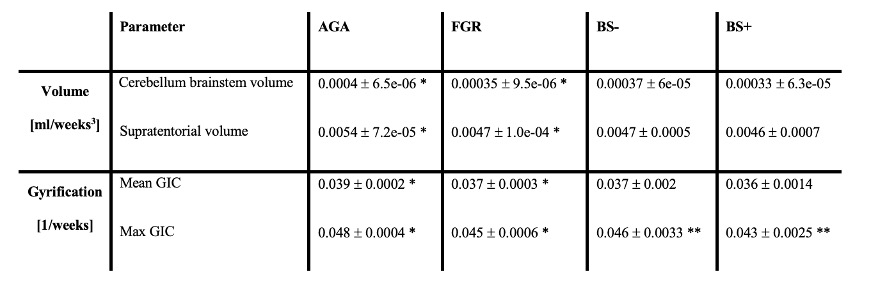
FGR and AGA: In the AGA group, supratentorial and cerebellum-brainsteam volumes showed significantly high correlation with GA, as expected. Significant decreased supratentorial and cerebellum-brainsteam volumes were measured in FGR fetuses compared with the AGA fetuses (P<0.001).Gyrification indices showed significant changes along GA. Both mean-GIC and max-GIC were significantly lower in FGR compared to AGA fetuses (P<0.001).
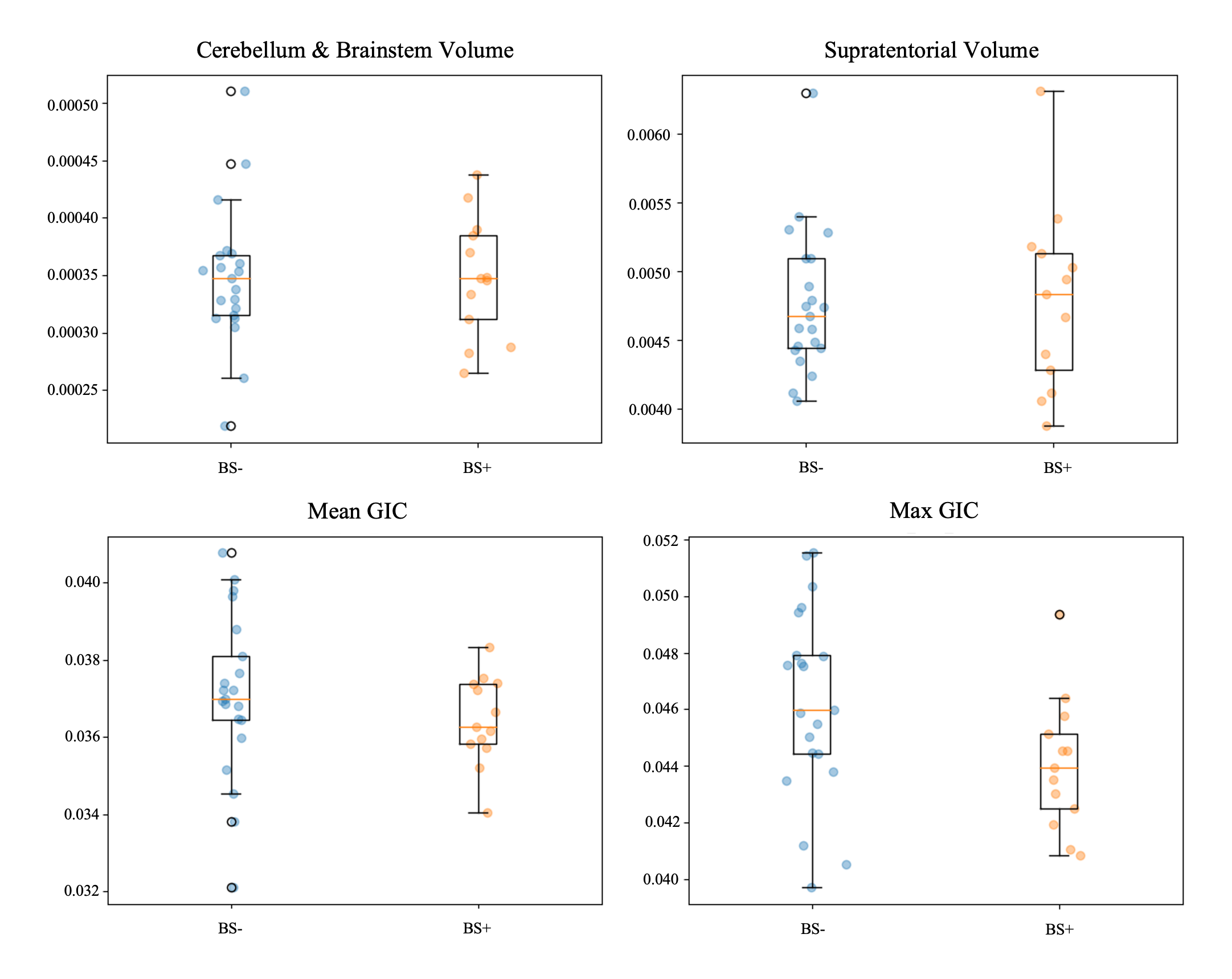
FGR with and without BS: No significant difference was measured for BS+ and BS- in supratentorial and cerebellum-brainsteam volumes.A significant decreased in max-GIC was detected for BS+ fetuses compared with BS- (P=0.04).
Results are shown in Table 1 and Figures 1 and 2.
Discussion
Our results demonstrate reduced brain volumes and delayed gyrification in FGR fetuses compared with AGA fetuses, corrocorating previous studies11–14. Delayed gyrification was more pronaounces in FGR fetuses with BS+, i.e MCA-PI<5th centile. Abnormal blood flow and redcued gyrification may indicate more sever growth restriction and may be connectedwith adverse neonetal outcome.Conclusion
This study presents brain changes, both in volume and in global gyrification of FGR fetuses, based on a relatively large clinical cohort. Quantifying the gyrification pattern may help assess the severity of the growth restriction, correlate with neuro-developmental outcome, and may provide additional information for pregnancy management.Acknowledgements
No acknowledgement found.References
1. Lees CC, Stampalija T, Baschat A, et al. ISUOG Practice Guidelines: diagnosis and management of small-for-gestational-age fetus and fetal growth restriction. Ultrasound in Obstetrics and Gynecology. 2020;56(2):298-312. doi:10.1002/uog.22134
2. Miller SL, Huppi PS, Mallard C. The consequences of fetal growth restriction on brain structure and neurodevelopmental outcome. Journal of Physiology. 2016;594(4):807-823. doi:10.1113/JP271402
3. Francis JH, Permezel M, Davey MA. Perinatal mortality by birthweight centile. Australian and New Zealand Journal of Obstetrics and Gynaecology. 2014;54(4):354-359. doi:10.1111/ajo.12205
