2547
The lack of growth hormone is accompanied by decreased GABA+ concentrations and neuronal activity within the thalamus in short children1Sichuan Provincial people’s hospital, Chengdu, China, 2Department of clinical and technical support, Philips Healthcare, Xi’an, China, 3Department of clinical and technical support, Philips Healthcare, Chengdu, China
Synopsis
Keywords: Neuro, Metabolism
Motivation: It is unclear whether the lack of growth hormone (GH) is accompanied by altered GABA in human brain and relationship between the alterations and neuronal activity.
Goal(s): Thalamus is one of brain region that has highest concentration of GH receptors. The purpose of this study was to explore changes in GABA concentrations in thalamus and its association with neuronal activity in children with GHD.
Approach: We used MEGA-PRESS sequence to quantify the concentration of GABA+ in thalamus and rs-fMRI to assess neuronal activity.
Results: We found that the levels of thalamus GABA+ decreased significantly, and it was related to abnormal neuronal activity.
Impact: This study provides a new insight into the neural mechanisms of cognitive dysfunction in children with GHD, and holds a promising biomarker for us to find a new treatment approach to GHD.
Introduction
Growth hormone (GH) plays a pivotal role in proper development and functioning of the human brain, with thalamus being one of the brain regions that boasts the highest concentration of GH receptors[1-3]. GH deficiency (GHD) is a recognized endocrine abnormality, with an incidence rate as high as 1/4000 in children, which present as defects of linear growth and is more likely to have cognitive deficits[3-6]. Gamma-aminobutyric acid (GABA) is one of major inhibitory neurotransmitter in human brain. It plays a crucial regulatory role in brain function and involved in the regulation of GH[7, 8]. Therefore, it is important to understand whether the lack of GH in children is associated with changes in GABA levels in brain and to explore the relationship between the alterations and the brain activity.This study aims to explore the changes in GABA concentrations in thalamus, and its association with neuronal activity in children with GHD by using magnetic resonance spectroscopy (MRS) and resting-state functional MRI (rs-fMRI) methods.
Materials and Methods
In this study, 7 children with GHD and 8 children with idiopathic short stature (ISS, GH not deficiency) were recruited. Data were collected using a 3.0 T MR scanner (lngenia Elition, Philips Healthcare, the Netherlands) with a 32-channel head coil. The MRS data was acquired by MEscher-GarwOod point resolved spectroscopy (MEGA-PRESS) sequence. For each participant, a 30 × 20 × 20 mm3 volume of interest (VOI) was placed at thalamus. The parameters of the MEGA-PRESS were as follows: TR/TE = 2000/68 ms, Gaussian editing pulses at 1.89 parts per million (ppm) of the proton frequency (edit-ON) and 7.46 ppm (edit-OFF), 288 averages, 1024 acquisition points and scanning duration = 612 seconds. Variable power and optimized relaxation delays was used for water suppression. MRS data were analyzed using Gannet 3.0 (http://www.gabamrs.com/)[9]. The measured GABA concentration using MEGA-PRESS protocol commonly referred to as GABA+ with the contribution from macromolecules. The contents of GABA+ and Glx (glutamate and glutamine) in gray matter were evaluated with spm12 toolbox.The BOLD date was acquired by SE-EPI sequence with the parameters as: TR/TE = 2000/35 ms, 220 time points, spatial resolution = 3 x 3 x 4 mm3 and scanning duration = 440 seconds. The static amplitude of low-frequency fluctuation (sALFF) and dynamic ALFF (dALFF) metrics were performed to explore the alteration of brain activity. Rs-fMRI data was processed using DPABI toolbox (https://www.rfmri.org/DPABI). Statistical analysis was performed by SPSS v25.0. The comparison of group differences was performed by using independent sample t-test. Voxel-wise two-sample t-tests were implemented within the thalamus mask to assess differences in sALFF and dALFF between two group using DPABI toolbox.
