2543
Validation of Semi-quantitative Brain Dysmaturation Score in Congenital Heart Disease: Correlated with Executive Function and Ciliary Motion1Department of Bioengineering, University of Pittsburgh, Pittsburgh, PA, United States, 2Department of Radiology, University of Pittsburgh School of Medicine, Pittsburgh, PA, United States, 3Department of Biomedical Informatics, University of Pittsburgh School of Medicine, Pittsburgh, PA, United States, 4Learning and Development Center, Child Mind Institute, New York, NY, United States, 5Department of Developmental Biology, University of Pittsburgh, Pittsburgh, PA, United States
Synopsis
Keywords: Neuro, Adolescents, Congenital Heart Disease Neurodevelopment Brain Dysmaturation Evaluation Method
Motivation: Develop and validate point-of-care MRI-based evaluation method for scoring brain dysplasia/abnormality (BDS) in congenital heart disease (CHD) that incorporates morphological alterations and subcortical structures.
Goal(s): Further develop our BDS system, previously validated in infants with CHD, in the older pediatric and young adult CHD population.
Approach: Evaluate brain dysplasia from T1 and T2 structural MRI of CHD and control participants and compare differences. Correlate BDS with executive function outcomes and genetic ciliary motion (CM) abnormalities.
Results: CHD group had higher total and subcortical dysplasia, especially single ventricle CHD group. Higher BDS (greater dysplasia) correlated with poorer executive function outcomes and greater CM abnormality.
Impact: Our BDS method is sensitive to dysmaturational features in CHD and correlated with executive function outcomes and CM - genetic-basis of CHD pathogenesis. Since it employs common point-of-care MRI techniques, it could be adapted for wider application in CHD brain evaluation.
INTRODUCTION
Children with congenital heart disease (CHD) face an elevated risk of developing brain dysmaturation, a generalized term encompassing abnormal and delayed development of brain macro- and microstructure.1-5 They also higher risk for acquired brain injuries, including infarcts and small vessel disease across lifespan as detected by conventional neuroimaging studies. Additionally, recently published guidelines engendered an increased clinical neuroimaging of patients during the peri-operative period. Most conventional semi-quantitative MRI scoring systems in CHD patients have focused on either acquired brain injury or cortical maturation, particularly in the neonatal period. We recently developed and validated a semi-quantitative score for infants that extends beyond cortical maturation and acquired brain injury to encompass morphological alterations in subcortical structures (cerebellum, hippocampus, olfactory bulb), cerebrospinal fluid (CSF), and the corpus callosum know as a brain dysplasia score (BDS), informed by preclinical CHD models.1 We have previously shown that BDS correlated with cortical maturation, white matter connectivity, genetic ciliary motion (CM), metabolism, and early neurodevelopmental outcomes.6-8 Our primary aim was to further develop BDS to detect abnormalities in CHD child/adolescent/young adult participants and examine links with executive function, an area of cognition often disrupted in this population. Our secondary aim was to correlate BDS with ciliary motion, the genetic component underpinning CHD pathogenesis.METHODS
A total of 240 participants (CHD=152, female=40, 14.47±7.02 years; Healthy Controls=88, female=46, 13.53±3.99 years) were prospectively recruited, with 222 (CHD=135; Healthy Controls=87) receiving an MRI scan. A 3T Skyra (Siemens Healthcare, Erlangen, Germany) with 32-channel head coil was used to acquire isotropic T1 and T2 structural images with the same resolution (matrix=256x256; resolution=1.0x1.0x1.0 mm) for brain dysmaturation assessment. Each participant’s scan was evaluated by two pediatric neuroradiologists with over 20 years of experience, as detailed previously (Panigrahy, 2016).1 BDS is determined by examining the following structures: cerebellar hemispheres and vermis; olfactory bulbs and sulci; hippocampus, choroid plexus, brain stem, corpus callosum, and extra-axial CSF. Higher BDS indicates a greater degree of brain dysmaturation. Of these participants, 136 (CHD=116; Controls=20) had CM assessment scored by three experts using a four-point scale, with higher score denoting greater motion abnormality.9 Participants underwent executive function tests and their parents rated their skills for the following domains: (1) Cognitive Flexibility: National Institutes of Health Toolbox (NIHtb) Dimensional Change Card Sort Test (DCCS), Delis-Kaplan Executive Function System (D-KEFS) Trail Making Test (TMT), and Behavior Rating Inventory of Executive Function, Parent Report (BRIEF) Shift; (2) Inhibition: NIHtb Flanker Inhibitory Control and Attention Test (Flanker), D-KEFS Color-Word Interference Test (CWIT), and BRIEF Inhibition; (3) Working Memory: NIHtb List Sorting Test, Wechsler Intelligence Scale for Children, 4th Edition (WISC-IV) or Wechsler Adult Intelligence Scale, 4th Edition (WAIS-IV) Letter-Number Sequencing, and BRIEF Working Memory.Differences in BDS between controls and CHD, and CHD subdivided by hypoplastic left heart single ventricle (SV) and biventricular (BV) groups, were analyzed. BDS was correlated with CM scores and reanalyzed with CHD status as covariate. Lastly, multivariable regression analyses between total BDS and executive function were conducted with number of ventricles and Childhood Opportunity Index as covariates.
