2521
Monitoring of therapeutic response using lesion segmentation and DTI in adult cerebral adrenoleukodystrophy treated with Leriglitazone1Sorbonne Université, INSERM, CNRS, Laboratoire d'Imagerie Biomédicale, Paris, France, 23Department of Pathobiology of the Nervous System, Center for Brain Research, Medical University of Vienna, Vienna, Austria, 3Department of Medical Genetics, Reference Centers for Adult Neurometabolic diseases and Adult Leukodystrophies, AP-HP, Pitié-Salpêtrière University Hospita, Paris, France, 4Minoryx Therapeutics, Barcelona, Spain, 5Braintale (Software As a Service), Paris, France, 6Department of Neuroradiology, AP-HP, Pitié-Salpêtrière University Hospital, Paris, France, 7Department of Medical Genetics, Reference Centers for Adult Neurometabolic diseases and Adult Leukodystrophies, AP-HP, Pitié-Salpêtrière University Hospital, Paris, France
Synopsis
Keywords: White Matter, Brain, Adrenoleukodystrophy, Leriglitazone, Volumetric analysis, Diffusion Tensor Imaging
Motivation: Cerebral adrenoleukodystrophy (CALD) is a rare and devastating demyelinating disease. The standard of care is hematopoeitic stem cell transplantation (HCST), which efficacy is limited to early-stage patients.
Goal(s): We studied the efficacy of Leriglitazone in CALD patients, either not eligible or awaiting HSCT.
Approach: Leriglitazone was administered to thirteen adult male patients. They underwent brain MRI every 3 months, with a quantitative analysis of lesion volumes on FLAIR, diffusion tensor parameters and gadolinium enhancements.
Results: The disease stabilized in all patients awaiting HSCT. Corticospinal tract lesions downsized in most patients and turned gadolinium-negative, showing a selective effect of this molecule on motor pathways.
Impact: Cerebral adrenoleukodystrophy is a devastating demyelinating disease, fatal for all patients without early stem cell transplantation. We showed that Leriglitazone represents a therapeutic alternative, allowing clinical and radiological stabilization in ten men. Remarkably, motor pathways lesions downsized and turned gadolinium-negative.
Introduction
X-linked adrenoleukodystrophy (X-ALD) is the most common leukodystrophy. All men affected develop a progressive spastic paraparesis (Adrenomyeloneuropathy, AMN).1 In addition, 1/3 of boys and >50% of men develop the cerebral form of the disease (CALD) which causes a devastating inflammatory demyelination with a median survival of 3 years.2Brain MRI is the gold standard for diagnosis, showing hyperintensities on FLAIR typically located in the corpus callosum, the corticospinal tracts (CST) and the cerebellum, that may be enhanced after gadolinium injection.3 Diffusion tensor imaging (DTI) parameters were shown to be sensitive outcome measures for myelopathy progression in AMN,4–7 whereas their relevance in CALD remains to be investigated. In daily practice, therapeutic management is guided by the number of white matter regions affected (corresponding to the Loes score8) and the location of lesions, which are associated with poor prognosis in the CST and cerebellum white matter.9 The gold standard treatment for early-stage CALD is hematopoietic stem cell transplantation (HSCT), which halts the neuroinflammatory process.10 Unfortunately, HSCT cannot be performed in elderly patients, or if the lesions have a poor prognosis.11
Leriglitazone is a novel selective PPAR-gamma agonist with anti-inflammatory properties that crosses the blood-brain barrier.12 The ADVANCE study demonstrated that in AMN patients Leriglitazone reduced the proprioceptive impairment associated with myelopathy and the risk of CALD conversion.13 Following these major results, we conducted a study to treat CALD adult patients with Leriglitazone, comprising a monitoring of lesion volumes and DTI parameters in different white-matter regions.
Material and Methods
Since 2021, we treated 13 men not eligible for HSCT (n=8) or awaiting HSCT (n=5) at La Pitié-Salpétrière Hospital, AP-HP, Paris. Patients were assessed every 3 months by standardized neurological scales and brain imaging on a 3.0 Tesla MRI scanner. The protocol included a 3D-FLAIR sequence, DTI, a 3D T1-w MPRAGE sequence and a 3D T1-w Turbo Spin Echo sequence after gadolinium injection.Longitudinal segmentation of CALD lesions was done manually after coregistration of all timepoints in a within-subject intermediate T1-w template according to the methodology of Reuter et al.14 in order to avoid reproducibility bias. We calculated total lesion load and CST lesion volume (comprising internal capsules, cerebral peduncles and the pons).
