2523
Spinal cord injury-induced changes in thoracolumbar microarchitecture: a semi-automated DTI pipeline for improved clinical translation1School of Medicine, Faculty of Health and Medical Sciences, The University of Adelaide, Adelaide, Australia, 2Neil Sachse Centre for Spinal Cord Research, Lifelong Health Theme, South Australian Health and Medical Research Institute, Adelaide, Australia, 3Preclinical, Imaging and Research Laboratories, South Australian Health and Medical Research Institute, Adelaide, Australia, 4Clinical & Research Imaging Centre, South Australian Health and Medical Research Institute, Adelaide, Australia, 5National Imaging Facility, South Australian Node, Adelaide, Australia, 6Siemens Healthcare GmbH, Erlangen, Germany, 7Australian Cancer Research Foundation Molecular Theranostics Laboratory, Centenary Institute, Sydney, Australia, 8Centre for Neuroscience Studies, Queens University, Kingston, ON, Canada, 9Department of Biomedical and Molecular Sciences, Queens University, Kingston, ON, Canada, 10Department of Physics, Queens University, Kingston, ON, Canada
Synopsis
Keywords: Spinal Cord, Microstructure, Diffusion Tensor Imaging
Motivation: While diffusion tensor imaging (DTI) is sensitive to spinal cord injury (SCI)-induced microstructural changes, manual pre-processing of thoracolumbar spinal cord (TL-SC) data precludes its clinical translation.