4. Richardson BS, Bocking AD. Metabolic and circulatory adaptations to chronic hypoxia in the fetus. Comp Biochem Physiol A Mol Integr Physiol. 1998;119(3):717-723. doi:10.1016/s1095-6433(98)01010-1
5. Arcangeli T, Thilaganathan B, Hooper R, Khan KS, Bhide A. Neurodevelopmental delay in small babies at term: a systematic review. Ultrasound Obstet Gynecol. 2012;40(3):267-275. doi:10.1002/uog.11112
6. Miller SL, Huppi PS, Mallard C. The consequences of fetal growth restriction on brain structure and neurodevelopmental outcome. J Physiol. 2016;594(4):807-823. doi:10.1113/JP271402
7. Leitner Y, Fattal-Valevski A, Geva R, et al. Neurodevelopmental outcome of children with intrauterine growth retardation: a longitudinal, 10-year prospective study. J Child Neurol. 2007;22(5):580-587. doi:10.1177/0883073807302605
8. Scherjon S, Briët J, Oosting H, Kok J. The discrepancy between maturation of visual-evoked potentials and cognitive outcome at five years in very preterm infants with and without hemodynamic signs of fetal brain-sparing. Pediatrics. 2000;105(2):385-391. doi:10.1542/peds.105.2.385
9. Eixarch E, Meler E, Iraola A, et al. Neurodevelopmental outcome in 2-year-old infants who were small-for-gestational age term fetuses with cerebral blood flow redistribution. Ultrasound Obstet Gynecol. 2008;32(7):894-899. doi:10.1002/uog.6249
10. Peretz R, Halevy T, Gafner M, et al. Volumetric Brain MRI Study in Fetuses with Intrauterine Growth Restriction Using a Semiautomated Method. AJNR Am J Neuroradiol. 2022;43(11):1674-1679. doi:10.3174/ajnr.A7665
11. Basso A, Youssef L, Nakaki A, et al. Fetal neurosonography at 31-35 weeks reveals altered cortical development in pre-eclampsia with and without small-for-gestational-age fetus. Ultrasound Obstet Gynecol. 2022;59(6):737-746. doi:10.1002/uog.24853
12. Paules C, Miranda J, Policiano C, et al. Fetal neurosonography detects differences in cortical development and corpus callosum in late-onset small fetuses. Ultrasound Obstet Gynecol. 2021;58(1):42-47. doi:10.1002/uog.23592
13. Egaña-Ugrinovic G, Sanz-Cortes M, Figueras F, Couve-Perez C, Gratacós E. Fetal MRI insular cortical morphometry and its association with neurobehavior in late-onset small-for-gestational-age fetuses. Ultrasound Obstet Gynecol. 2014;44(3):322-329. doi:10.1002/uog.13360
