2531
OpenMAP-Di: Open Resource for Multiple Anatomical Region Parcellation of Diffusion MRI for Infantile Hypoxic-Ischemic Lesion Quantification1Radiology and Radiological Science, Johns Hopkins University School of Medicine, Baltimore, MD, United States, 2Applied Physics Laboratory, The Johns Hopkins University, Laurel, MD, United States, 3Johns Hopkins University School of Medicine, Baltimore, MD, United States, 4Applied Informatics, Graduate School of Science and Engineering, Hosei University, Tokyo, Japan, 5Neonatology, Toyama University Hospital, Toyama, Japan, 6University of Maryland School of Medicine, Baltimore, MD, United States, 7Neonatology, Johns Hopkins University School of Medicine, Baltimore, MD, United States, 8Pediatrics, Johns Hopkins University School of Medicine, Baltimore, MD, United States, 9General Internal Medicine, Johns Hopkins University School of Medicine, Baltimore, MD, United States, 10Gynecology & Obstetrics, Johns Hopkins University School of Medicine, Baltimore, MD, United States
Synopsis
Keywords: Neuro, Diffusion Tensor Imaging
Motivation: Diffusion MRI (dMRI) is promising for predicting disabilities due to neonatal hypoxic-ischemic encephalopathy (HIE), yet current automated image quantification methods are slow and unvalidated for HIE lesions.
Goal(s): Develop a rapid deep-learning model, OpenMAP-Di, to quantify dMRI with and without HIE injury to predict the short-term outcome (STO) score.
Approach: We utilized nnU-Net to develop OpenMAP-Di, enabling dMRI parcellation and quantification, and applied an elastic regression model to predict the STO score.
Results: OpenMAP-Di accurately parcellated and quantified infant brains across varying scanners, acquisition parameters, and HIE severity levels in three minutes, and can also predict STO.
Impact: The increased processing speed and robustness to technological and pathological variations offered by OpenMAP-Di promises timely and reliable future neurodevelopmental outcome assessments for individuals surviving HIE, while also offering researchers opportunities for extensive medical image analysis.
Introduction
Perinatal hypoxic-ischemic events can lead to encephalopathy (HIE) or perinatal arterial ischemic stroke (PAIS), which often lead to neurodevelopmental disabilities, but these outcomes are challenging to predict in infancy. Developing early interventions to improve HIE and PAIS outcomes necessitates a reliable method for early prediction of future neurological functions. Brain MRI, particularly dMRI is a valuable non-invasive tool that is sensitive to various types of brain damage, including cytotoxic and vasogenic edema, as well as Wallerian degeneration. Quantitative dMRI can predict short- and long-term neurological consequences1-4. While machine-learning combined with atlas-based image quantification has shown promise in outcome prediction5, existing methods are inaccurate for assessing areas affected by HIE and stroke lesions, and are computationally intensive. The Multi-Atlas Label-Fusion (MALF)6, 7 approach is recognized for its robustness against technological discrepancies and the presence of pathological lesions, but requires long processing times (several hours per image). This high computational demand poses substantial challenges for clinical implementation of MALF and for the simultaneous analysis of extensive image sets. This paper introduces a rapid, deep learning-based approach for neonatal dMRI parcellation, aiming to overcome these challenges.Methods
Training data The dMRI scans were sourced from two different datasets: the University of Hawaii – Johns Hopkins University (JHU) multi-atlas dataset, which includes healthy neonates (n = 10, median postmenstrual age [PMA] of 51 weeks at scans, range: 40–58 weeks), and the JHU-BIN study dataset, comprising neonates with HIE of varying severities (n = 16, median PMA of 40 weeks at scans, range: 36–84 weeks). Each neonate underwent a single dMRI scan that yielded multiple channels, including diffusion-weighted imaging (DWI), b0, and a fractional anisotropy (FA)-weighted orientation map.Test data The dMRI scans were obtained from two sources. For the HIE dataset, we utilized data from the JHU-BIN study, which was not included in the training of OpenMAP-Di (n = 209 with a median PMA of 40 weeks, ranging from 34 to 188 weeks). Additionally, we employed a dataset of healthy neonates obtained from the Baby Connectome Project (BCP, https://babyconnectomeproject.org/), n = 28 with a median chronological age of 11 weeks, ranging from 2 to 13 weeks.