RESULTS
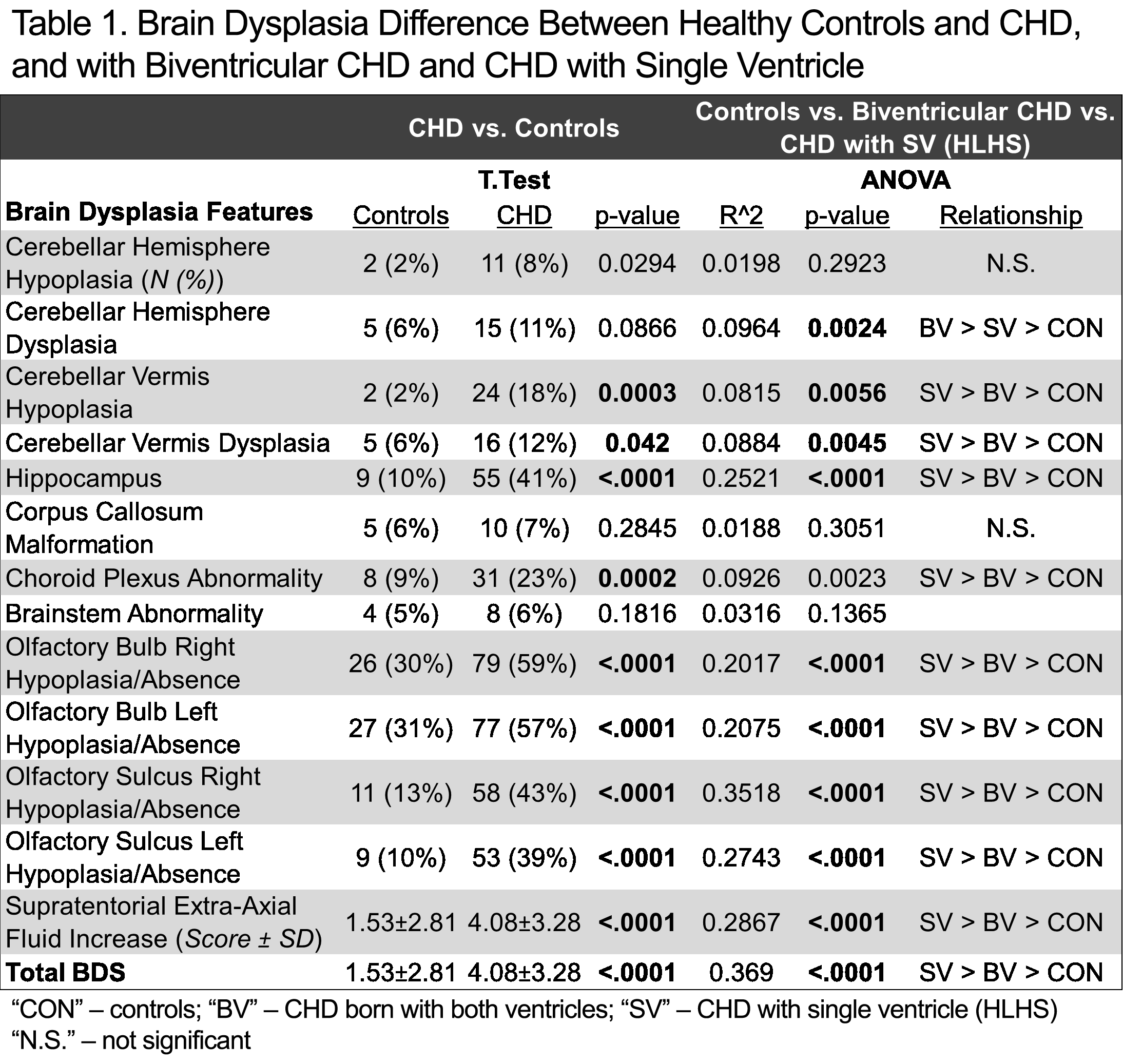
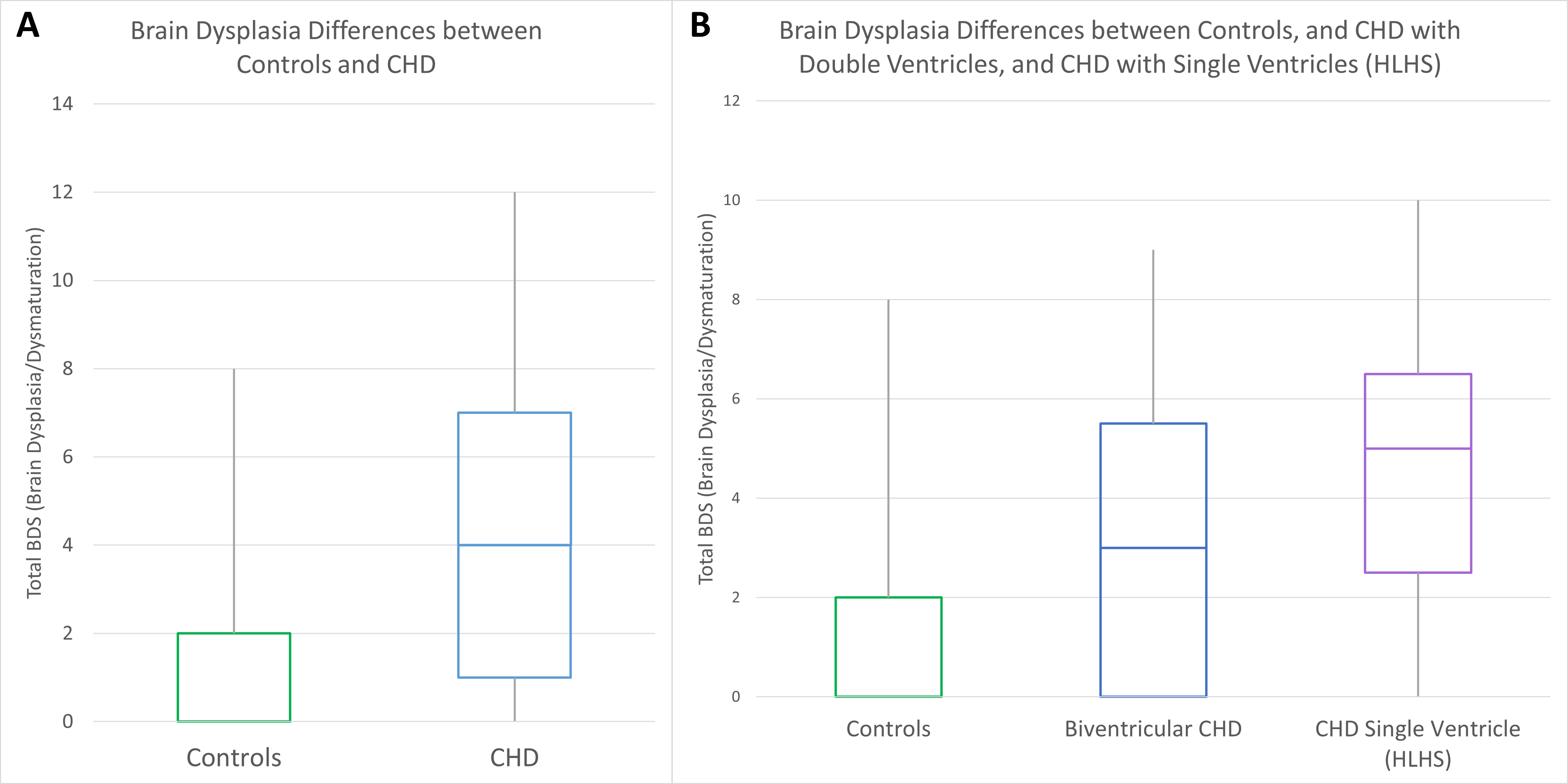
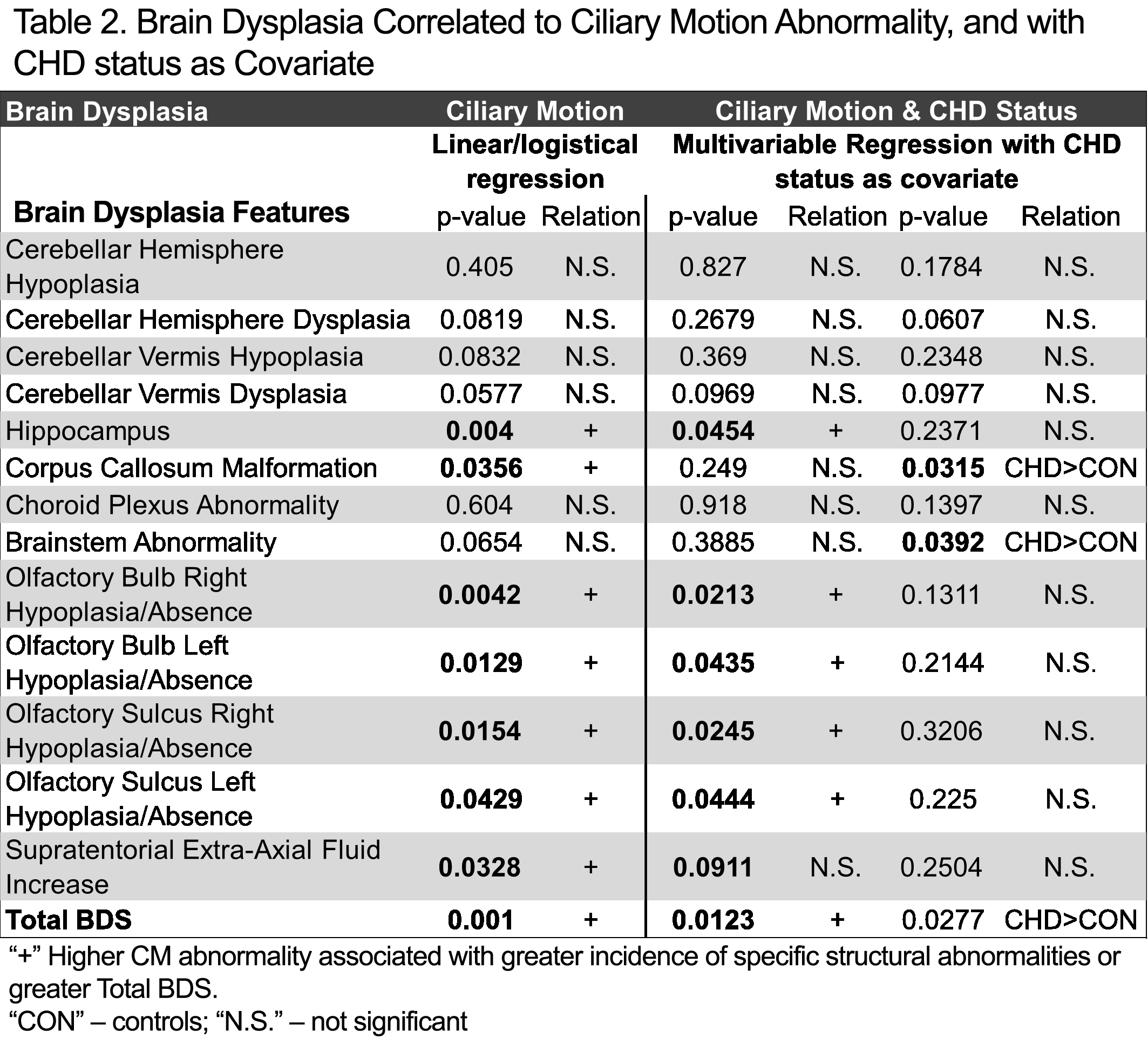
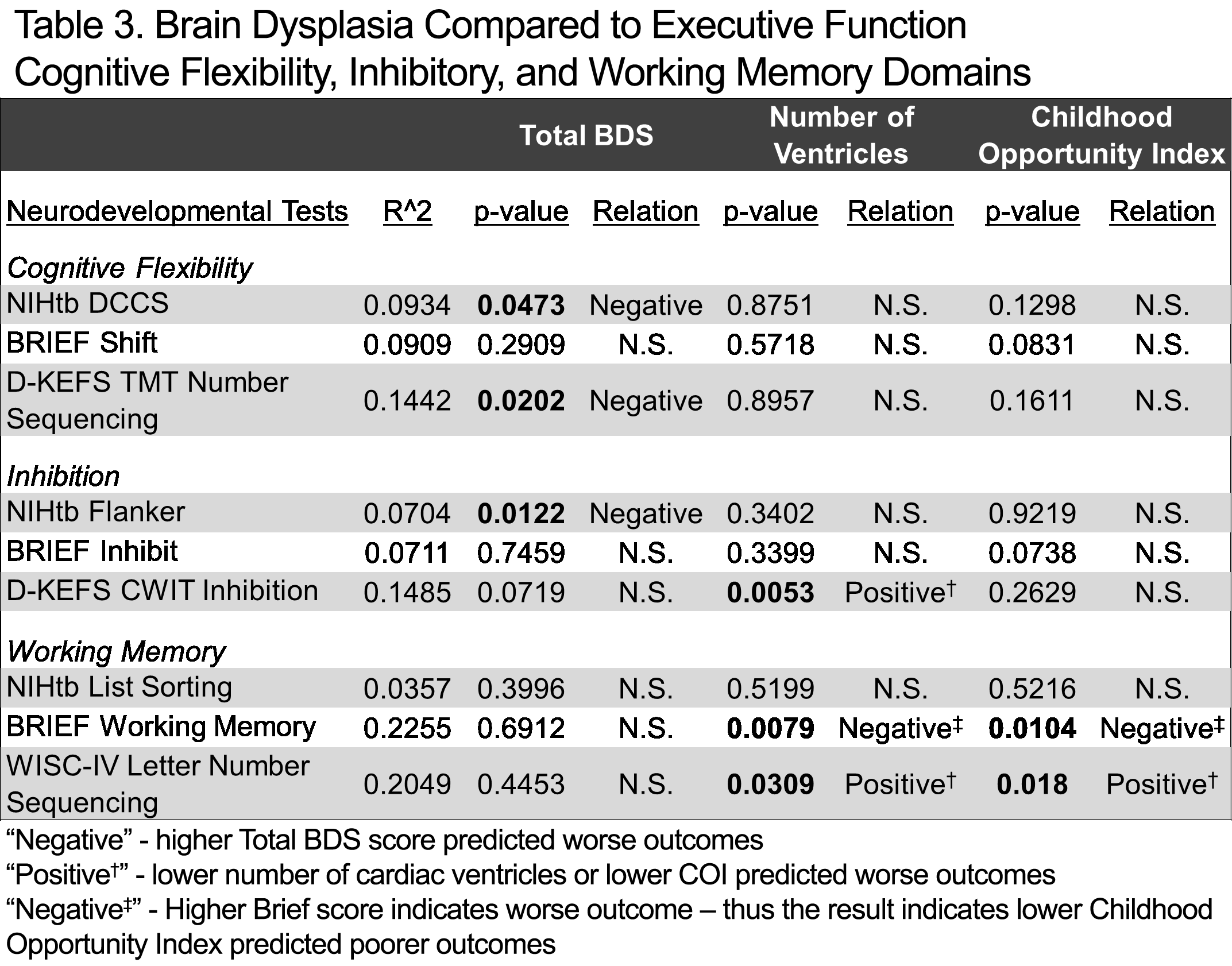
The CHD group had higher dysmaturation in subcortical components of BDS: cerebellar hypoplasia (Hemisphere p=0.0294; Vermis p=0.0003); hippocampus (p<0.0001) and choroid plexus (p=0.0002) abnormality; olfactory bulb and sulci hypoplasia (p<0.0001); increased Extra-Axial CSF (p<0.0001); and consequently, higher overall total BDS than the control group (Table 1). When CHD was stratified by cardiac ventricle subgroups, the SV group exhibited higher total BDS (p<0.0001) (Figure 1). Greater CM abnormality was correlated with greater incidence of abnormal findings in hippocampus, corpus callosum, olfactory bulb and sulci, increased extra-axial CSF, and higher BDS (p=0.0010) (Table 2). Even when accounting for CHD status, these associations between CM dysfunction and brain dysmaturation (except corpus callosum) remained significant. The multivariable regression demonstrated that greater brain dysmaturation predicted poor cognitive flexibility (NIHtb DCCS p=0.0473 and D-KEFS TMT p=0.0202) and inhibitory control (NIHtb Flanker p=0.0122).DISCUSSION
Our BDS is sensitive to dysmaturational differences between CHD and healthy controls among children, adolescents, and young adults, and is predictive of executive dysfunction. Additionally, within this CHD cohort, we observed greater incidence of subcortical dysmaturational components of BDS compared to controls, which follows our findings in neonates with CHD. Just as we found in neonates, abnormal CM was significantly associated with BDS in this older CHD population suggesting a common genetic mechanism that may persist across the lifespan. As clinical brain MRI use becomes more prevalent in cardiac neurodevelopmental practice, the BDS may be a useful point-of-care tool to assess not only acquired brain injury but also brain dysmatuation across the lifespan, pending further validation.Acknowledgements
Grant Support from: Department of Defense [Grant reference: W81XWH-16-1-0613], University of Pittsburgh Clinical and Translational Science Institute (CTSI UL1 TR0018570), and National Institutes of Health, National Heart, Lung, and Blood Institute [Grant reference: F31 HL165730-01]References
- Panigrahy A, Lee V, Ceschin R, et al. Brain dysplasia associated with ciliary dysfunction in infants with congenital heart disease. The Journal of pediatrics. 2016;178:141-148. e1.
