2535
Initial results in pediatric volunteers using a silent and motion corrected ZTE protocol1Radiology, University of Iowa, Iowa city, IA, United States, 2Champaign Imaging, LLC, Minneapolis, MN, United States, 3Electrical and Computer engineering, University of Iowa, Iowa city, IA, United States
Synopsis
Keywords: Neuro, Motion Correction, Quiet
Motivation: Improve imaging for pediatric subjects by reducing loud acoustic noise and accommodating subject motion.
Goal(s): Develop a ZTE-based silent and motion-corrected neuroimaging protocol in pediatric subjects.
Approach: Nine pediatric volunteers were imaged with a protocol consisting of silent ZTE based T1w and T2w acquisitions and conventional Cartesian 3D gradient echo T1 MPRAGE and T2 FSE-CUBE. Images were reviewed and scored by a board-certified radiologist to assess overall image quality.
Results: Radiologist review indicates relatively comparable image quality for the ZTE acquisitions versus the conventional acquisitions. Motion induced blurring of some brain structures during motion was reduced using ZTE with motion correction.
Impact: This approach shows promise for studies in sensitive populations such as pediatrics with ear disorders and autism spectrum disorder.
Introduction
Pediatric neuroimaging studies rely on imaging pulse sequences that are based on conventional Cartesian encoding methods. Nevertheless, the high imaging gradient slew rates and amplitude of these techniques can lead to significant acoustic noise, which can lead to difficulty in studying sensitive populations such as pediatric population with developmental disorders such as autism, pediatric patients with inner ear disorders, or pediatric patients with psychiatric conditions such as depression. Acquisition strategies such as zero-echo time (ZTE) have been shown to allow