2522
Quantitative and Comparative Evaluation of 2D Reduced-FOV Multi-shot Diffusion Tensor Imaging in Spinal Cord1Department of Biomedical Engineering, The Chinese University of Hong Kong, Hong Kong, China, 2Multi-Scale Medical Robotics Center, Hong Kong, China, 3Department of Diagnostic Radiology, The University of Hong Kong, Hong Kong, China
Synopsis
Keywords: Spinal Cord, Spinal Cord, reduced-FOV, multi-shot DTI
Motivation: To our best knowledge, there has yet to be a comprehensive evaluation of the combination of cardiac triggering, reduced-FOV, or multi-shot techniques together for improving spinal cord DTI.
Goal(s): This study aims to compare the performances of spinal cord DTI with different parametric combinations.
Approach: Extensive and comparative experiments in five aspects were conducted.
Results: Results demonstrate that multi-shot DTI with MUSE could achieve better reconstruction in the spinal cord. A combination of reduced-FOV and multi-shot techniques could be adopted simultaneously in pursuit of ultimate distortion correction. In addition, cardiac triggering should be equipped to reduce the influences on cerebrospinal fluid pulsation.
Impact: Multi-shot DTI with MUSE and cardiac triggering might be the optimal combination for clinical diagnosis of the spinal cord if available on commercial MRI scanners. Future coil design could focus on customized coil arrangement of the spinal cord for optimization.
Introduction
Diffusion tensor imaging (DTI) can reflect the microstructural integrity of the spinal cord1~2, and single-shot diffusion-weighted echo-planar imaging is the most commonly used sequence for data acquisition (i.e., single-shot DTI). Despite high scan efficiency, single-shot DTI suffers from several disadvantages, as shown in Fig.1(a)~(d), therefore hindering the clinical adoption of spinal cord DTI. Previous studies have proposed to apply cardiac triggering, reduced-FOV (r-FOV), or multi-shot techniques (e.g., multiplexed sensitivity encoding; MUSE3) to partially address the aforementioned problems4~5. To our best knowledge, however, there has yet to be a comprehensive evaluation of the combination of different strategies together for improving spinal cord DTI. Therefore, this study aims to compare the performances of spinal cord DTI with different combinations of r-FOV and multi-shot parameters, and also investigate the influence of reconstruction strategies for improving image quality.Methods
