2550
Hyperdynamic CSF flow is related to ventricular volumes and jugular venous flow in adolescents with congenital heart disease (CHD)1University Children's Hospital, Zurich, Switzerland
Synopsis
Keywords: Neuro, Neurofluids
Motivation: Enlarged CSF volumes have been reported in children with congenital heart disease (CHD), and have been linked to neurodevelopmental outcome, but the origin of these enlarged CSF volumes is not yet known.
Goal(s): To examine the link between CSF flow, arteriovenous flow and CSF volumes in order to improve our understanding of the observed changes in CSF volume.
Approach: Phase contrast MRI of the cerebral aqueduct, carotid arteries and jugular veins was combined with 3D anatomical MRI for segmentation of the CSF spaces.
Results: CHD children show hyperdynamic CSF flow, which is linked to enlarged 3rd ventricle volumes and venous flow.
Impact: An improved understanding of the link between heart defects and brain development and hydrodynamics may help to foster improved development and outcome for children with CHD in future.
Introduction
Accumulating evidence suggests that patients with congenital heart disease (CHD) show reduced brain volumes, which are linked to neurodevelopmental and cognitive deficits, (for a recent review, see: [1]). Cerebrospinal fluid (CSF) volumes have been less extensively studied in CHD, but enlarged CSF volumes have also been reported [2-4], and linked to developmental outcome [2,3]. However, the origin of these CSF volume changes in CHD is not yet known. One previous study in univentricular CHD reported a link between elevated venous pressure and increased CSF volumes. [5] Hence, increased venous pressure may contribute to the CSF volume changes, but these effects may only be relevant for the most severe univentricular cases. By examining the link between CSF flow, arteriovenous flow and CSF volumes it may be possible to improve our understanding of the origin of the observed changes in CSF volume. The aims of this study were twofold: firstly, to examine differences in CSF flow and volume in adolescents with CHD, aiming to reproduce findings from previous studies, and secondly to examine the link between CSF ventricular volumes, aqueductal CSF flow, and arteriovenous flow (AVF).Methods
After exclusion of datasets demonstrating motion, aliasing or other (e.g. susceptibility) artefacts, the final participant group included 88 adolescents, including 34 with complex CHD (18 female, mean age 13.6 years, range 10-15), who had been operated before age one, and 54 healthy controls (27 female, mean age 13.1 years, range 10-16). Cardiac-gated phase contrast MRI flow data were collected on a GE MR750 MRI scanner (GE HealthCare, Milwaukee, WI, USA), with TR/TE = 9.5/5.8 ms (CSF), 7.5/4.0 ms (AVF), FOV=180 mm, matrix 256x256, flip angle: 20 degrees, slice thickness= 4 mm, venc= 10 cm/s (CSF), 120 cm/s (AVF), and 30 cardiac phases. CSF flow was measured on a slice perpendicular to the aqueduct, and arteriovenous flow was assessed on a slice perpendicular to the internal carotid arteries. 3D T1-weighted cerebral MRI data were collected with an inversion-recovery prepared, spoiled gradient echo volume with TI/TE/TR= 600/5/11 ms and a voxel resolution of 1x1x1mm3, and segmented with FreeSurfer version 7.1. [6] The volumes of the lateral, 3rd, and 4th ventricles were extracted for comparison with the CSF flow data. CSF and AVF data were analysed with QFlow version 8.1 (Medis Suite 3.0, MEDIS Medical Imaging Systems, Leiden, The Netherlands), and the following parameters extracted for subsequent statistical analysis: peak CSF velocity, mean CSF velocity, mean CSF flow, forward CSF flow, backward CSF flow. The peak velocity, mean velocity, and mean flow in the left and right carotid arteries and jugular veins were also extracted for comparison with the CSF flow. Socioeconomic status (SES) was estimated from a parental education questionnaire. Groupwise differences in CSF flow parameters and ventricular volumes were tested with Mann-Whitney tests, and intercorrelations between flow parameters were assessed with Spearman correlations.Results