Results
The demographic data were shown in Table 1. VOl of MRS was placed at thalamus (Figure 1A). A typical GABA+ / Glx spectra obtained from thalamus were shown in Figure 1B. Compared with ISS group, the GABA+ concentration in thalamus significantly decreased in GHD group (Table 1). Similarly, GHD group showed decreased sALFF and dALFF in the left thalamus (Table 2 and Figure 2) compared with ISS group. The results of correlation analysis were shown in Figure 3. The concentration of GABA+ was positively correlated with IGF-1 (r = 0.767, p = 0.044), sALFF (r = 0.769, p = 0.043) and dALFF (r = 0.805, p = 0.029) in GHD group. Meanwhile, the abnormal IGF-1 was significantly positively correlated with sALFF (r = 0.758, p = 0.048) and dALFF (r = 0.822, p = 0.023).Discussion
In this study, we investigated the neurochemical transmitters (GABA+ and Glx), neuronal activity of thalamus (sALFF and dALFF) and their relationship with clinical indices (IGF-1) in children with GHD. The main results were as follows: First, the GABA+ levels of thalamus in GHD group decreased significantly, and it was related to abnormal sALFF, dALFF and IGF-1. The decrease of IGF-1 is related to the severity of GHD[10]. Thus, these results suggest that the lack of GH in children is accompanied by altered GABA in thalamus, and dysfunction in thalamus is related to the imbalance of GABA+. Secondly, the IGF-1 was related to abnormal sALFF and dALFF in GHD group, indicating that GH may directly influence the thalamic function besides the alteration of GABA+.Conclusion
This study revealed a decrease trend in GABA+ levels in thalamus associated with thalamic activity in children with GHD. These results provide a new insight into the neural mechanisms of cognitive dysfunction in children with GHD, and holds a promising biomarker for us to find a new treatment approach to GHD.Acknowledgements
We are grateful to all the participants for their cooperation.References
1. SONNTAG W E, RAMSEY M, CARTER C S. Growth hormone and insulin-like growth factor-1 (IGF-1) and their influence on cognitive aging [J]. Ageing Res Rev, 2005, 4(2): 195-212.
2. YUAN T, YING J, JIN L, et al. The role of serum growth hormone and insulin-like growth factor- 1 in adult human brain morphology [J]. Aging, 2020, 12(2): 1377-96.
3. WEBB E A, O'REILLY M A, CLAYDEN J D, et al. Effect of growth hormone deficiency on brain structure, motor function and cognition [J]. Brain, 2012, 135(1): 216-27.
4. SAVAGE M, STORR H, BACKELJAUW P. The continuum between GH deficiency and GH insensitivity in children [J]. Rev Endocr Metab Disord, 2021, 22(1): 91-9.
5. MURRAY P, DATTANI M, CLAYTON P. Controversies in the diagnosis and management of growth hormone deficiency in childhood and adolescence [J]. Arch Dis Child, 2016, 101(1): 96-100. 6. HU Y, LIU X, CHEN X, et al. Differences in the functional connectivity density of the brain between individuals with growth hormone deficiency and idiopathic short stature [J]. Psychoneuroendocrinology, 2019, 103: 67-75.
7. POWERS M J M, SCIENCE S. GABA supplementation and growth hormone response [J]. 2012, 59: 36-46.
8. DUMAN R, SANACORA G, KRYSTAL J J N. Altered Connectivity in Depression: GABA and Glutamate Neurotransmitter Deficits and Reversal by Novel Treatments [J]. 2019, 102(1): 75-90.
9. EDDEN R, PUTS N, HARRIS A, et al. Gannet: A batch-processing tool for the quantitative analysis of gamma-aminobutyric acid–edited MR spectroscopy spectra [J]. 2014, 40(6): 1445-52.
10. AGUIAR-OLIVEIRA M, GILL M, DE A BARRETTO E, et al. Effect of severe growth hormone (GH) deficiency due to a mutation in the GH-releasing hormone receptor on insulin-like growth factors (IGFs), IGF-binding proteins, and ternary complex formation throughout life [J]. J Clin Endocrinol Metab, 1999, 84(11): 4118-26.