Experimental designTo compare the reconstruction performances of r-FOV multi-shot spinal cord DTI and demonstrate the effectiveness of reconstruction strategies in different aspects. Extensive experiments were conducted as listed in Fig.1(e).
Data acquisition
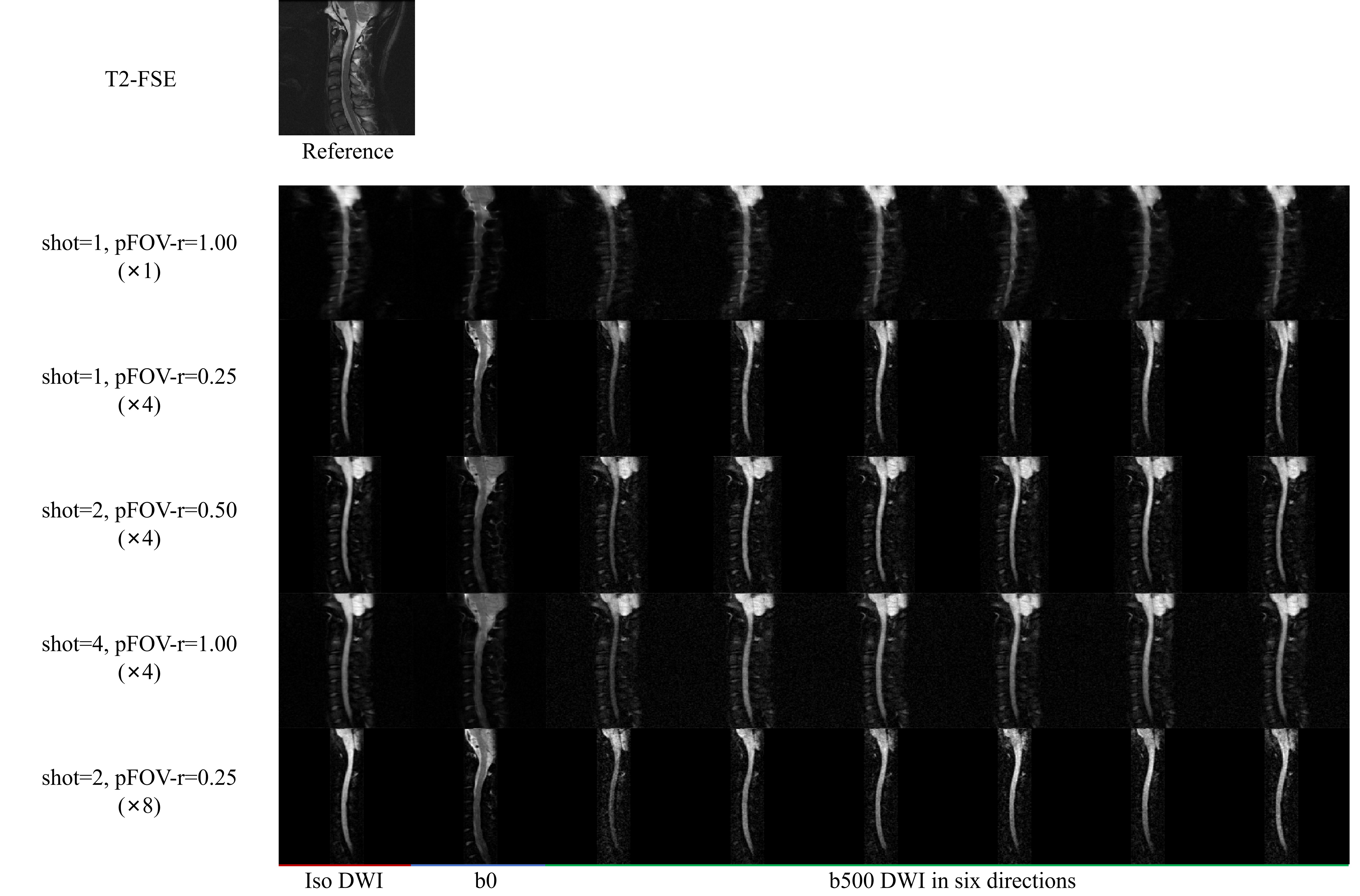
Sagittal cervical spinal cord DTI data with 6 diffusion directions was acquired on a 1.5T MRI scanner (Artist, GE Healthcare) from 2 healthy subjects using a 19-channel head coil, 40-channel spine coil, and 30-channel body coil with following scan parameters: Resolution=0.94×0.94mm2, FOV=180×(180*pFOV-r)mm, matrix size=192×(192*pFOV-r), over-scan for partial Fourier=8, TE=63ms, TR=4000ms or 4 cardiac cycle (3000ms~4000ms) depends on subject’s heart rate, b-value=500s/mm2, thickness=4mm, spacing=0.5mm, number of slices=7. Peripheral pulse unit was adopted for cardiac triggering with trigger delay time=200ms. In addition to 2D-RF excitation for achieving r-FOV, the outer volume suppression was also used to further reduce the residual signals outside the excited FOV. Furthermore, routine T2-FSE was acquired at the same slice locations for serving as the geometric gold standard.
Data analysis
The region-of-interest (ROI) of the cervical spinal cord was manually contoured on each slice using the ITK-SNAP software. The image quality and the contrast between ROI and background tissues (e.g., vertebral body and intervertebral disc) were assessed using SNR and CNR based on the NEMA1 difference method6~7. The repeatability of signal intensity among NEX and the extent of signal loss in apparent diffusion coefficient (ADC) measurement of all sequences were quantitatively evaluated using the coefficient of variation (CV)8 and ADC ratio9, respectively. The performance of distortion reduction was evaluated using dice similarity coefficient (DSC) by measuring the overlap between the ROI in T2-FSE and DTI data. A pair student t-test was used for statistical analysis. P-value<0.01 indicates statistical significance.