silent imaging capabilities [1]. Furthermore, a radial ZTE approach can be improved read-out trajectories that can allow correction or provide motion robustness. We present initial results from our high resolution, motion corrected, quiet ZTE-based protocol for pediatric neuroimaging.Methods
Nine healthy pediatric volunteers (7-15 years) and one adult volunteer were imaged for this IRB approved study after receiving informed written consent. Imaging was performed on a 3T clinical MRI (Premier, GE Healthcare, Waukesha, WI) using a custom built 12 ch excite/receive array pediatric head coil designed for fast excite/receive switching time (pediatric studies) (Champaign Imaging/Scanned) or a 48ch receive array head coil (adult study) (GE Healthcare). The pediatric imaging protocol consisted of: 1) anatomic localizer, 3D ZTE based 2) T1w and 3) T2w acquisitions and conventional Cartesian 3D 4) gradient echo T1 MPRAGE and 5) T2 FSE-CUBE. Acquisition parameters for ZTE included 25.6 cm isotropic FOV, 256 acquired matrix isotropic, +/-31.25kHz BW and contrast was achieved using intermittent magnetization preparation pulses (T1: adiabatic inversion pulse or T2: 180° BIR-4) that were performed at the start of each segmented readout block consisting of collecting 192 angularly optimized ZTE FID radial lines using the HEALPix approach [2]. Coil sensitivity functions for all scans were estimated using JSENSE [3; 4]. Cartesian images were reconstructed via standard Fourier transform or with SENSE [5] when accelerated. ZTE images were reconstructed using TV regularized CG-SENSE [6] with time-efficient gridding [5] and Pipe-Menon sampling density compensation [6] using in-house python scripts based on SigPy [7]. Motion was estimated from ZTE data using the k-space data using the K-MoCo self supervised machine