Figures
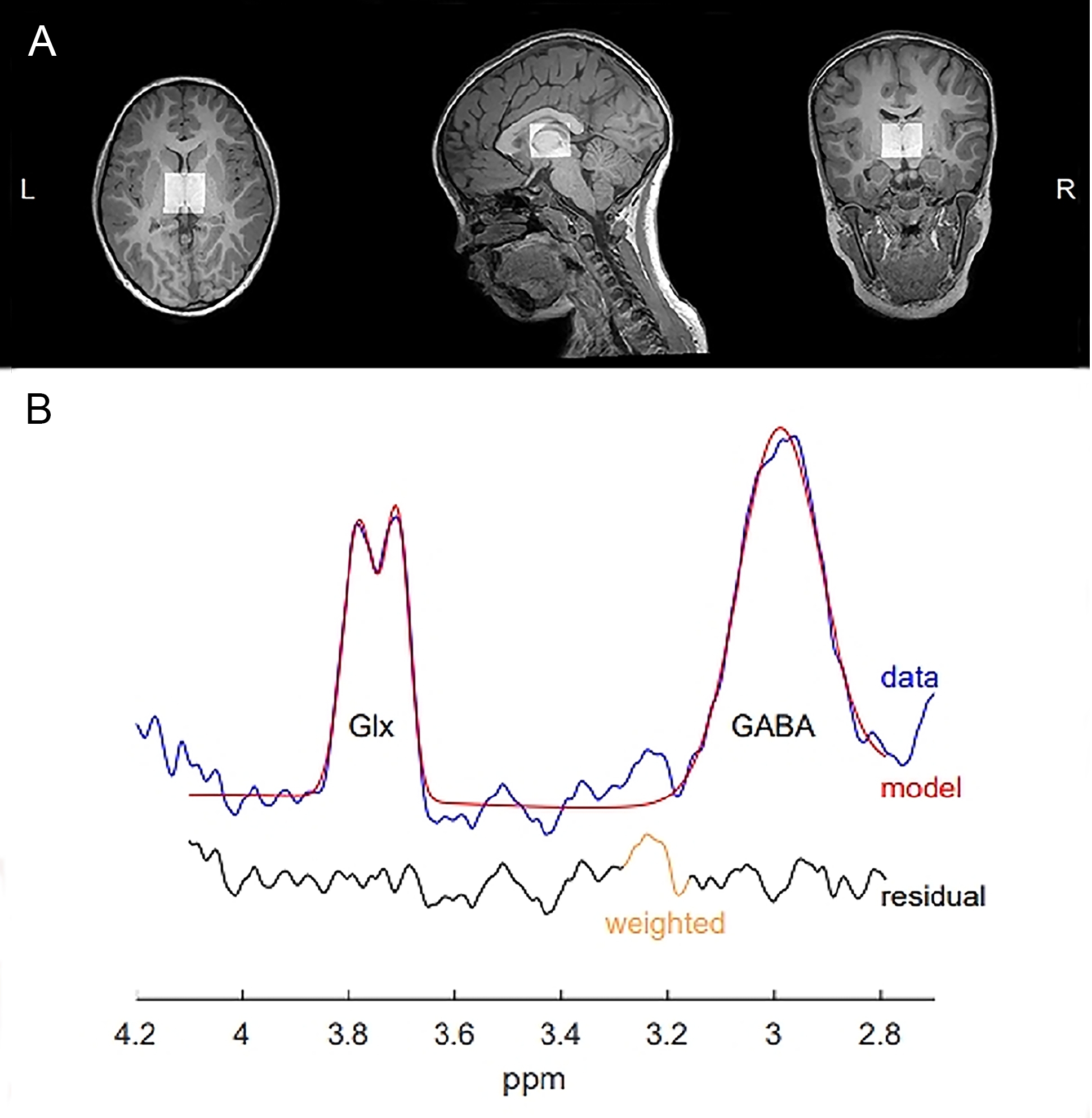
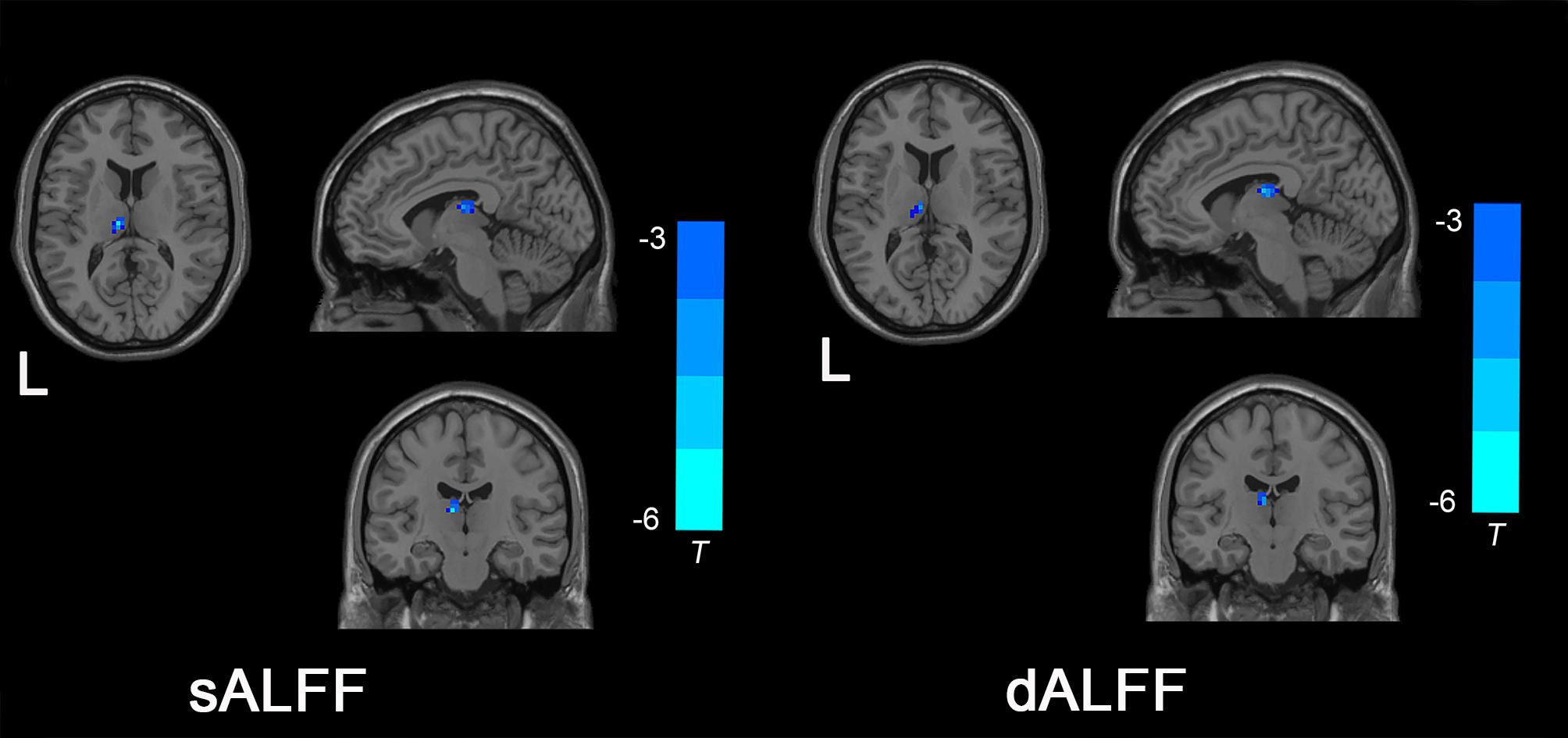
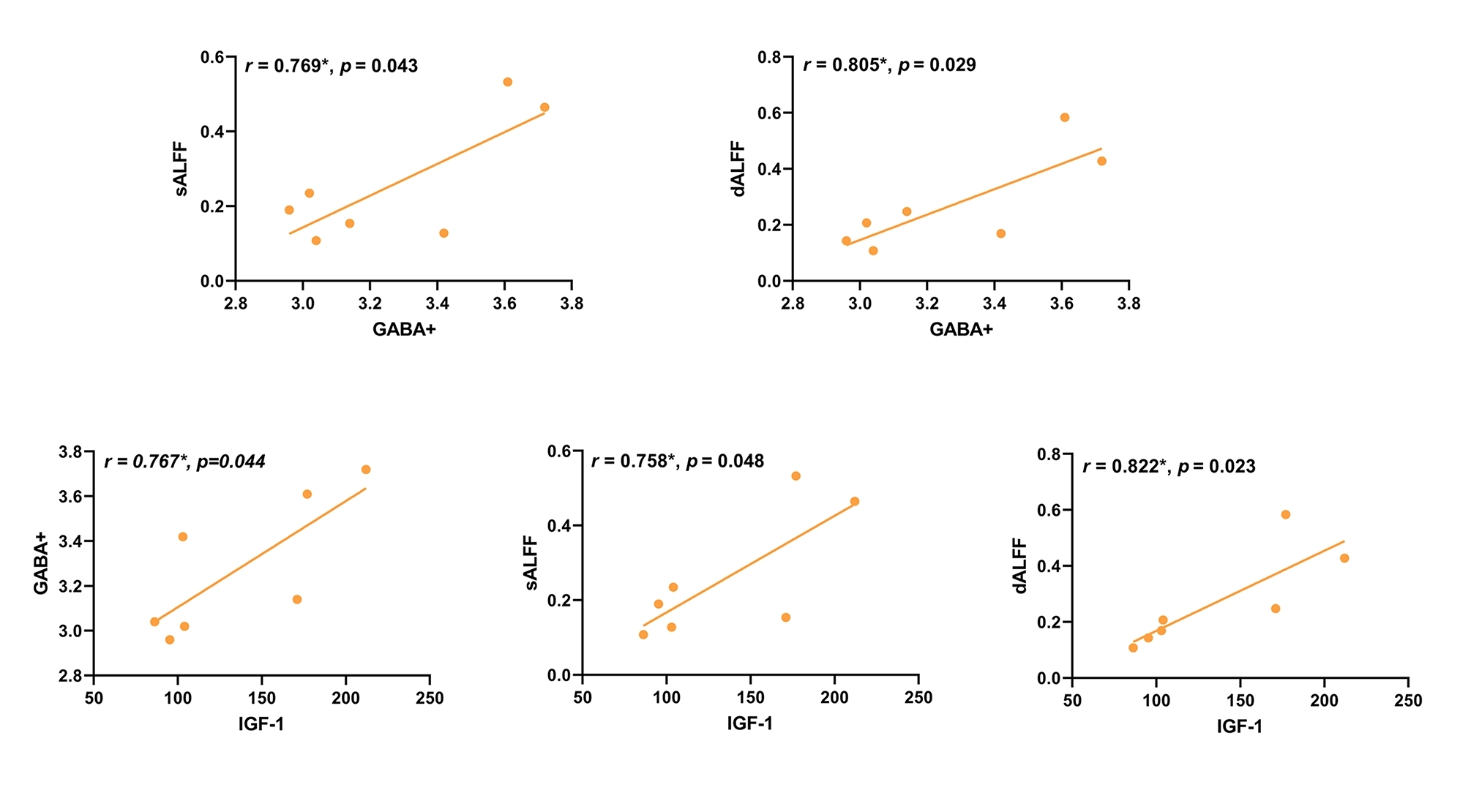
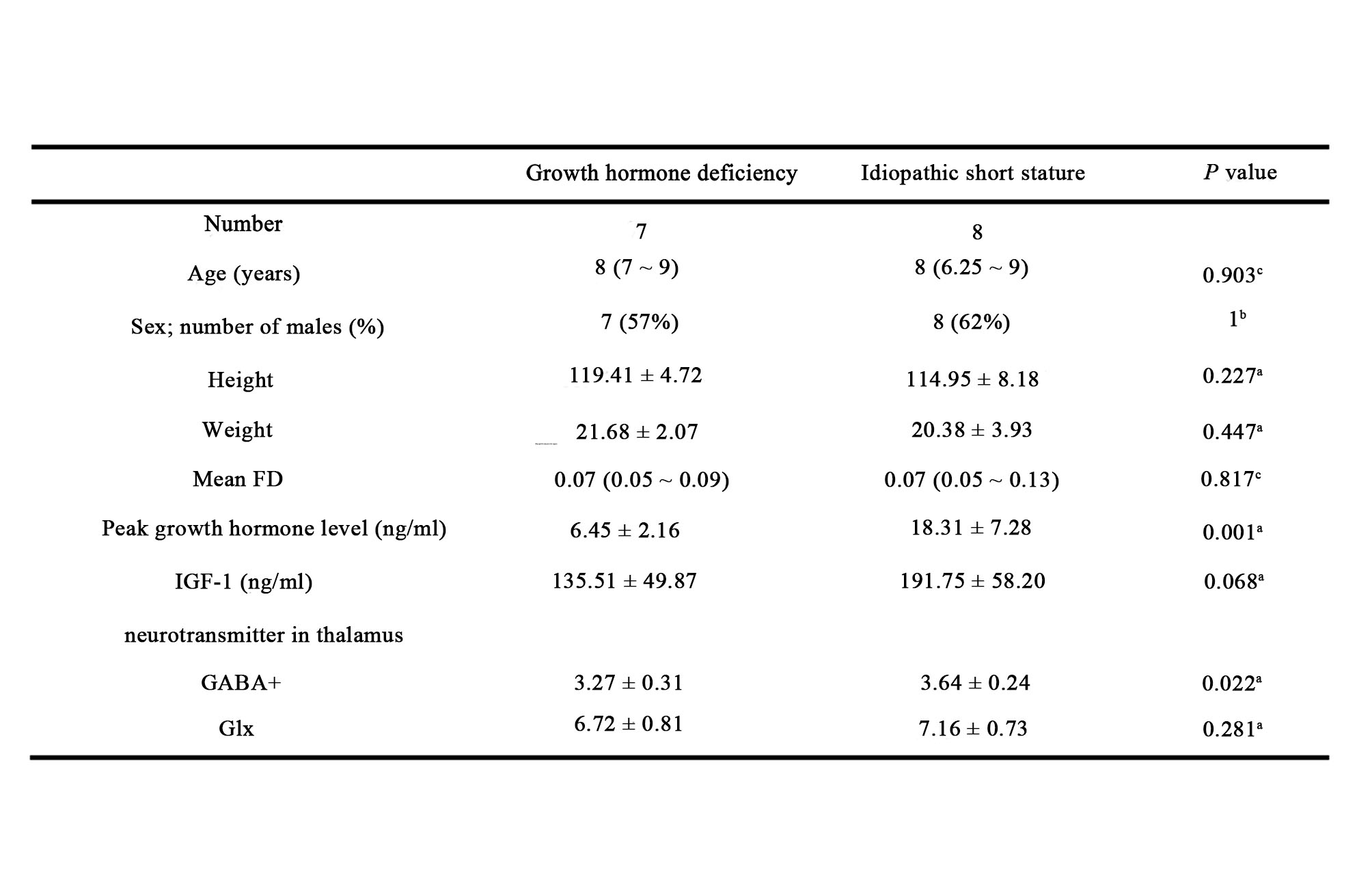