DTI sequences were processed with brainQuant module from the brainTale-care platform (version 2.2.0). We calculated mean values of fractional anisotropy (FA) and mean diffusivity (MD) of total white-matter, and regional values of MD from a 19-regions deep white-matter atlas.15
Results
Of 13 patients, one died at 3 months from Covid19 infection and two (>60 years old with cognitive impairment) continued to deteriorate. The other 10 patients (including 7 patients with > 1 year of treatment) showed an excellent clinical and radiological response, with complete clinical stability and stable lesion load in most patients (Figure 2). Remarkably, all the lesions involving the CST turned gadolinium-negative and downsized in 4 patients (out of 5) on volumetric analysis for three patients and visual assessment for one patient (Figure 3). On the other hand, two patients had a major progression of white-matter cerebellar lesions. Global FA and MD of total white matter was overall stable in patients who did not deteriorate clinically. Regional MD values showed variations which seemed to be in line with the volumetric evolution of lesions (Figure 4). Treatment was well-tolerated and HSCT is currently no longer indicated for the 5 patients awaiting transplantation.Discussion and Conclusion
These encouraging results suggest that Leriglitazone can halt the lethal neuroinflammatory process in men with CALD. The remarkable efficacy on CST lesions suggests that this treatment has a specific action on the motor pathways, which is of particular interest as these lesions are associated with poor prognosis. Among the patients who developed extensive lesions in the cerebellum, one had a medical history of posterior fossa ependymoma, and the other reported chronic alcohol abuse during the study. We inferred that these conditions led to an additional vulnerability of the cerebellum to demyelination. The two patients who continued to deteriorate under treatment were the oldest of the study and had a prominent cognitive impairment, which were also associated with poor outcomes after HSCT. Limitations to this study include a small sample size and the absence of a placebo group. However, the evolution of our patients was similar to what was observed after HSCT in early-stages CALD.9To conclude, this treatment represents a genuine therapeutic alternative to HSCT for ALD. Lesion volume and DTI markers in the deep white matter were useful tools to assess therapeutic response. The role of DTI in CALD should be further investigated in future studies.
Acknowledgements
The authors would like to thank the patients who agreed to take part in this study, as well as Minoryx Therapeutics which funded their treatment.References
1. Engelen M, Kemp S, Poll-The BT. X-linked adrenoleukodystrophy: pathogenesis and treatment. Curr Neurol Neurosci Rep. 2014;14(10):486. doi:10.1007/s11910-014-0486-0
2. Mallack EJ, Turk B, Yan H, Eichler FS. The Landscape of Hematopoietic Stem Cell Transplant and Gene Therapy for X-Linked Adrenoleukodystrophy. Curr Treat Options Neurol. 2019;21(12):61. doi:10.1007/s11940-019-0605-y
3. Liberato AP, Mallack EJ, Aziz-Bose R, et al. MRI brain lesions in asymptomatic boys with X-linked adrenoleukodystrophy. Neurology. 2019;92(15):e1698-e1708. doi:10.1212/WNL.0000000000007294
4. Adanyeguh IM, Lou X, McGovern E, et al. Multiparametric in vivo analyses of the brain and spine identify structural and metabolic biomarkers in men with adrenomyeloneuropathy. NeuroImage Clin. 2021;29:102566. doi:10.1016/j.nicl.2021.102566
5. Huffnagel IC, van Ballegoij WJC, Vos JMBW, Kemp S, Caan MWA, Engelen M. Longitudinal diffusion MRI as surrogate outcome measure for myelopathy in adrenoleukodystrophy. Neurology. 2019;93(23):e2133-e2143. doi:10.1212/WNL.0000000000008572
6. Castellano A, Papinutto N, Cadioli M, et al. Quantitative MRI of the spinal cord and brain in adrenomyeloneuropathy: in vivo assessment of structural changes. Brain J Neurol. 2016;139(Pt 6):1735-1746. doi:10.1093/brain/aww068
7. Politi LS, Castellano A, Papinutto N, et al. Longitudinal quantitative magnetic resonance imaging in adrenomyeloneuropathy. Eur J Neurol. 2019;26(10):1341-1344. doi:10.1111/ene.13959
8. Loes DJ, Hite S, Moser H, et al. Adrenoleukodystrophy: a scoring method for brain MR observations. AJNR Am J Neuroradiol. 1994;15(9):1761-1766.