Goal(s): We aimed to optimise a semi-automatic TL-SC DTI protocol to detect SCI-induced microarchitectural changes.
Approach: TL-SC DTI data from two participants with diagnosed SCI and six healthy volunteers were pre-processed to equate the TL-SC microarchitecture and then compared to semi-automated analysis.
Results: Our optimised TL-SC DTI acquisition and semi-automatic analysis pipeline is sensitive to SCI-induced microstructural changes and may provide a more clinically viable method for TL-SC DTI analysis.
Impact: This study assessed and validated our newly developed thoracolumbar spinal cord (TL-SC) diffusion tensor imaging (DTI) pipeline in detecting spinal cord injury (SCI)-induced microstructural changes and offers an alternative semi-automatic pre-processing method for improved clinical translation.
Background
Diffusion tensor imaging (DTI) is a quantitative MRI (qMRI) technique that uses the directional functionality of water molecules within biological tissue as an indirect measure of axonal microarchitecture. The longitudinal layout of spinal cord white matter causes predominant water diffusion along axonal fibres. DTI indices (fractional anisotropy (FA), mean diffusivity (MD), axial diffusivity (AD), and radial diffusivity (RD)) are sensitive to the disruption of this fibre architecture, including spinal cord injury (SCI), providing information about injury-induced microstructural integrity changes (1). DTI may offer an alternative to the limitation of conventional MRI by providing additional microstructural information for improved SCI diagnosis and prognosis. Despite the routine use of DTI in clinical brain pathology, clinical translation has yet to be seen in the spinal cord. The spinal cord's small cross-sectional area and long length require a higher spatial resolution during image acquisition. Similarly, motion-related artefacts resulting from the cardiac cycle add further image pre-processing complexity (2). Several advancements in image acquisition and pre-processing have successfully mitigated these issues in the cervicothoracic spinal cord (3,4). However, progress in thoracolumbar spinal cord (TL-SC) DTI is relatively nascent. Imaging quality in the TL-SC is further hampered by added physiological motion from respiration and intestinal peristalsis. Current pre-processing techniques, including automatic vertebral labelling, were developed for the cervicothoracic spinal cord (5). Consequently, manual pre-processing of TL-SC DTI data is employed due to the lack of available automated techniques. For this study, we developed an optimised DTI acquisition and analysis pipeline in the TL-SC. We aimed to evaluate the feasibility of TL-SC DTI in detecting SCI-induced microstructural integrity changes and to determine if these changes can be detected via our semi-automated pipeline.Methods