Table 1. Demographic characteristics and neurotransmitters in children with GHD and ISS.
Notes: a, independent two-sample t-test; b, fisher's exact test; c, Mann-Whitney U test. Abbreviations: GHD, growth hormone deficiency; ISS, idiopathic short stature; FD, framewise displacement; GH, growth hormone; IGF-1, insulin-like growth factor-1; GABA+, Gamma-aminobutyric acid; Glx, glutamate + glutamine.
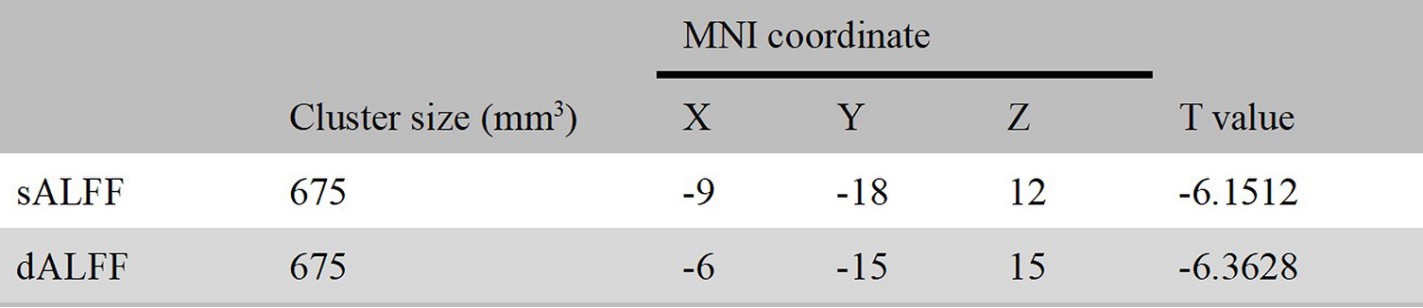
Table 2. sALFF and dALFF in GHD group significantly lower than those in ISS group in left thalamus (voxel level p < 0.005, cluster level p < 0.05, GRF corrected).