- Ceschin R, Zahner A, Reynolds W, et al. A computational framework for the detection of subcortical brain dysmaturation in neonatal MRI using 3D Convolutional Neural Networks. NeuroImage. 2018;178:183-197.
- Heye KN, Knirsch W, Latal B, et al. Reduction of brain volumes after neonatal cardiopulmonary bypass surgery in single-ventricle congenital heart disease before Fontan completion. Pediatric research. 2018;83(1):63-70.
- von Rhein M, Buchmann A, Hagmann C, et al. Severe congenital heart defects are associated with global reduction of neonatal brain volumes. The Journal of pediatrics. 2015;167(6):1259-1263. e1.
- Watson CG, Stopp C, Wypij D, Newburger JW, Rivkin MJ. Reduced cortical volume and thickness and their relationship to medical and operative features in post-Fontan children and adolescents. Pediatric research. 2017;81(6):881-890.
- Badaly D, Beers SR, Ceschin R, et al. Cerebellar and Prefrontal Structures Associated with Executive Functioning in Pediatric Patients with Congenital Heart Defects. Frontiers in Neurology. 2022;13
- Schmithorst VJ, Votava‐Smith JK, Tran N, et al. Structural network topology correlates of microstructural brain dysmaturation in term infants with congenital heart disease. Human brain mapping. 2018;39(11):4593-4610.
- Harbison AL, Votava-Smith JK, Del Castillo S, et al. Clinical factors associated with cerebral metabolism in term neonates with congenital heart disease. The Journal of pediatrics. 2017;183:67-73. e1.
- Garrod AS, Zahid M, Tian X, et al. Airway ciliary dysfunction and sinopulmonary symptoms in patients with congenital heart disease. Annals of the American Thoracic Society. 2014;11(9):1426-1432.
Figures