learning approach [8, 9] and corrected during reconstruction. Cartesian T1w scan parameters included TR/TE/TI= 2.46 sec/2.6 ms/1.06 sec, 8 deg. flip, FOV 25.6cm, 256x256x180 acquired matrix, +/-31.25kHz BW and 5:13 (min:sec) scan time. Cartesian T2w scan parameters included TR/TE = 2.99sec / effective 59.9ms, FOV 25.6cm, 256x256x180acquired matrix, +/-62.5kHzBW and 5:10 (min:sec) scan time. The adult volunteer was scanned for four repeat T1w ZTE acquisitions and the subject was asked to hold still during the first acquisition followed by progressively greater motion for each of the three subsequent scans. Images from the pediatric study were reviewed and scored by a board-certified radiologist to assess overall image quality.Results
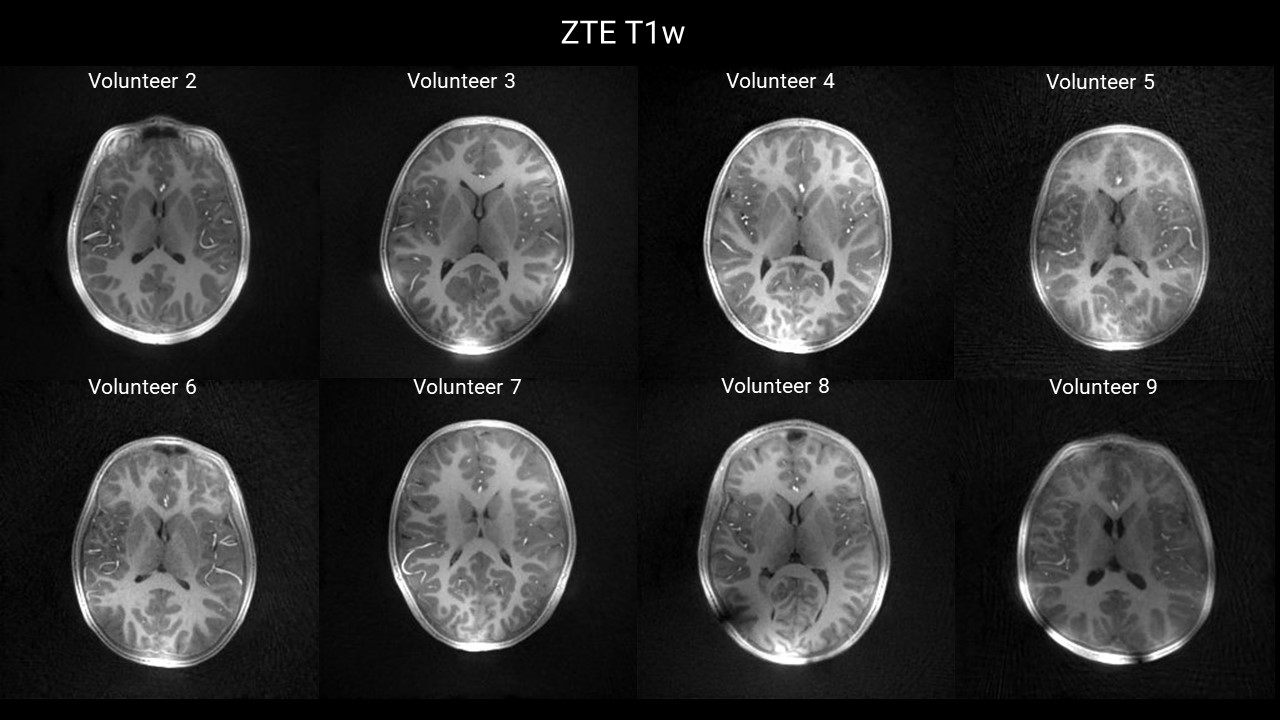
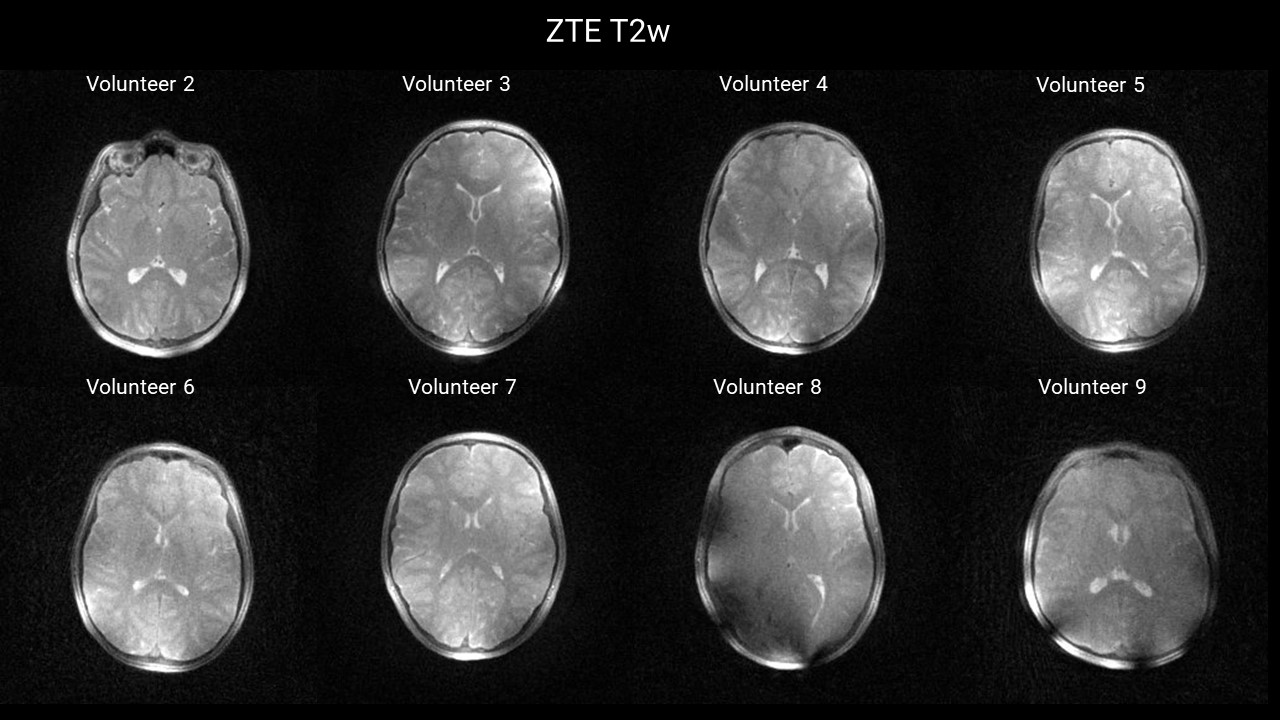
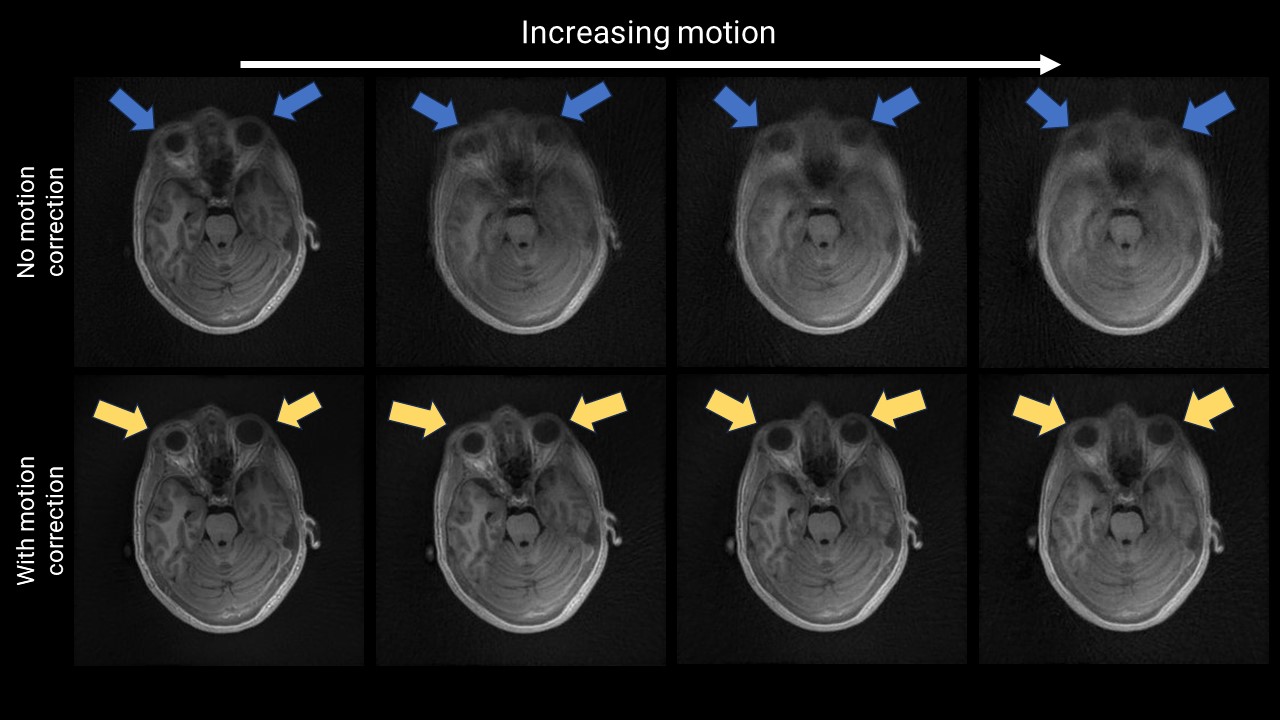
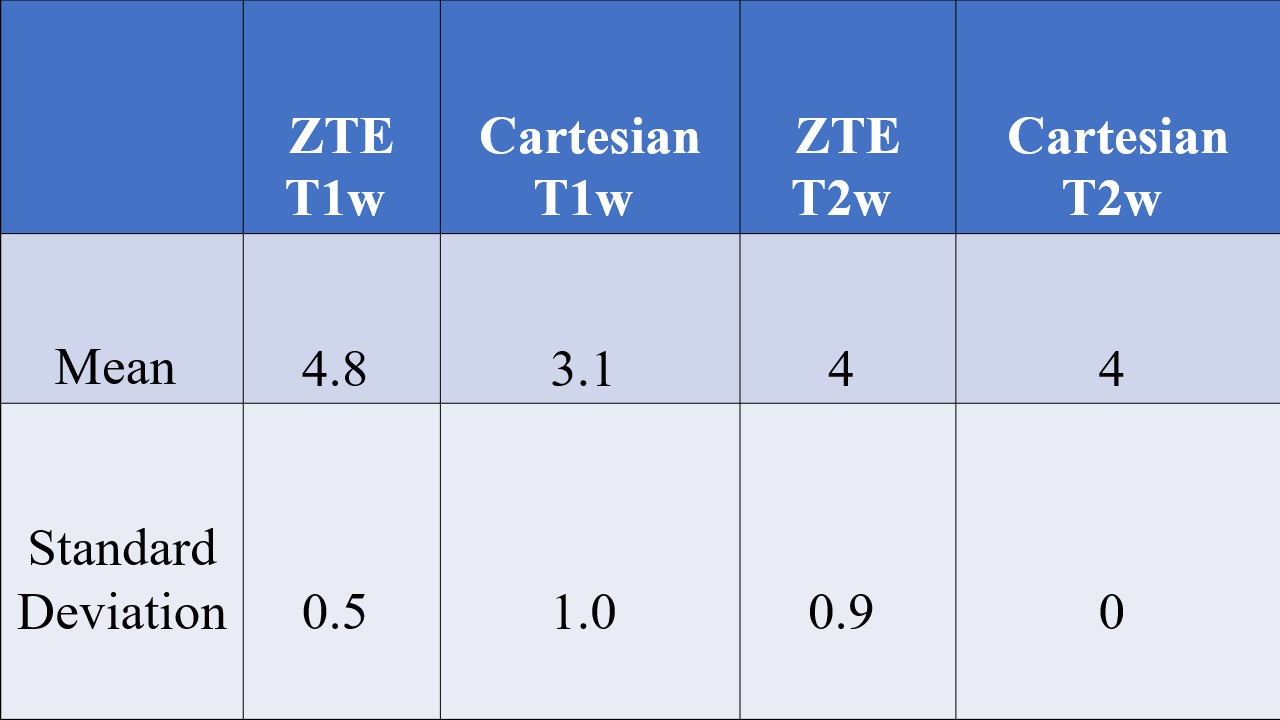
A summary of ZTE T1w and T2w images are shown for pediatric volunteers (Figs. 1 and 2). Results from the radiologist image review of overall image quality indicate at least equivalent and sometimes better image quality for the ZTE acquisitions versus the conventional Cartesian acquisition (Table1). These improvements were more evident on T1 imaging than T2 imaging. Note that Volunteer 1 had dental braces that introduced substantial artifacts in all imaging methods and this subject was excluded from the comparison. Results from the controlled angular motion studies (head wag method - generating anterior brain angular motion with a relatively anchored posterior skull, thus resulting in a back to front gradual gradient of linear motion) demonstrate the ability to recover fine structural details with relatively large amounts of subject motion (Fig. 3). Comparing pre and post motion corrected T1 axial reformats shows improved recovery of features such sulci and ventricles with motion correction. Blurring of small structures including middle cerebral arteries during motion was improved through motion correction with ZTE.Discussion