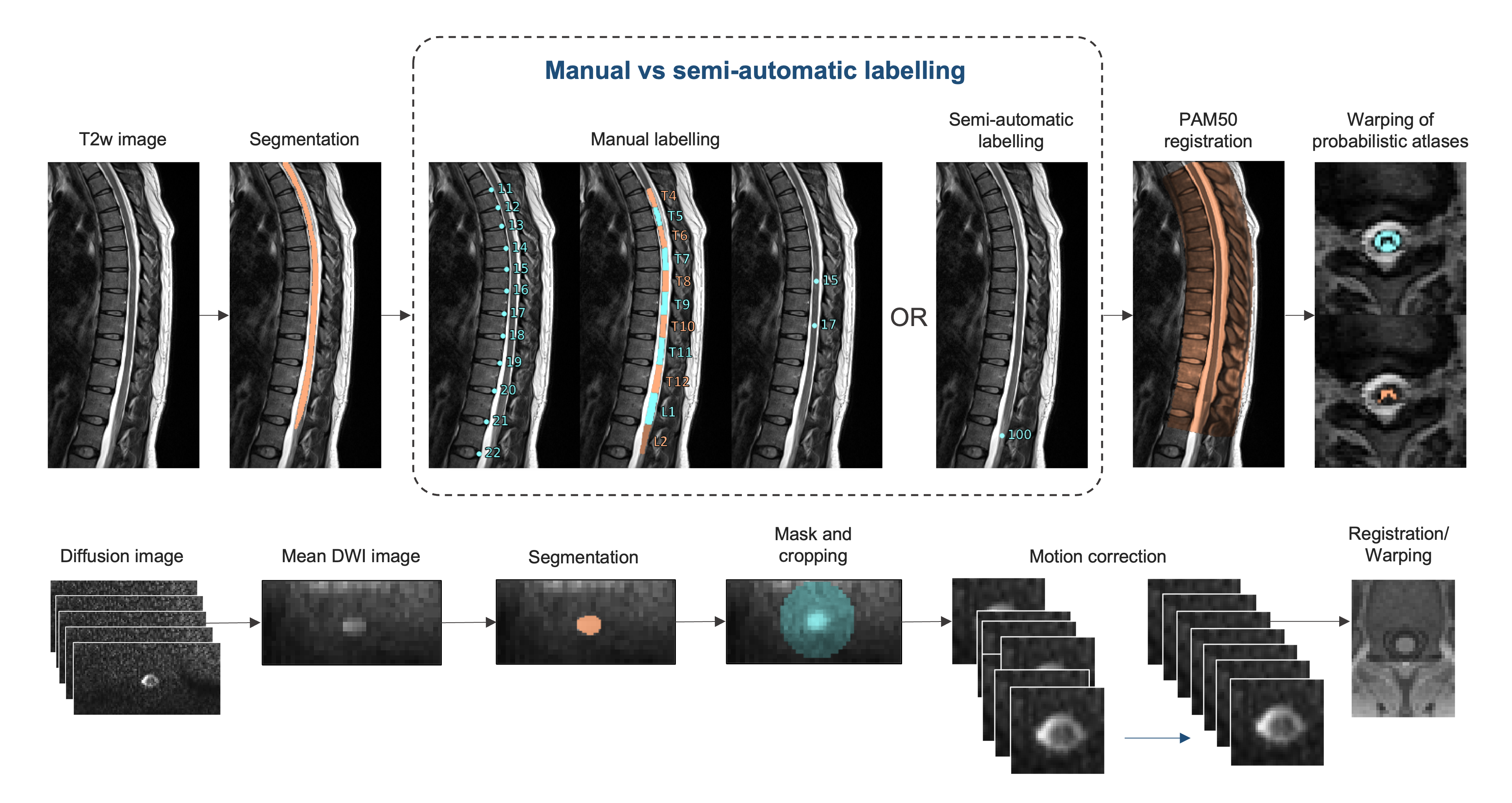
Participant data from our clinical trial (Project SCIN [ACTRN1262200073374]) included two participants with diagnosed chronic complete SCI (m=2, mean age 36.00 years +18.39, American Spinal Injury Association (ASIA) A, levels C5 and T6), and six healthy volunteers (m=2, f=4, mean age 38.00 years +16.15). Following written informed consent, all participants underwent TL-SC diffusion-weighted imaging on a 3T Siemens MAGNETOM Skyra whole-body scanner (Siemens Healthcare, Erlangen, Germany) using a 32-channel spine coil. Diffusion image acquisition employed a single-shot echo planar imaging (EPI) research application sequence comprising 66 interleaved axial slices with TR = 5,000 ms, TE = 80 ms, bandwidth = 1,628 Hz/pixel, FOV = 157 x 234 mm, matrix size = 128 x 86, acceleration factor = 2, and a 2mm slice thickness. An optimised twice-refocused spin-echo plus diffusion scheme was used (6,7), with 12 directions and b value of 0 and 600s/mm2 (1 average). Susceptibility-induced spatial distortions were corrected using a field map-based approach (6,7). Structural T2-weighted images were also acquired using a Sampling Perfection