Ground Truth (GT) Anatomical Labeling To establish ground truth parcellation labels, a MALF parcellation method was employed and subsequently manually refined by experts. The MALF pipeline segmented the entire brain into 169 distinct structures.8-11
Model Design and Evaluation We used nnU-Net12, based on the U-Net architecture for semantic segmentation and modeling. To evaluate OpenMAP-Di's performance, we applied volume and shape-based metrics such as Spearman’s rank-correlation, Dice Similarity Coefficient (DSC), recall, precision, and Intersection over Union (IoU), comparing OpenMAP-Di’s predictions to MALF’s results. We also evaluated the ability of the OpenMAP-Di to predict the short-term outcomes (STO) of neonates with HIE. The STO score, designed to evaluate short-term neurological function via assessment of feeding ability, ranges from 0 (normal) to 4 (death). FA and mean diffusivity (MD) values, extracted from the parcellation map, served as input variables for an elastic net model, which was used to predict the STO score. Four-fold cross-validation was then performed to establish the correlation between the measured and predicted STO scores.
Results
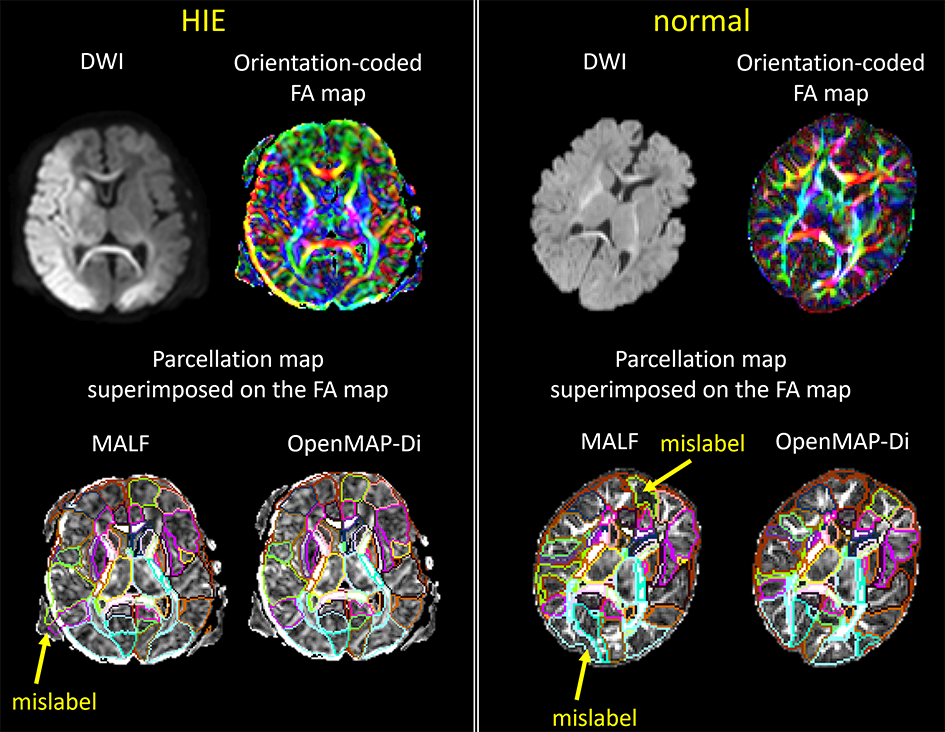
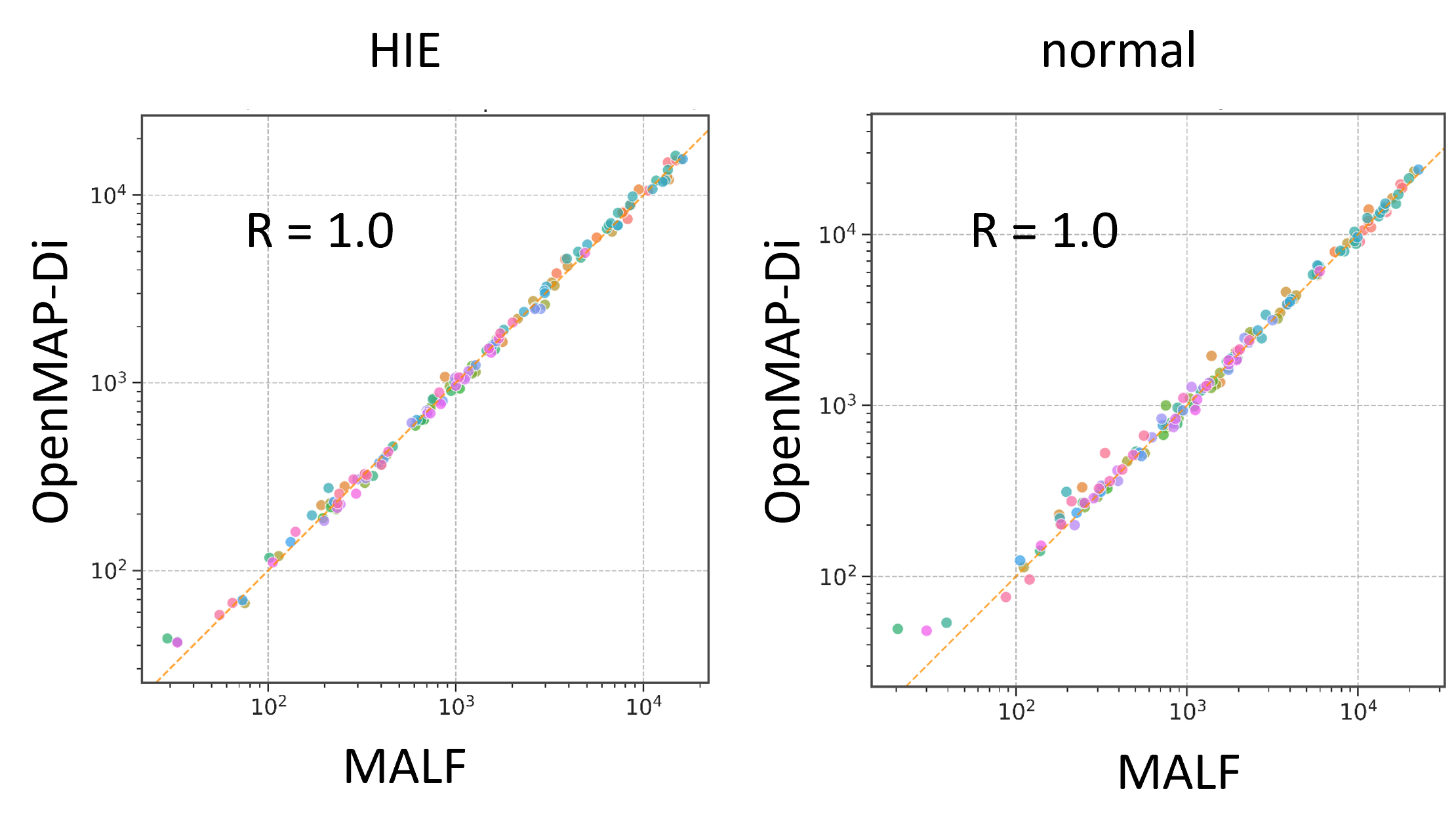
Figure 1 provides a side-by-side comparison of parcellation results from MALF and OpenMAP-Di, demonstrating OpenMAP-Di's proficiency in accurately parcellating images, regardless of the presence or absence of HIE lesions.Figure 2 demonstrates a strong correlation between the volume predictions made by MALF and OpenMAP-Di.
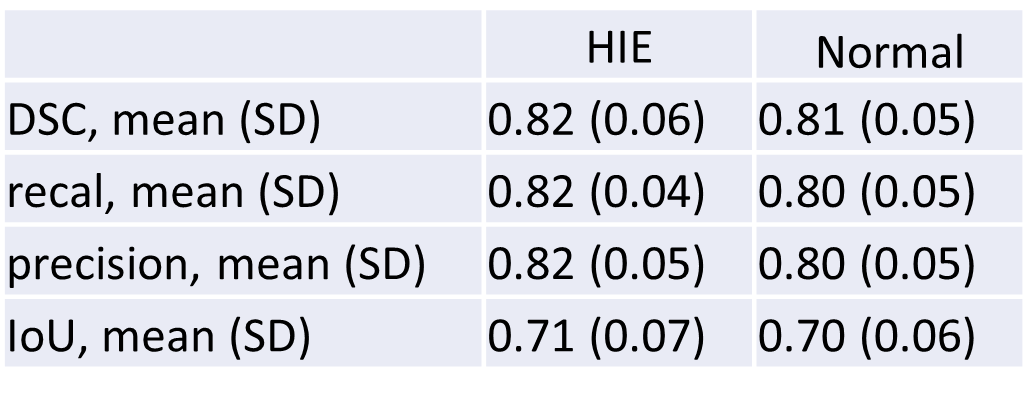
Figure 3 lists DSC, recall, precision, and IoU, calculated for the parcellation results of both MALF and OpenMAP-Di, revealing a high level of concordance between the two methods, regardless of the disease status. For images exhibiting low DSC values, the discrepancies can often be attributed to mislabeling issues in the MALF results, as illustrated in Figure 1.