Results
Fig.2 compares the reconstruction performances of spinal cord DTI with different strategies. Fig.3 compares the reconstruction results of different parametric DTI acquisitions and reconstruction algorithms. Fig.4 presents the comparison of SNR and CNR maps among different parametric combinations. Fig.5 demonstrates the comparison of different distortion levels for DWIs with different acceleration factors along phase-encoding.Discussion and Conclusion
For different parametric combinations, 4-shot full-FOV DTI could yield best CNR, CV, and ADC ratio, suggesting that the multi-shot technique with MUSE may be superior to r-FOV in terms of improving contrast, repeatability, and signal loss. Compared with severe distortion present in single-shot full-FOV DTI, integrating multi-shot and r-FOV techniques could achieve a more efficient distortion reduction (i.e., 2-shot 0.25-FOV DTI in Fig.5). Cardiac triggering could alleviate the signal loss due to CSF pulsation but also lead to unstable repeatability (P is near significant). The increase of CV with triggering might have originated from the signal variations (i.e., different degrees of T1-weighting) caused by the various TRs among the subject’s heart rate. Furthermore, this effect was more obvious in single-shot than multi-shot DTI, which might be because the multi-shot phase correction can also reduce signal loss originating from phase dispersion induced by cardiac motion. Among different reconstruction algorithms, single-shot DTI with iFFT yielded a high noise floor due to magnitude average, leading to a high SNR but low CNR, which may not be conducive to clinical diagnosis. In contrast, MUSE could achieve better CNR and reduction of signal loss for both single-shot and multi-shot DTI because its effective phase correction also enabled complex average, as shown in Fig.3~4. Although the performance of MUSE highly relies on a number of coils, increasing the number of coil elements could only gain subtle performance improvement due to the elongated shape of the cervical spine. In conclusion, multi-shot DTI with triggering and MUSE might be the optimal choice for data acquisition in the spinal cord. This study still has limitations, such as small samples, and no quantitative measurement or comparison of ADC and fractional anisotropy (FA) between healthy subjects and patient cohorts.Acknowledgements
The work was in part supported by grants from Hong Kong Research Grant Council (GRF17106820, GRF17125321, GRF14206723, and ECS24213522).References
[1] Dong Q, Welsh R C, Chenevert T L, et al. Clinical applications of diffusion tensor imaging[J]. Journal of Magnetic Resonance Imaging: An Official Journal of the International Society for Magnetic Resonance in Medicine, 2004, 19(1): 6-18.
[2] Shabani S, Kaushal M, Budde M D, et al. Diffusion tensor imaging in cervical spondylotic myelopathy: a review[J]. Journal of Neurosurgery: Spine, 2020, 33(1): 65-72.
[3] Chen N, Guidon A, Chang H C, et al. A robust multi-shot scan strategy for high-resolution diffusion weighted MRI enabled by multiplexed sensitivity-encoding (MUSE)[J]. Neuroimage, 2013, 72: 41-47.
[4] Saritas E U, Cunningham C H, Lee J H, et al. DWI of the spinal cord with reduced FOV single‐shot EPI[J]. Magnetic Resonance in Medicine: An Official Journal of the International Society for Magnetic Resonance in Medicine, 2008, 60(2): 468-473.
[5] Xu X, Zhang B, Sun K, et al. Reliability and validity of multi-shot DWI in diagnosis of cervical spondylotic myelopathy: a study based on 3-T MRI[J]. European Spine Journal, 2020, 29: 1219-1226.
[6] Griffanti L, Baglio F, Preti M G, et al. Signal-to-noise ratio of diffusion weighted magnetic resonance imaging: Estimation methods and in vivo application to spinal cord[J]. Biomedical Signal Processing and Control, 2012, 7(3): 285-294.
[7] Crop F, Robert C, Viard R, et al. Efficiency and Accuracy Evaluation of Multiple Diffusion‐Weighted MRI Techniques Across Different Scanners[J]. Journal of Magnetic Resonance Imaging, 2023.
[8] Chang H C, Hui E S, Chiu P W, et al. Phase correction for three‐dimensional (3D) diffusion‐weighted interleaved EPI using 3D multiplexed sensitivity encoding and reconstruction (3D‐MUSER)[J]. Magnetic resonance in medicine, 2018, 79(5): 2702-2712.
[9] Liu Y J, Lee Y H, Chang H C, et al. A potential risk of overestimating apparent diffusion coefficient in parotid glands[J]. PloS one, 2015, 10(4): e0124118.
Figures