with Application-optimised Contrast using different flip angles (SPACE) acquisition sequence for anatomical reference during pre-processing. The combined total acquisition time for diffusion and structural image acquisition was 11 min 27 sec. Diffusion and structural data were pre-processed twice (Figure 1); the first method employed manual vertebral labelling (total processing time = 16GB RAM: 17 min 12 sec), and the second semi-automatic method involved manual placement of an end-of-cord label (total pre-processing time = 16GB RAM: 12 min 30 sec). Total processing time refers to the pre-processing duration of four parallel participant data sets. Pre-processing and DTI metric extraction were done using the Spinal Cord Toolbox (8). The TL-SC microarchitecture was then spatially mapped using DSI Studio (http://dsi-studio.labsolver.org). DTI metrics, including FA, MD, AD, and RD in the healthy and injured spinal cord, were compared via a two-way analysis of variance (ANOVA; p<0.05). A within-group comparison between manual and semi-automatic labelling of thoracolumbar vertebrae (two-way ANOVA; p<0.05).Results
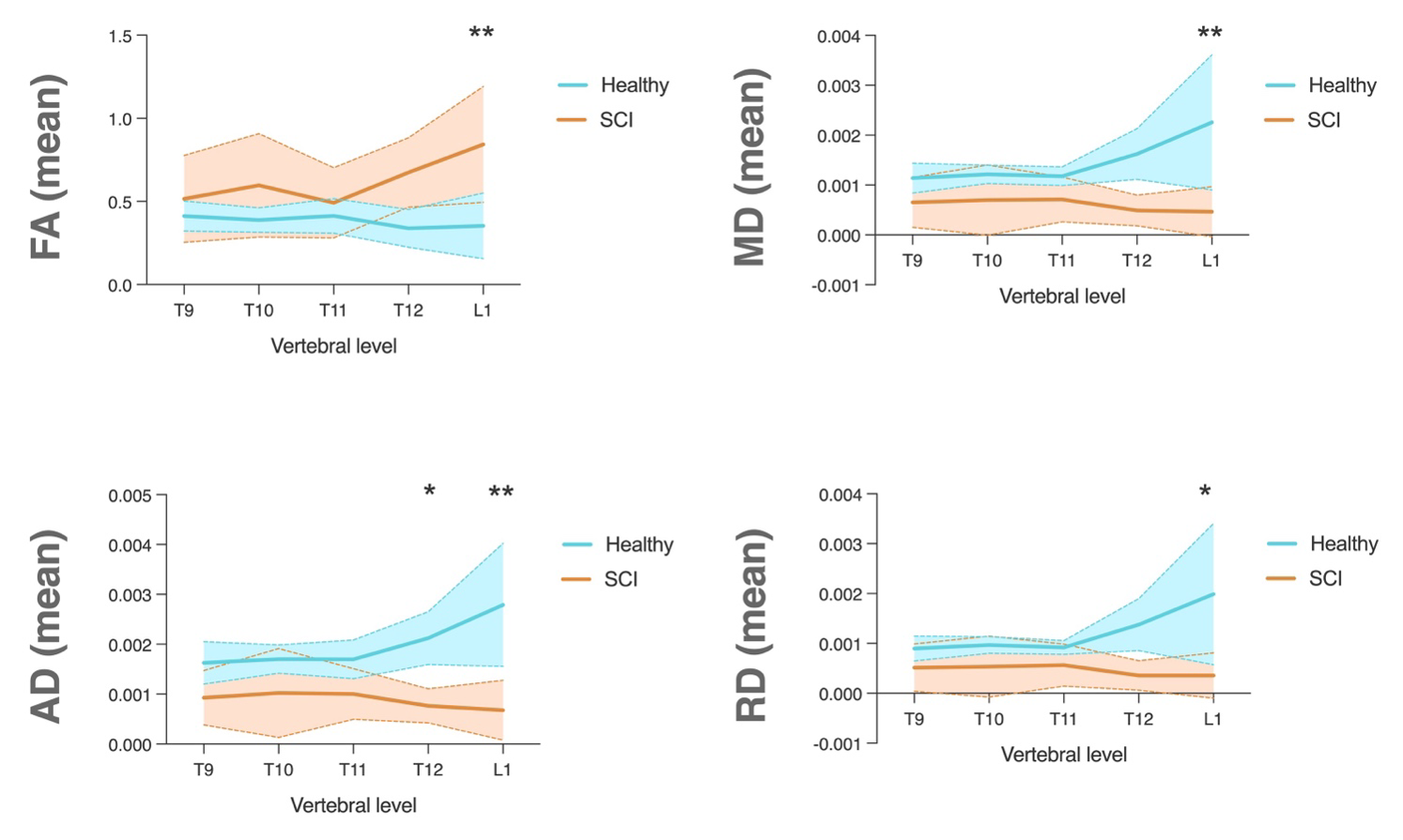
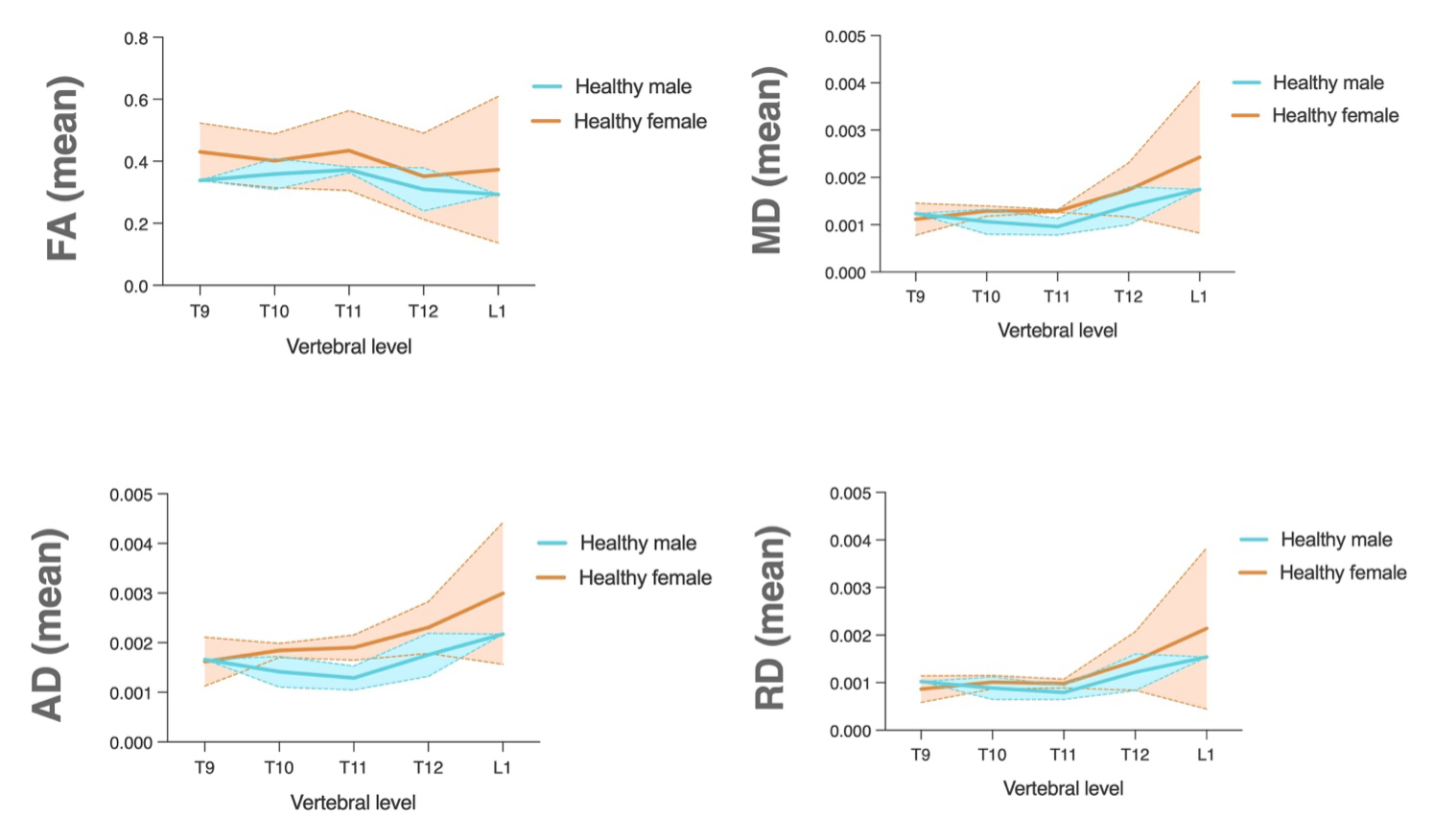
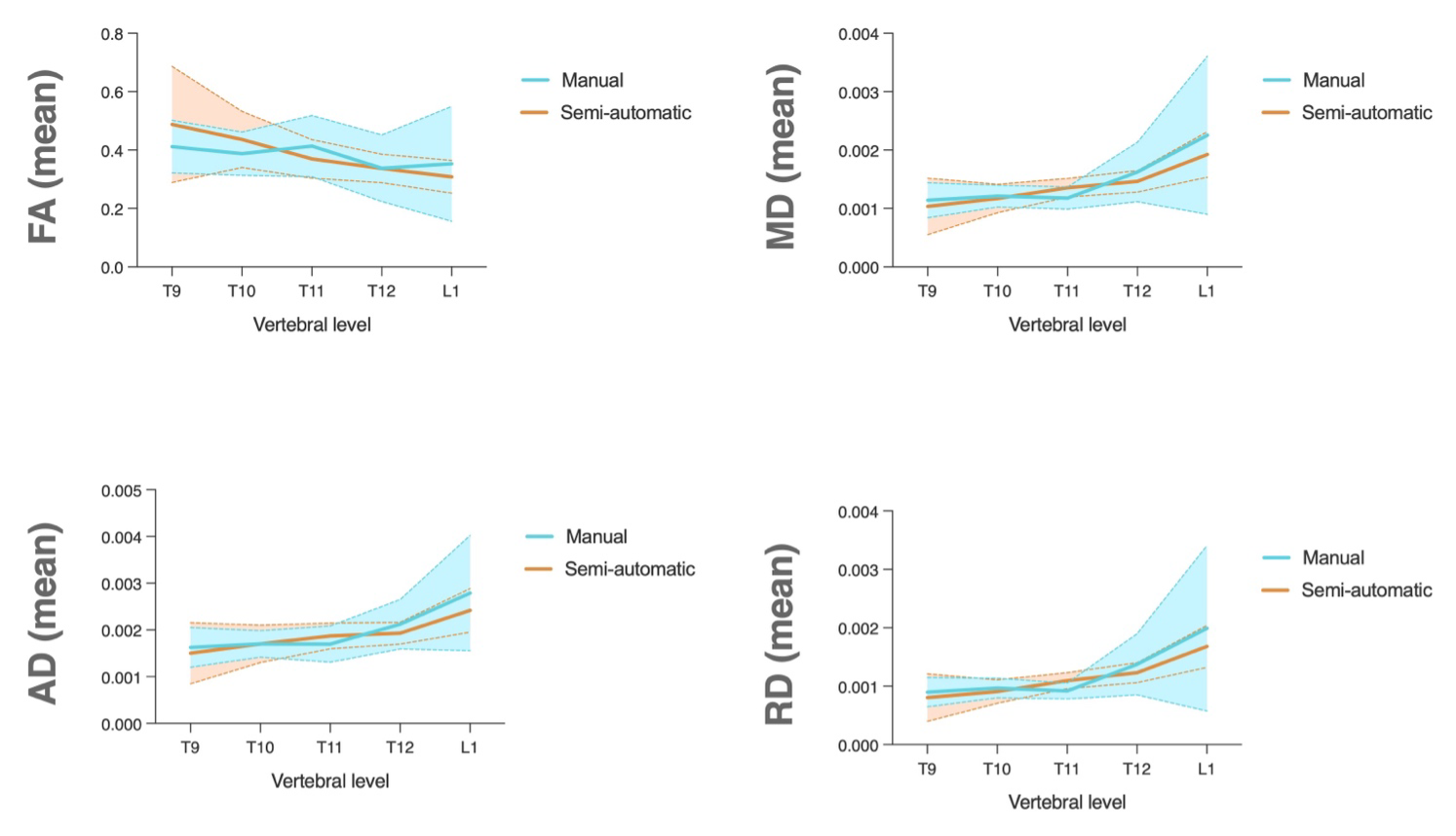
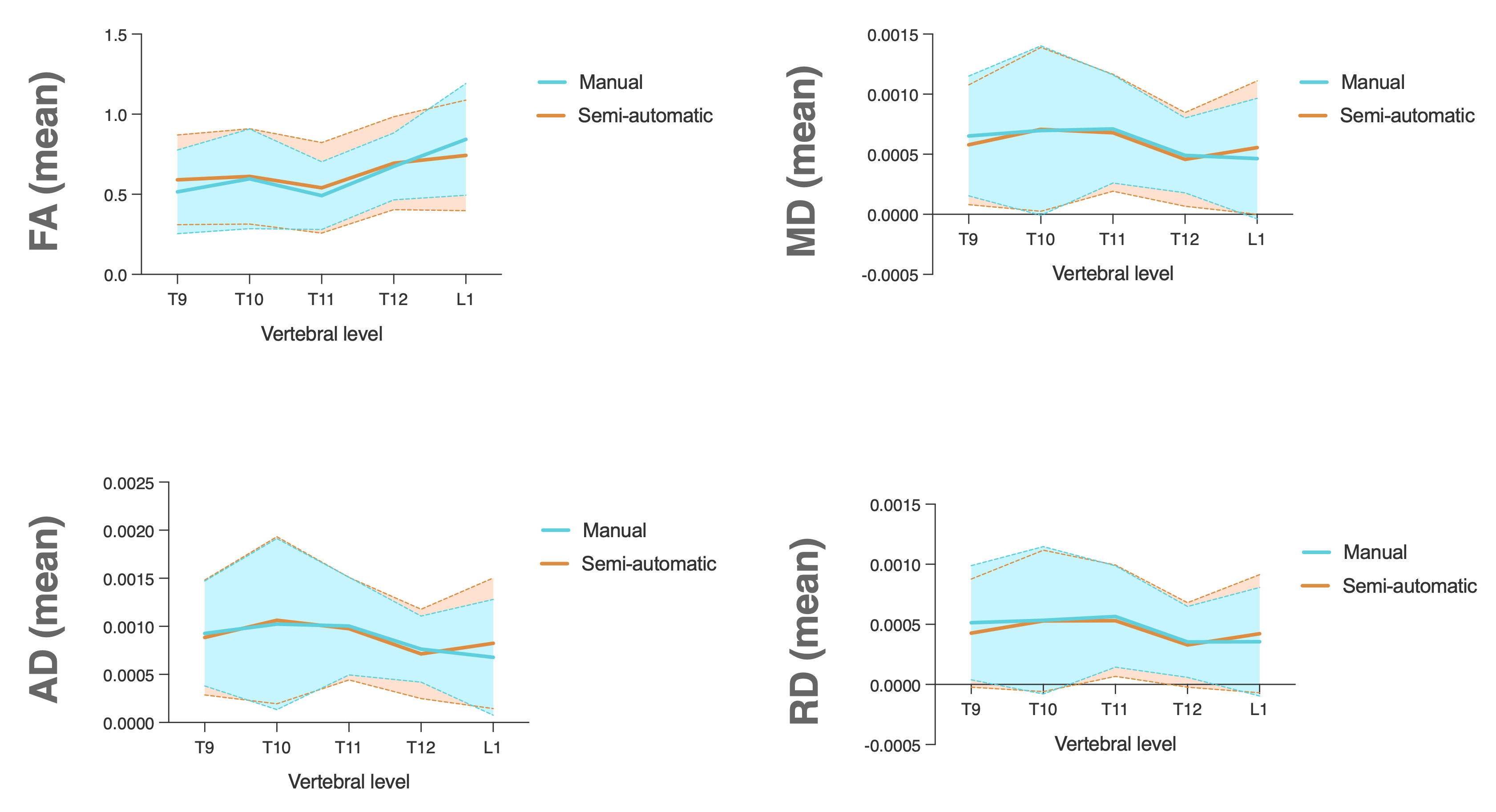