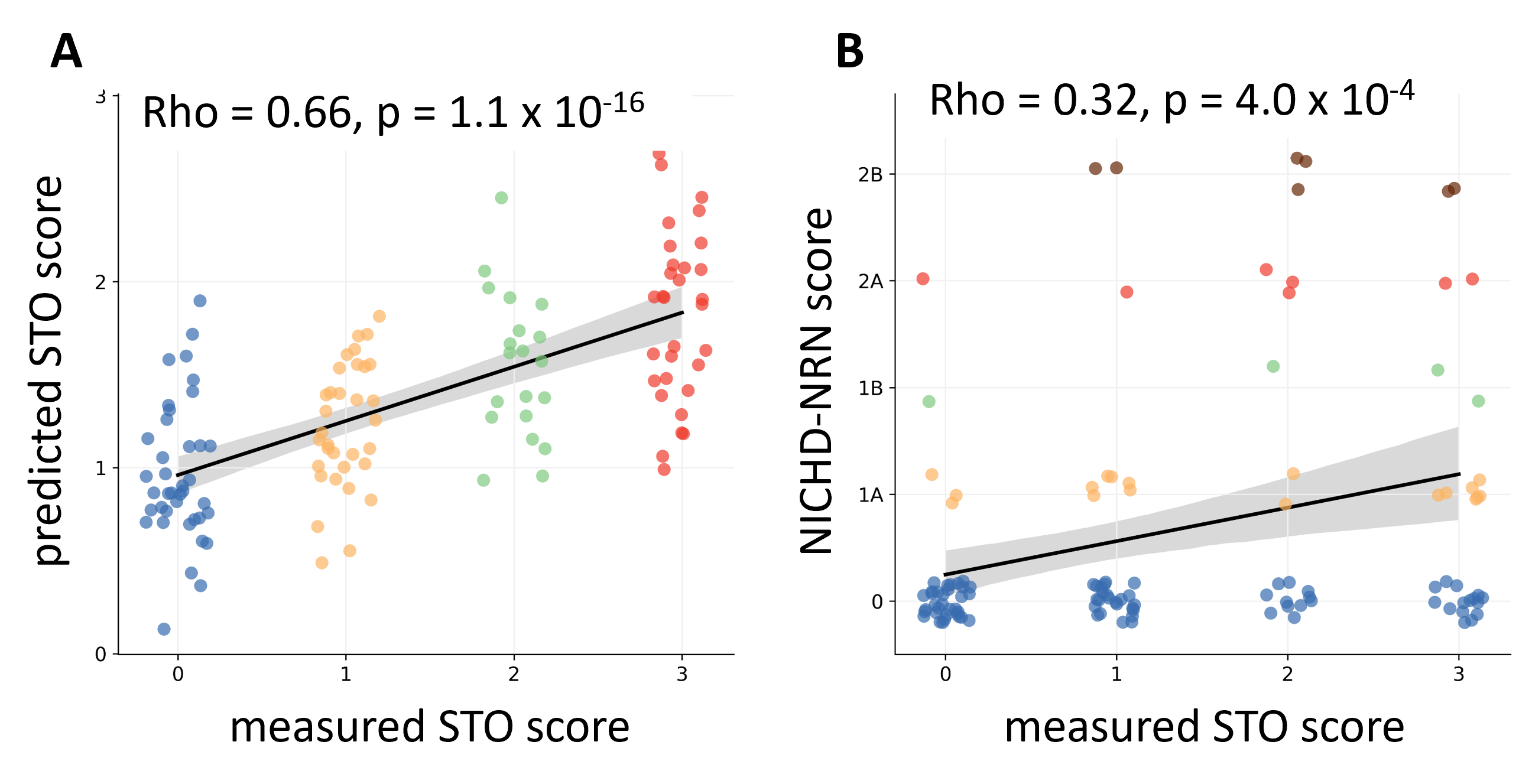
Figure 4 demonstrates how the actual measured STO is predicted by the different severity scales. The NICHD-NRN scores are from a scale for semi-quantifying HIE-related MRI findings. The correlation was significantly stronger (p=2.9×10-6, Z-test) between the predicted and actual STO scores (Figure 4A) than between the NICHD-NRN scores and the actual STO scores (Figure 4B), highlighting the superiority of OpenMAP-Di-based predictions.
