2529
Influence of Maternal Position on Fetal Organ Oxygenation using Low Field MR1Centre for the Developing Brain, School of Biomedical Engineering and Imaging Sciences, King's College London, London, United Kingdom, 2Biomedical Engineering Department, School of Biomedical Engineering and Imaging Sciences, King's College London, London, United Kingdom, 3Department of Women and Children’s Health, St Thomas’ Hospital, King's College London, London, United Kingdom, 4Smart Imaging Lab, Radiological Institute, University Hospital Erlangen, Erlangen, Germany
Synopsis
Keywords: Fetal, Fetus
Motivation: Maternal supine sleeping position in the third trimester has been linked to decreased uterine blood flow and increases in stillbirth.
Goal(s): To investigate the impact of maternal position on fetal and placental T2* values by taking advantage of the increased dynamic T2* range at low field strengths
Approach: We acquired dynamic whole uterus multi-echo gradient echo sequences at 0.55T with the subject in both left lateral and supine positions and compare the T2* placental and fetal body organ values organs in 91 subjects.
Results: Significant differences in mean T2* values were observed between both positions in the placenta and 7 fetal body organs.
Impact: Maternal position significantly impacts mean placental and fetal body T2* values. In addition, future quantitative fetal T2* studies should consider maternal position in their study design.
Introduction
During the late stages of pregnancy, women are advised to sleep on their side, as studies linked sleeping supine to reduced uterine blood flow, increased risk of stillbirths and reduced birth weight1–3. Magnetic resonance imaging (MRI) demonstrated a reduction in internal iliac artery flow4,5 as well as an increase in venous blood due to the compression of the inferior vena cava6.The increased availability of clinical low field (0.55T) scanners provides additional opportunities to investigate the effects of maternal position on fetal blood flow and tissue oxygenation: The wide bore scanner allows women of all sizes and in late gestation to comfortably lie in both supine and left lateral (LL) position, the B0 field is more homogeneous than at higher field strengths, and no shimming is required, key for functional sequences. Most importantly, low field strengths have a larger dynamic range of T2* values, allowing to observe subtle differences not discernible at higher field strengths.
