2528
Development of Quantitative Magnetization Transfer Imaging for the Human Cervical Spinal Cord at 3 Tesla1Neuroimaging Innovation Center, Barrow Neurological Institute, Phoenix, AZ, United States, 2Translational Neuroscience, Barrow Neurological Institute, Phoenix, AZ, United States
Synopsis
Keywords: Spinal Cord, Relaxometry, Quantitative Magnetization Transfer, C-spine
Motivation: We proposed to use a method known as selective inversion recovery (SIR), which allows one to perform the entire QMT (quantitative magnetization transfer) experiment from a conventional inversion recovery sequence.
Goal(s): To translate the SIR-QMT method to the spinal cord at 3T with optimized sampling schemes to yield high-resolution cervical spinal cord PSR (macromolecular pool-size-ratios) maps within clinically relevant scan times.
Approach: SIR-QMT was conducted on two healthy volunteers to calculate PSR and R1f.
Results: These results suggest that QMT imaging can be performed in the human cervical spinal cord at 3T.
Impact: The work has important clinical indication to study de/remyelination and nerve injuries/repairs in spinal cord disorders.
INTRODUCTION
Quantitative magnetization transfer (QMT) imaging has been used to quantify myelin content changes associated with de/remyelination in brain of persons with multiple sclerosis (pwMS). Spinal cord demyelination may be more closely linked with clinical deficits1; however, few studies have applied QMT to the spinal cord due to the challenges associated with spinal cord imaging (high-resolution demands, susceptibility artifacts, motion). One method to overcome these issues is to fit data acquired following a single off-resonance saturation to a constrained model of the MT effect. Although this approach has shown the ability to detect demyelination in focal spinal cord lesions1, it is unclear if the model constraints are valid in certain pathological scenarios. Furthermore, the method requires independent estimate of T1, B0, and B1, resulting in a method that is challenging to implement in clinical scenarios. Herein, we propose an alternative method known as selective inversion recovery (SIR), which allows one to perform the entire QMT experiment from a conventional inversion recovery sequence. Previous work in the brain has indicated that SIR-derived macromolecular pool-size-ratios (PSR) relate to myelin content in the brain2 and disability3. Herein, we translate this method to the spinal cord at 3T for the first time and combine with optimized sampling schemes and compressed SENSING under sampling4 to yield high-resolution cervical spinal cord PSR maps within clinically relevant scan times.METHODS
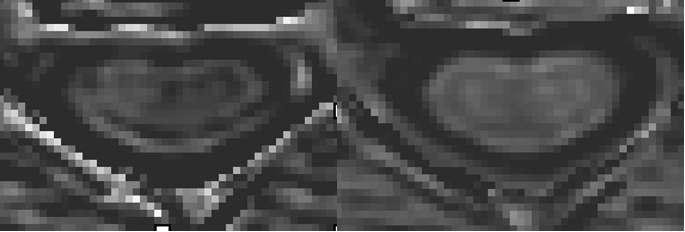
Two healthy volunteers (22–30 y.o.) were imaged using a 3-T Philips MR scanner. A SIR imaging sequence with a turbo spin echo (SIR-TSE) readout was used to collect QMT data in an axial volume from C2 to C5 using an optimized approach5: inversion time ti = [15, 15, 278, 1007] ms, delay time td = [684, 4171, 2730, 10], resolution = 1×1×5 mm3, field-of-view = 150×150×90 mm3, and CS-SENSE factor = 4. Regions-of-interest (ROIs) were conservatively defined in the white matter (wm) and in gray matter (gm) to minimize partial-voluming (Fig. 1). Data from each ROI were fit to a biexponential model derived from a two-pool model of the MT effect6. This yielded the macromolecular to free proton pool size ratio (PSR) and the R1 of the free pool (R1f).RESULTS
Sample SIR-TSE images are given in Fig. 1. Note the contrast between white and grey matter and the absence of flow- and susceptibly related artifacts due to the TSE readout. Sample PSR and R1f maps are shown in Fig. 2, and Mean QMT parameters were tabulated across all slices and volunteers (Table 1). PSR values were slightly higher in white matter relative to grey matter. This agrees with previously reported PSR values from the human cervical spinal cord3,4.DISCUSSION
Consistent with previous T1 measurements in the cervical spinal cord at 3T7, R1f values were higher in white matter relative to gray matter. These preliminary results suggest that QMT imaging can be performed in the human cervical spinal cord at 3T, although additional work is needed to minimize the impact of motion and partial volume averaging with surrounding CSF. Future work will include systematically evaluation these effects and applying this method in a cohort in pwMS.Acknowledgements
The study was supported by the National Multiple Sclerosis Society (RG-2111-38720), DOD/PRMRP (PR211292), and Philips Healthcare.
References
1. Dortch RD, Moore J, Li K, et al. Quantitative magnetizationtransfer imaging of human brain at 7 T. Neuroimage. 2013; 64:640-649.
2. Zackowski K, Smith S, Reich D, et al. Sensorimotor dysfunction in multiple sclerosis and column-specific magnetization transfer-imaging abnormalities in the spinal cord. 2009; 132(Pt 5):1200-1209.
3. Smith S, Golay X, Fatemi A, et al. Quantitative magnetization transfer characteristics of the human cervical spinal cord in vivo: application to adrenomyeloneuropathy. Magn Reson Med. 2009; 61(1):22-27.
4. Wang P, Sisco N, Yoo W, et al. Rapid whole-brain myelin imaging with selective inversion recovery and compressed SENSE. Magn Reson Med. 2023; 89(3):1041-1054.
5. Dortch R, Bagnato F, Gochberg D, et al. Optimization of selective inversion recovery magnetization transfer imaging for macromolecular content mapping in the human brain. Magn Reson Med. 2018;80:1824-1835.
6. Li K, Zu Z, Xu J, et al. Optimized inversion recovery sequences for quantitative T1 and magnetization transfer imaging. Magn Reson Med. 2010;64:491-500.
7. Smith S, Edden R, Farrell J et al. Measurement of T1 and T2 in the cervical spinal cord at 3 tesla. Magn Reson Med. 2008; 60(1):213-219.
Figures