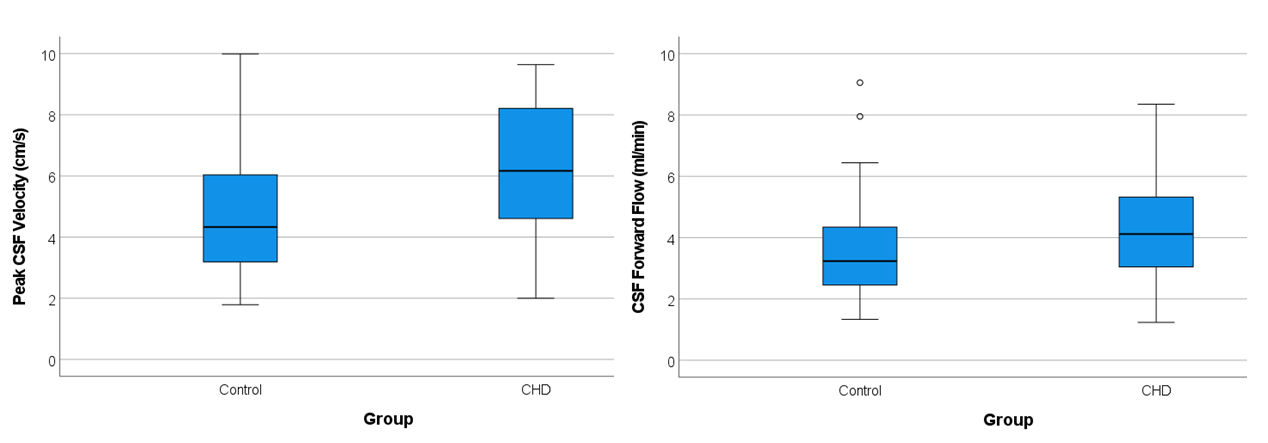
CHD and control groups did not differ significantly in age (p=0.100) or sex (p=0.79), but the controls had significantly higher SES (p=0.001). CHD participants showed significantly higher peak CSF velocity (p=0.006), higher forward flow (p=0.038), and a trend towards higher total flow (p=0.070) and backward flow (p=0.057). The volume of the 3rd ventricle was significantly enlarged in CHD (p=0.001), and this difference remained significant after covarying for SES and the total brain volume. The volume of the 3rd ventricle correlated positively with the peak CSF velocity (rho=0.417, p<0.001), forward flow (rho=0.552, p<0.001), backward flow (rho=0.468, p<0.001), and mean CSF flow (rho=0.394, p<0.001), and negatively with the average flow velocity in the right carotid artery (rho=-0.283, p=0.024). There were no significant intercorrelations between CSF flow and arterial flow parameters, but the peak CSF flow velocity correlated negatively with the right jugular venous flow (rho=-0.346, p=0.007). and positively with the left jugular flow (rho=0.261, p=0.044). The right jugular flow also correlated negatively with the CSF forward flow (rho=-0.266, p=0.040), and positively with the total brain volume (rho=0.350, p=0.006).Discussion
The increased peak CSF velocity, forward flow, and trend-level increase in backward flow are consistent with the hyperdynamic CSF flow reported previously in children with CHD. [7] The significant association between the 3rd ventricle volume and the total CSF flow also reproduces findings reported previously in an independent dataset. However, the link between venous and CSF flow extends these findings, indicating that the altered CSF flow and volume may be linked to alterations in venous flow, possibly resulting from alterations in venous pressure due to the heart defect.Acknowledgements
Swiss National Science Foundation (SNF 32003B_172914)References
- Aleksonis HA & King TZ. Relationships Among Structural Neuroimaging and Neurocognitive Outcomes in Adolescents and Young Adults with Congenital Heart Disease: A Systematic Review. Neuropsychol Rev. 2023 Jun;33(2):432-458.
- Knirsch W, et al. Structural cerebral abnormalities and neurodevelopmental status in single ventricle congenital heart disease before Fontan procedure. Eur J Cardiothorac Surg. 2017 Apr 1;51(4):740-746.
- Heye K., et al. Reduction of brain volumes after neonatal cardiopulmonary bypass surgery in single-ventricle congenital heart disease before Fontan completion. Pediatr Res. 2018 Jan;83(1-1):63-70. doi: 10.1038/pr.2017.20
- Lee VK, et al. Macroscopic Hyperdynamic CSF Flow and CSF Volume Analysis in Children and Adolescents with Congenital Heart Disease. Proc ISMRM 2019, abstract 0755.
- Reich B, et al. Interrelationship Between Hemodynamics, Brain Volumes, and Outcome in Hypoplastic Left Heart Syndrome. Ann Thorac Surg. 2019 Jun;107(6):1838-1844
- Dale AM, et al.. Cortical surface-based analysis. I. Segmentation and surface reconstruction. Neuroimage 9, 179-194 (1999)
- Macroscopic Hyperdynamic CSF and Ciliary Motion Dysfunction Predict Executive Dysfunction in Children and Adolescents with Congenital Heart Disease. Proc. ISMRM 2018, abstract 0849
Figures