While a physiological decrease in placental T2* values occurs throughout gestation, reduced placental T2* values have been observed in disorders such as pre-eclampsia7, fetal growth restriction8, and congenital heart disease9. However, the effect on fetal body organs has not yet been studied. We aim to determine how fetal body organ and placental T2* values are influenced by the maternal position.
Methods
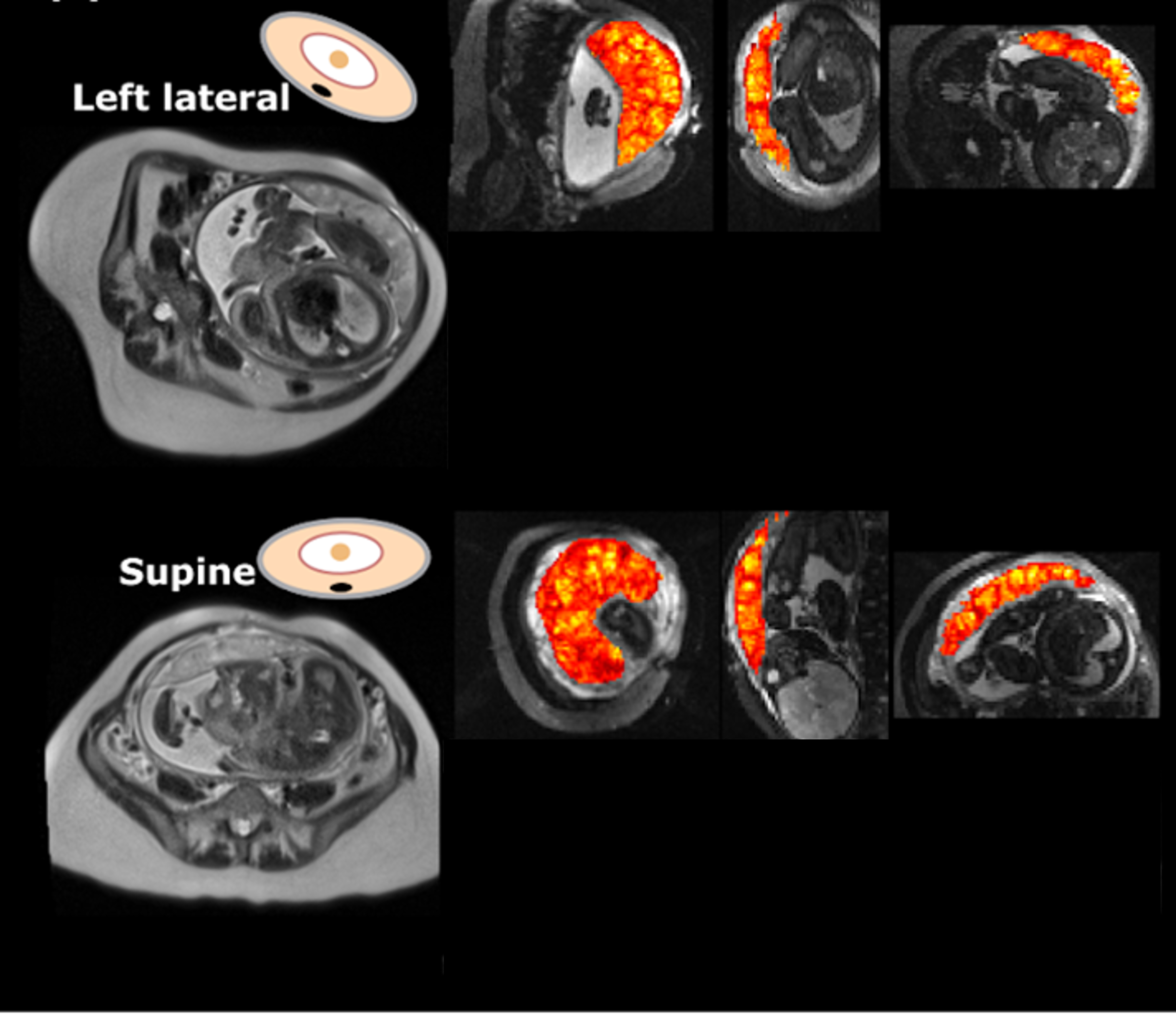
Fetal MRI was acquired prospectively as part of an ethically approved study (19/LO/0852) at St Thomas’ Hospital, in London, UK on a clinical 0.55T scanner (MAGNETOM Free.Max, Siemens Healthcare) using a 6-element blanket coil and a 9-element spine coil. The first 6 minutes of the scan were acquired in maternal LL position, supported by a pregnancy pillow and/or wedges, before switching the maternal position to supine, providing padding in the lower back as required (Figure 1, left).Dynamic multi-echo gradient echo singe-shot EPI scans were acquired in both positions, the LL sequence at the beginning and the supine sequence at the end of the hour-long scanning session. The parameters include resolution= 3x3x3mm2, FOV=400x400mm2, GRAPPA=22, TE=[42, 107, 172]ms; TR=10,420ms, 20 dynamics. In addition, whole uterus 2D Turbo Spin Echo Imaging scans were acquired in both positions (FOV=450x450, resolution=1.5x1.5x4.5mm, TR=2500ms, TE=106ms).
Multichannel deformable slice-to-volume reconstruction10 was performed, T2* maps calculated and the fetal lungs, liver, stomach, spleen, thymus, adrenal glands, bladder, gallbladder, kidney parenchyma and kidney pelvis segmented automatically11. The placenta was outlined automatically on the first dynamic9 directly without 3D reconstruction using nnUNet12. Mean T2* values were calculated for all organs.
To compare the T2* values in LL and Supine, a paired T-test was used in python, with p-values<0.05 considered significant, on the entire cohort as well as split in cases less than 30weeks, and greater than 30 weeks.