14. Egaña-Ugrinovic G, Sanz-Cortes M, Figueras F, Bargalló N, Gratacós E. Differences in cortical development assessed by fetal MRI in late-onset intrauterine growth restriction. Am J Obstet Gynecol. 2013;209(2):126.e1-8. doi:10.1016/j.ajog.2013.04.008
15. Paules C, Miranda J, Policiano C, et al. Fetal neurosonography detects differences in cortical development and corpus callosum in late-onset small fetuses. Ultrasound Obstet Gynecol. 2021;58(1):42-47. doi:10.1002/uog.23592
16. Egaña-Ugrinovic G, Sanz-Cortés M, Couve-Pérez C, Figueras F, Gratacós E. Corpus callosum differences assessed by fetal MRI in late-onset intrauterine growth restriction and its association with neurobehavior. Prenat Diagn. 2014;34(9):843-849. doi:10.1002/pd.4381
17. Fields J, Dumaop W, Eleuteri S, et al. HIV-1 Tat alters neuronal autophagy by modulating autophagosome fusion to the lysosome: implications for HIV-associated neurocognitive disorders. J Neurosci. 2015;35(5):1921-1938. doi:10.1523/JNEUROSCI.3207-14.2015
18. Sanz-Cortes M, Egaña-Ugrinovic G, Simoes R V, Vazquez L, Bargallo N, Gratacos E. Association of brain metabolism with sulcation and corpus callosum development assessed by MRI in late-onset small fetuses. Am J Obstet Gynecol. 2015;212(6):804.e1-8. doi:10.1016/j.ajog.2015.01.041
19. Garel C, Chantrel E, Brisse H, et al. Fetal cerebral cortex: normal gestational landmarks identified using prenatal MR imaging. AJNR Am J Neuroradiol. 2001;22(1):184-189.
20. Gordijn SJ, Beune IM, Thilaganathan B, et al. Consensus definition of fetal growth restriction: a Delphi procedure. Ultrasound Obstet Gynecol. 2016;48(3):333-339. doi:10.1002/uog.15884
21. Yehuda B, Rabinowich A, Link-Sourani D, et al. Quantitative Assessment of Gyrification Patterns and Symmetry of the Fetal Brain based on Routine Fetal 2D MRI. In: ISMRM; 2023.
22. Dudovitch G, Link-Sourani D, ben Sira L, Miller E, ben Bashat D, Joskowicz L. Deep Learning Automatic Fetal Structures Segmentation in MRI Scans with Few Annotated Datasets. In: International Conference on Medical Image Computing and Computer-Assisted Intervention. ; 2020:365-374.
23. Ori Ben Zvi, Netanell Avisdris, Bossmat Yehuda, et al. Automatic segmentation of fetal brain components from MRI using deep learning. In: ISMRM . ; 2021.
Figures