We present initial results in a pilot study using a ZTE-based silent and motion-robust neuroimaging protocol in pediatric volunteers. Results from controlled motion studies demonstrate robustness of the optimized ZTE acquisition and reconstruction to subject motion. The current imaging protocol did not include randomized acquisition order and there was evidence of systematically greater motion during the Cartesian T1w acquisition that will be addressed in future studies. The pediatric RF coil enabled rapid switching times but introduced substantial localized B1 inhomogeneities that impacted tissue visualization in some volunteers and future work will aim to optimize the coil performance.Conclusion
Segmented view order with T1w and T2w intermittent magnetization preparation pulses provided comparable image contrast to conventional Cartesian approaches in the pediatric population. HEALpix view order provided full coverage of k-space within 192 views for motion correction while maintaining acoustic noise levels well below conventional Cartesian based imaging protocols.Acknowledgements
NIH R43MH122028, NIH R01AG067078, NIH P50HD103556, NIH P50HD103556 and NIH S10OD025025. We thank Stephen Otto for project management and logistics related to this work.References
[1] Ljungberg, E.; Damestani, N. L.; Wood, T. C.; Lythgoe, D. J.; Zelaya, F.; Williams, S. C. R.; Solana, A. B.; Barker, G. J. & Wiesinger, F. (2021). Silent zero TE MR neuroimaging: Current state-of-the-art and future directions, Progress in Nuclear Magnetic Resonance Spectroscopy . PMID: 34078538