Results
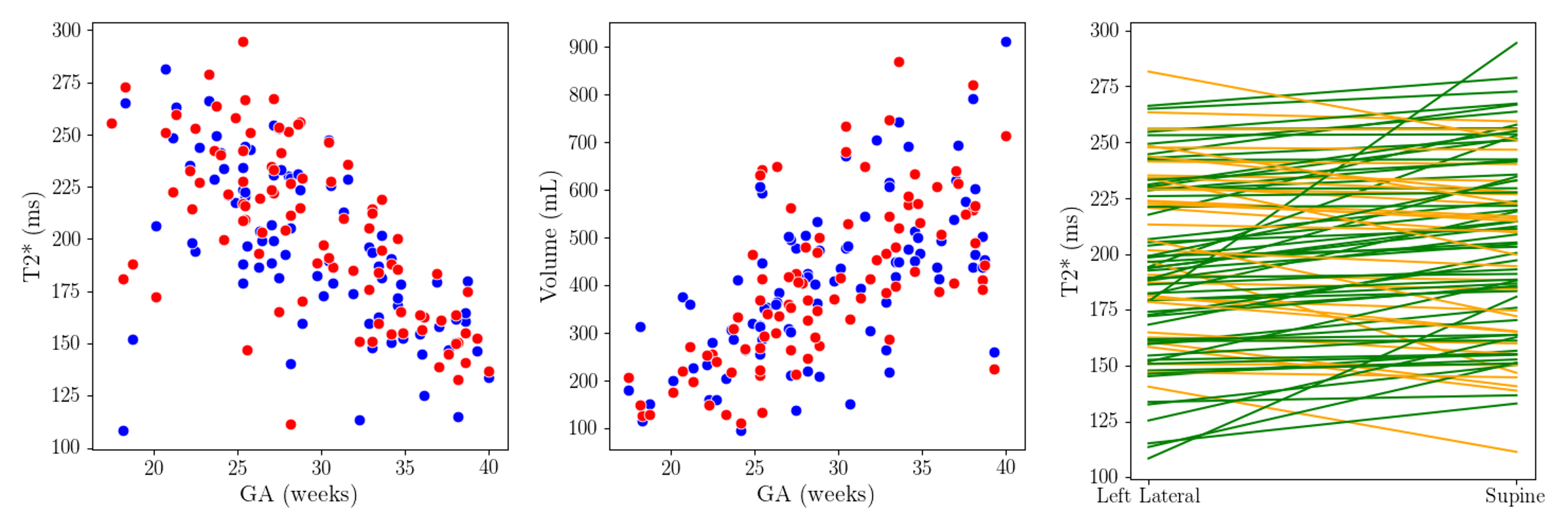
91 datasets (GA 22-40 weeks, 71 healthy and 20 with pathologies) with a dynamic multi-echo multi-gradient in both positions were available. All subjects were analysed together, as we were interested in the subject-specific changes of T2* values rather than across groups. For the fetal body organs, each reconstruction was visually reviewed, resulting in 58 cases with good quality reconstructions in both positions. Of the 33 cases excluded, 14 were <24 weeks. All placental datasets were included.Example T2* placenta maps can be found in Figure 1 (right). Placental volume increased and T2* values decreased over gestation (Figure 3).Mean placental T2* values were higher in the LL position compared to supine across all gestational ages (p<0.01).