Compared to healthy volunteers, participants with a SCI had decreased AD (p<0.05) at the 12th thoracic vertebral level, as well as increased FA (p<0.01) and decreased MD (p<0.01), AD (p<0.01), and RD (p<0.05) at the first lumbar vertebral segment (Figure 2), suggesting our optimised DTI image acquisition protocol can detect SCI-induced changes in the TL-SC. Furthermore, no significant difference in measured DTI metrics was found between healthy male and female volunteers (Figure 3), nor between semi-automatic and manual thoracolumbar spinal cord data labelling (Figures 4 and 5), demonstrating the potential of semi-automatic labelling as an alternative to other manual techniques.Conclusions
Our optimised TL-SC DTI acquisition and semi-automated analysis pipeline demonstrated sensitivity in detecting SCI-induced microarchitectural changes. The reduced need for user input and a total acquisition and pre-processing time of 23 minutes and 57 seconds provide a more clinically translatable method for interrogating SCI-induced changes in TL-SC microarchitecture without compromising DTI metric accuracy.Acknowledgements
The authors acknowledge the support of the National Imaging Facility, a National Collaborative Research Infrastructure Strategy (NCRIS) capability of Australia.References
1. Wheeler-Kingshott CA, Stroman PW, Schwab JM, et al. The current state-of-the-art of spinal cord imaging: applications. Neuroimage 2014;84:1082-1093.