Discussion
The accuracy of OpenMAP-Di is on par with that of MALF, yet it markedly improves processing speed. OpenMAP-Di exhibited superior parcellation performance on test datasets that encompassed images of healthy infants sourced from the BCP as well as images featuring a range of HIE-related lesions, underscoring its viability for clinical applications.Conclusion
We have developed OpenMAP-Di, a fast, robust, and accurate whole brain parcellation tool applicable to quantify the severity of HIE injury.Acknowledgements
We thank the families of the sick neonates included in this study for their willingness to participate. We also thank the nursing and ancillary staff at the Johns Hopkins Hospital NICU and core laboratory for their support in the collection of the samples. This work was supported by the National Institutes of Health R01HD065955, R01NS126549, RO1HD086058, and R01HD110091.References
1. Allen KA, Brandon DH. Hypoxic Ischemic Encephalopathy: Pathophysiology and Experimental Treatments. Newborn Infant Nurs Rev. 2011;11(3):125-33. Epub 2011/09/20. doi: 10.1053/j.nainr.2011.07.004. PubMed PMID: 21927583; PubMed Central PMCID: PMCPMC3171747.
2. Greco P, Nencini G, Piva I, Scioscia M, Volta CA, Spadaro S, Neri M, Bonaccorsi G, Greco F, Cocco I, Sorrentino F, D’Antonio F, Nappi L. Pathophysiology of hypoxic–ischemic encephalopathy: a review of the past and a view on the future. Acta Neurologica Belgica. 2020;120(2):277-88. doi: 10.1007/s13760-020-01308-3.
3. Onda K, Chavez-Valdez R, Graham EM, Everett AD, Northington FJ, Oishi K. Quantification of Diffusion Magnetic Resonance Imaging for Prognostic Prediction of Neonatal Hypoxic-Ischemic Encephalopathy. Developmental Neuroscience. 2023:1-14. doi: 10.1159/000530938.
4. Cauley KA, Filippi CG. Apparent diffusion coefficient histogram analysis of neonatal hypoxic–ischemic encephalopathy. Pediatric Radiology. 2014;44(6):738-46. doi: 10.1007/s00247-013-2864-1.
5. Onda K, Catenaccio E, Chotiyanonta J, Chavez-Valdez R, Meoded A, Soares BP, Tekes A, Spahic H, Miller SC, Parker S-J, Parkinson C, Vaidya DM, Graham EM, Stafstrom CE, Everett AD, Northington FJ, Oishi K. Development of a composite diffusion tensor imaging score correlating with short-term neurological status in neonatal hypoxic–ischemic encephalopathy. Frontiers in Neuroscience. 2022;16. doi: 10.3389/fnins.2022.931360.
6. Otsuka Y, Chang L, Kawasaki Y, Wu D, Ceritoglu C, Oishi K, Ernst T, Miller M, Mori S, Oishi K. A Multi-Atlas Label Fusion Tool for Neonatal Brain MRI Parcellation and Quantification. J Neuroimaging. 2019. Epub 2019/05/01. doi: 10.1111/jon.12623. PubMed PMID: 31037800.
7. Tang X, Yoshida S, Hsu J, Huisman TA, Faria AV, Oishi K, Kutten K, Poretti A, Li Y, Miller MI, Mori S. Multi-contrast multi-atlas parcellation of diffusion tensor imaging of the human brain. PLoS One. 2014;9(5):e96985. Epub 2014/05/09. doi: 10.1371/journal.pone.0096985. PubMed PMID: 24809486; PubMed Central PMCID: PMC4014574.
8. Djamanakova A, Tang X, Li X, Faria AV, Ceritoglu C, Oishi K, Hillis AE, Albert M, Lyketsos C, Miller MI. Tools for multiple granularity analysis of brain MRI data for individualized image analysis. Neuroimage. 2014;101:168-76.
9. Liang Z, He X, Ceritoglu C, Tang X, Li Y, Kutten KS, Oishi K, Miller MI, Mori S, Faria AV. Evaluation of cross-protocol stability of a fully automated brain multi-atlas parcellation tool. PloS one. 2015;10(7):e0133533.
10. Wu D, Ma T, Ceritoglu C, Li Y, Chotiyanonta J, Hou Z, Hsu J, Xu X, Brown T, Miller MI. Resource atlases for multi-atlas brain segmentations with multiple ontology levels based on T1-weighted MRI. Neuroimage. 2016;125:120-30.
11. Mori S, Wu D, Ceritoglu C, Li Y, Kolasny A, Vaillant MA, Faria AV, Oishi K, Miller MI. MRICloud: delivering high-throughput MRI neuroinformatics as cloud-based software as a service. Computing in Science & Engineering. 2016;18(5):21-35.
12. Isensee F, Jaeger PF, Kohl SAA, Petersen J, Maier-Hein KH. nnU-Net: a self-configuring method for deep learning-based biomedical image segmentation. Nat Methods. 2021;18(2):203-11. Epub 2020/12/09. doi: 10.1038/s41592-020-01008-z. PubMed PMID: 33288961.
Figures