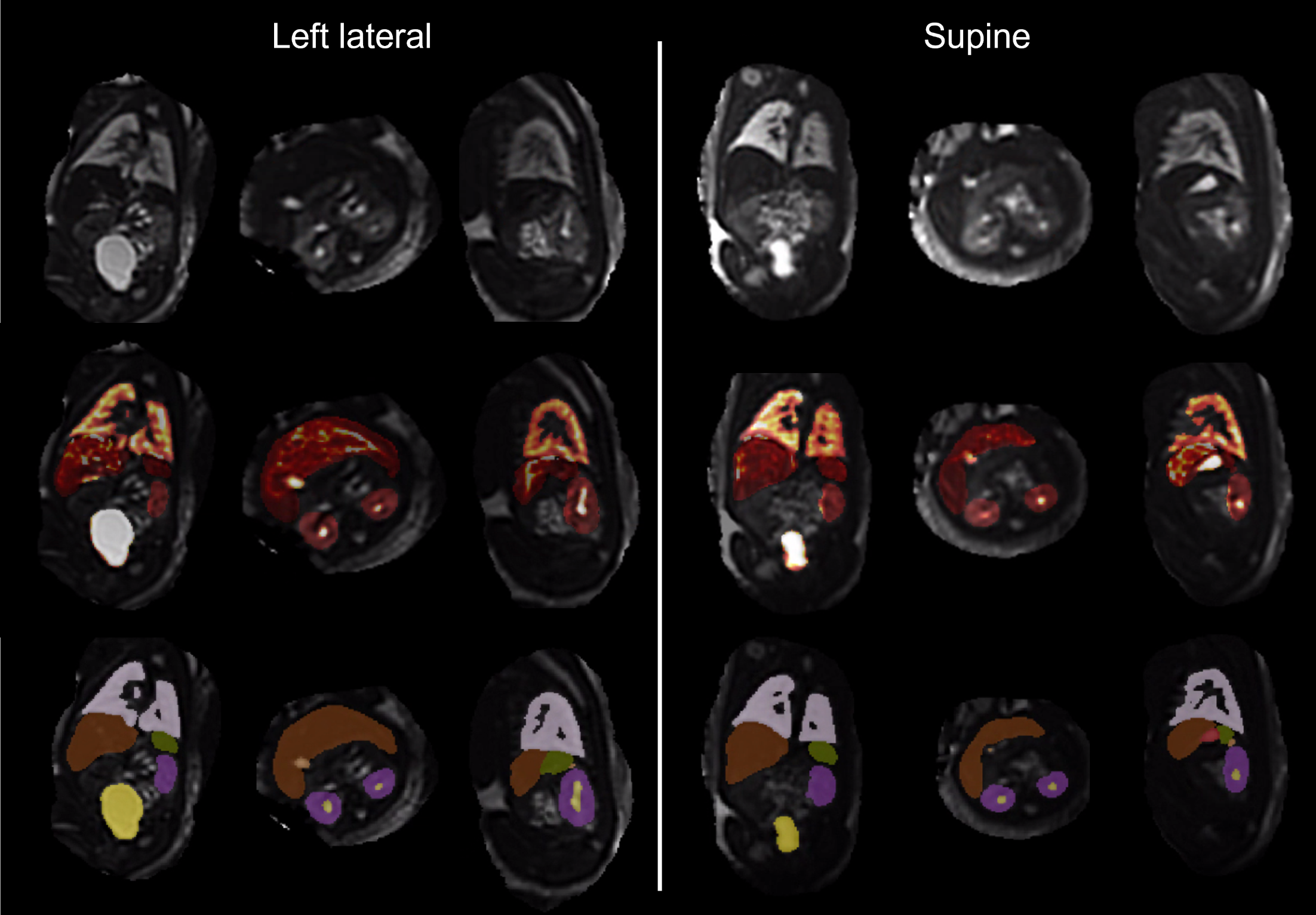
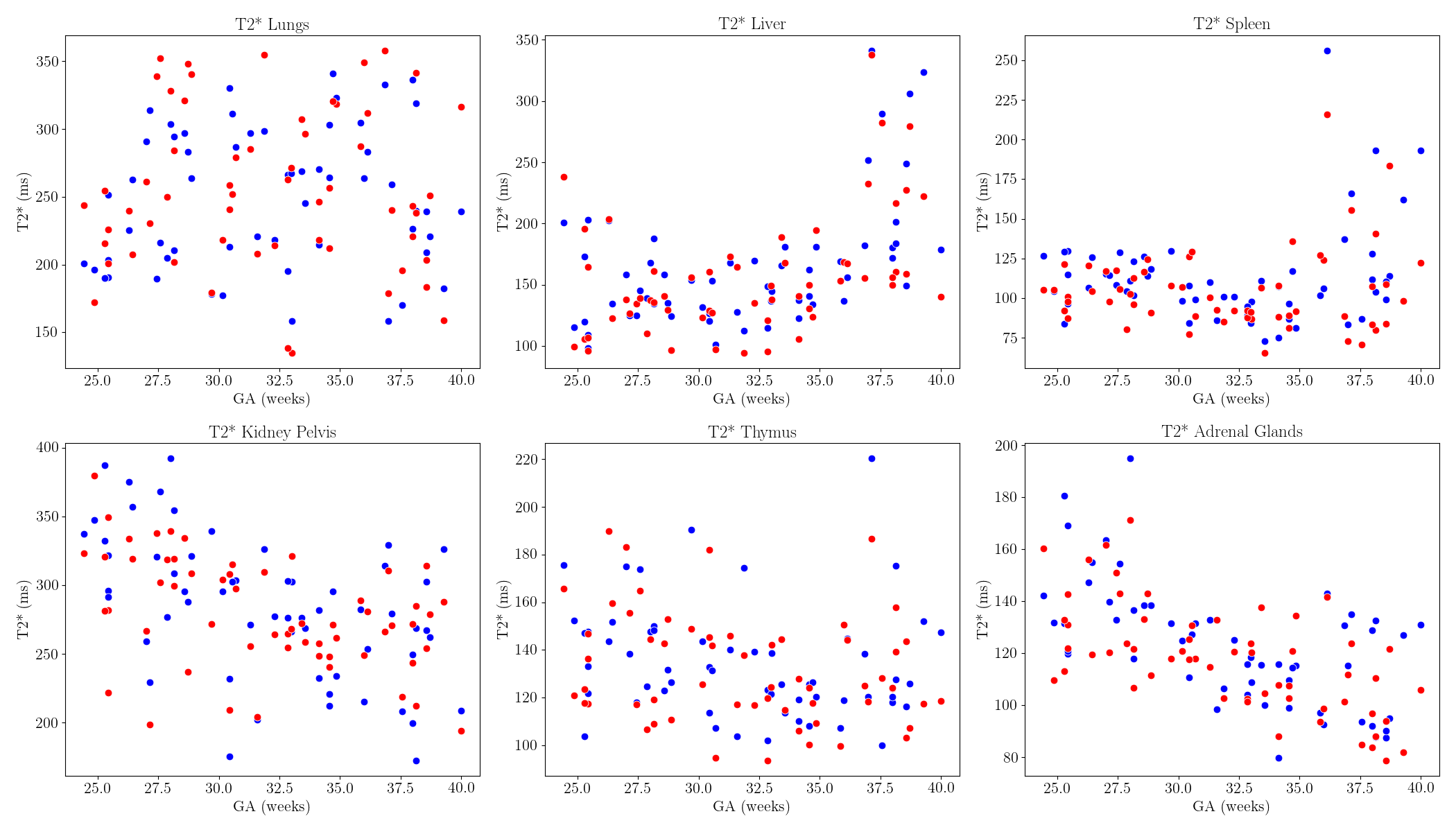
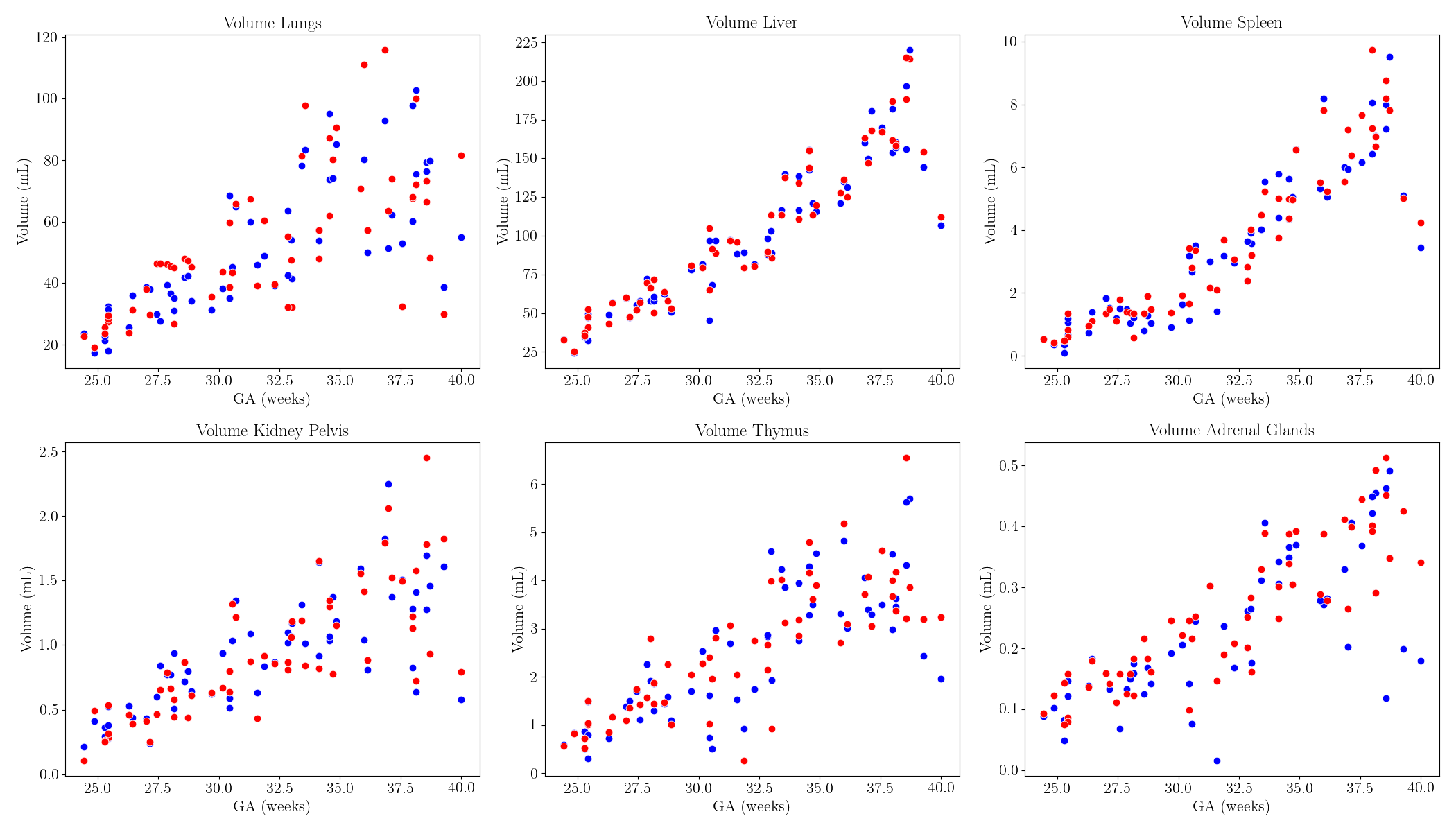
Example fetal body organ reconstructions, label maps, and T2* maps can be found in Figure 2. No difference in T2* values was seen in the lungs, bladder, and thymus (Figure 4). Mean T2* values of the liver (p<0.01), stomach (p<0.01), spleen (p<0.01), kidney parenchyma (p=0.02), and adrenal glands (p<0.01) were higher in the LL position when compared to the supine for all gestational ages. Mean T2* values of the kidney pelvis (p<0.01) and gallbladder (p=0.04) were found to be higher in the LL position in fetuses <30 weeks. No significant volume differences were found (Figure 5).