2. Stroman PW, Wheeler-Kingshott C, Bacon M, et al. The current state-of-the-art of spinal cord imaging: methods. Neuroimage 2014;84:1070-1081.
3. David G, Freund P, Mohammadi S. The efficiency of retrospective artifact correction methods in improving the statistical power of between-group differences in spinal cord DTI. Neuroimage 2017;158:296-307.
4. Mohammadi S, Freund P, Feiweier T, Curt A, Weiskopf N. The impact of post-processing on spinal cord diffusion tensor imaging. Neuroimage 2013;70:377-385.
5. Ullmann E, Pelletier Paquette JF, Thong WE, Cohen-Adad J. Automatic labeling of vertebral levels using a robust template-based approach. Int J Biomed Imaging 2014;2014:719520.
6. Grauhan NF, Grunebach N, Brockstedt L, et al. Reduction of Distortion Artifacts in Brain MRI Using a Field Map-based Correction Technique in Diffusion-weighted Imaging : A Prospective Study. Clin Neuroradiol 2023.
7. Tong A, Lemberskiy G, Huang C, Shanbhogue K, Feiweier T, Rosenkrantz AB. Exploratory study of geometric distortion correction of prostate diffusion-weighted imaging using B0 map acquisition. Journal of Magnetic Resonance Imaging 2019;50(5):1614-1619.
8. De Leener B, Levy S, Dupont SM, et al. SCT: Spinal Cord Toolbox, an open-source software for processing spinal cord MRI data. Neuroimage 2017;145(Pt A):24-43.
Figures