[2] Corum, C. A.; Kruger, S. & Magnotta, V. A. (2020). HEALPix View-order for 3D+time Radial Self-Navigated Motion-Corrected ZTE MRI, 2020 IEEE 17th International Symposium on Biomedical Imaging (ISBI) : 0409. http://arxiv.org/pdf/1910.10276v2
[3] Ying, L. & Sheng, J. (2007). Joint image reconstruction and sensitivity estimation in SENSE (JSENSE)., Magnetic resonance in medicine 57 : 1196-1202. PMID: 17534910
[4] Uecker, M.; Hohage, T.; Block, K. T. & Frahm, J. (2008). Image reconstruction by regularized nonlinear inversion--joint estimation of coil sensitivities and image content., Magnetic resonance in medicine 60 : 674-682. PMID: 18683237
[5] Pruessmann KP, Weiger M, Scheidegger MB, Boesiger P. SENSE: sensitivity encoding for fast MRI. 1999) Magn Reson Med. Nov;42(5):952-62. PMID: 10542355.
[6] Pruessmann KP, Weiger M, Börnert P, Boesiger P. (2001) Advances in sensitivity encoding with arbitrary k-space trajectories. Magn Reson Med.;46:638–651.
[7] Beatty, P. J.; Nishimura, D. G. & Pauly, J. M. (2005). Rapid gridding reconstruction with a minimal oversampling ratio, Medical Imaging, IEEE Transactions on 24 : 799 - 808. PMID: 15959939
[8] Pipe, J. G. & Menon, P. (1999). Sampling density compensation in MRI: rationale and an iterative numerical solution., Magn Reson Med 41 : 179-186. PMID: 10025627
[9] Ong, F. & Lustig, M. (2019). SigPy: a python package for high performance iterative reconstruction., Proc. Intl. Soc. Mag. Reson. Med. 27 : 4819. PMID: https://archive.ismrm.org/2019/4819.html
[10] Chen, Y.; Holmes, J. H.; Corum, C. A.; Magnotta, V. & Jacob, M. (2023). Motion compensated multi-contrast MRI using deep factor model, ISMRM.
[11] Chen, Y.; Holmes, J. H.; Corum, C.; Magnotta, V. & Jacob, M. (2022). DEEP FACTOR MODEL: A NOVEL APPROACH FOR MOTION COMPENSATEDMULTI-DIMENSIONAL MRI, https://doi.org/10.48550/arXiv.2304.00102
Figures