Discussion & Conclusion
Several fetal body organ T2* values are lower in the supine position than the LL. However, the mean placental T2* values in the supine position were higher than in the LL position, contradicting literature values4,5. Further investigation into the individual changes in T2* values (Figure 3) will be explored and correlated with important maternal factors such as BMI and chronic hypertension. The presented investigation allows to study the impact of maternal position on the oxygenation of the fetus and placenta (albeit indirectly via T2*), more investigation is needed to understand the underlying hemodynamics.Acknowledgements
The authors thank all the participating families as well as the midwives and radiographers involved in this study. This work was supported by the NIH (Human Placenta Project—grant 1U01HD087202‐01), Wellcome Trust Sir Henry Wellcome Fellowship (201374/Z/16/Z and /B), UKRI FLF (MR/T018119/1), DFG Heisenberg funding [502024488], EPSRC (EP/V034537/1), the NIHR Clinical Research Facility (CRF) at Guy's and St Thomas' and by core funding from the Wellcome/EPSRC Centre for Medical Engineering [WT203148/Z/16/Z] and by the National Institute for Health Research (NIHR) Clinical Research Facility based at Guy’s and St Thomas’ NHS Foundation Trust and King’s College London. The views expressed are those of the authors and not necessarily those of the NHS or the NIHR or the Department of Health and Social Care.References
1. Anderson, N. H. et al. Association of Supine Going-to-Sleep Position in Late Pregnancy With Reduced Birth Weight. JAMA Netw. Open 2, e1912614 (2019).
2. Cronin, R. S. et al. An Individual Participant Data Meta-analysis of Maternal Going-to-Sleep Position, Interactions with Fetal Vulnerability, and the Risk of Late Stillbirth. EClinicalMedicine 10, 49–57 (2019).
3. Stone, P. R. et al. Effect of maternal position on fetal behavioural state and heart rate variability in healthy late gestation pregnancy. J. Physiol. 595, 1213–1221 (2017).
4. Couper, S. et al. The effects of maternal position, in late gestation pregnancy, on placental blood flow and oxygenation: an MRI study. J. Physiol. 599, 1901–1915 (2021).
5. Jani, D. et al. The effect of maternal position on placental blood flow and fetoplacental oxygenation in late gestation fetal growth restriction: a magnetic resonance imaging study. J. Physiol. n/a,. 6. Humphries, A., Mirjalili, S. A., Tarr, G. P., Thompson, J. M. D. & Stone, P. The effect of supine positioning on maternal hemodynamics during late pregnancy. J. Matern.-Fetal Neonatal Med. Off. J. Eur. Assoc. Perinat. Med. Fed. Asia Ocean. Perinat. Soc. Int. Soc. Perinat. Obstet. 32, 3923–3930 (2019). 7. Ho, A. et al. Placental magnetic resonance imaging in chronic hypertension: A case-control study. Placenta 104, 138–145 (2021).
8. Sinding, M. et al. Placental magnetic resonance imaging T2* measurements in normal pregnancies and in those complicated by fetal growth restriction. Ultrasound Obstet. Gynecol. 47, 748–754 (2016).
9. Steinweg, J. K. et al. T2* placental MRI in pregnancies complicated with fetal congenital heart disease. Placenta 108, 23–31 (2021).
10. Uus, A. et al. Deformable Slice-to-Volume Registration for Motion Correction of Fetal Body and Placenta MRI. IEEE Trans. Med. Imaging 39, 2750–2759 (2020).
11. Payette, K. et al. An Automated Pipeline for Quantitative T2* Fetal Body MRI and Segmentation at Low Field. in Medical Image Computing and Computer Assisted Intervention – MICCAI 2023 (eds. Greenspan, H. et al.) 358–367 (Springer Nature Switzerland, 2023). doi:10.1007/978-3-031-43990-2_34.
12. Isensee, F., Jaeger, P. F., Kohl, S. A. A., Petersen, J. & Maier-Hein, K. H. nnU-Net: a self-configuring method for deep learning-based biomedical image segmentation. Nat. Methods 18, 203–211 (2021).
Figures