9. Kühl JS, Suarez F, Gillett GT, et al. Long-term outcomes of allogeneic haematopoietic stem cell transplantation for adult cerebral X-linked adrenoleukodystrophy. Brain J Neurol. 2017;140(4):953-966. doi:10.1093/brain/awx016
10. Eichler F, Mahmood A, Loes D, et al. Magnetic resonance imaging detection of lesion progression in adult patients with X-linked adrenoleukodystrophy. Arch Neurol. 2007;64(5):659-664. doi:10.1001/archneur.64.5.659
11. Raymond GV, Aubourg P, Paker A, et al. Survival and Functional Outcomes in Boys with Cerebral Adrenoleukodystrophy with and without Hematopoietic Stem Cell Transplantation. Biol Blood Marrow Transplant J Am Soc Blood Marrow Transplant. 2019;25(3):538-548. doi:10.1016/j.bbmt.2018.09.036
12. Ao C, Huo Y, Qi L, Xiong Z, Xue L, Qi Y. Pioglitazone suppresses the lipopolysaccharide-induced production of inflammatory factors in mouse macrophages by inactivating NF-kappaB. Cell Biol Int. 2010;34(7):723-730. doi:10.1042/CBI20090005
13. Köhler W, Engelen M, Eichler F, et al. Safety and efficacy of leriglitazone for preventing disease progression in men with adrenomyeloneuropathy (ADVANCE): a randomised, double-blind, multi-centre, placebo-controlled phase 2-3 trial. Lancet Neurol. 2023;22(2):127-136. doi:10.1016/S1474-4422(22)00495-1
14. Reuter M, Schmansky NJ, Rosas HD, Fischl B. Within-subject template estimation for unbiased longitudinal image analysis. Neuroimage. 2012;61(4):1402-1418. doi:10.1016/j.neuroimage.2012.02.084
15. Mori S, Oishi K, Jiang H, et al. Stereotaxic white matter atlas based on diffusion tensor imaging in an ICBM template. NeuroImage. 2008;40(2):570-582. doi:10.1016/j.neuroimage.2007.12.035
Figures
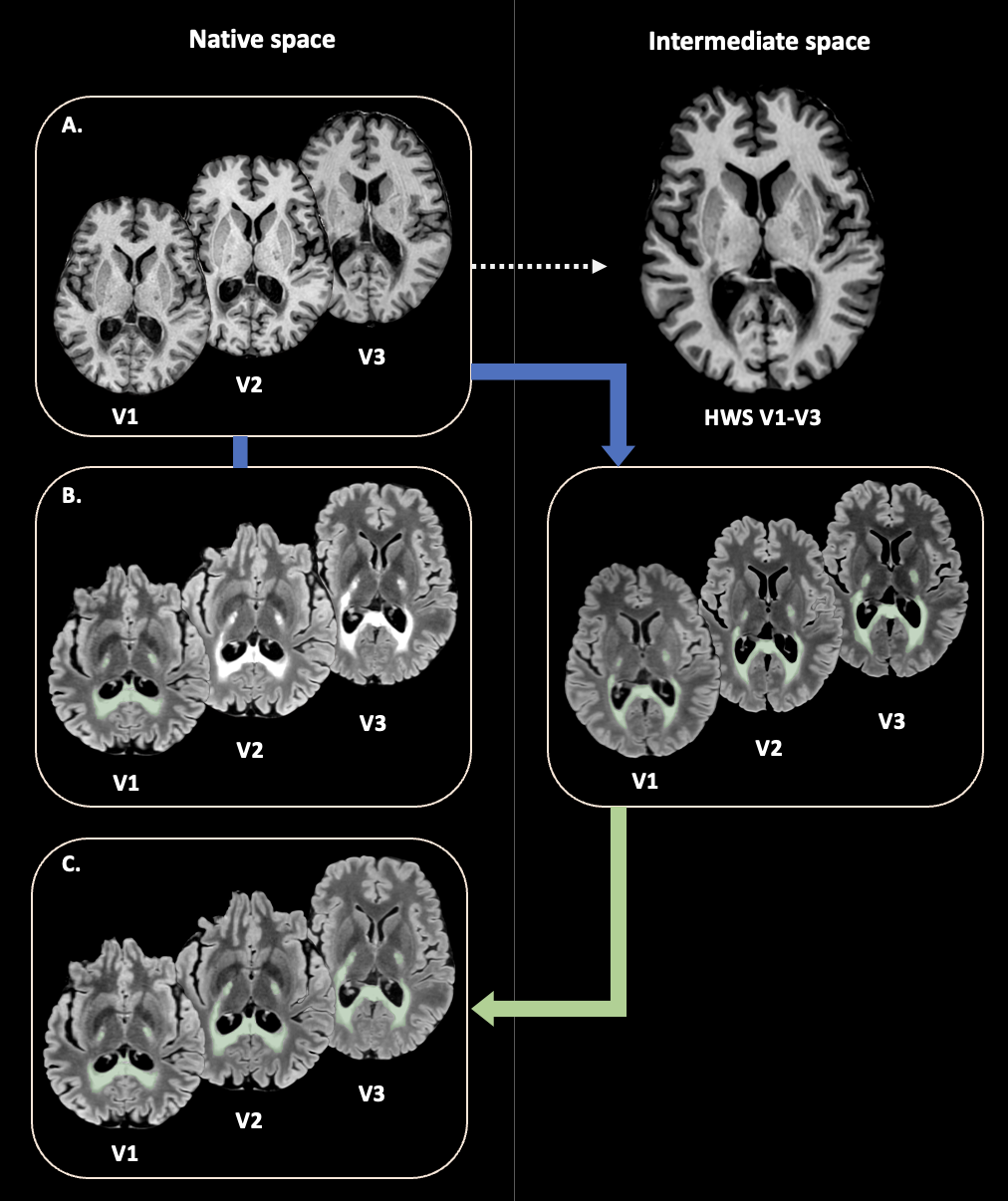
(A) T1 sequences at each visit were bias field corrected, denoised and skull-stripped. A T1 template (halfway space, HWS) was created from the mean of all visits (dashed arrow).
(B) Lesions were segmented manually on the visit 1 (V1) FLAIR. All FLAIR were rigidly and inverse-consistently coregistered to the HWS (blue arrow). Segmentation of next visits was done in the HWS, by adapting the V1 mask to lesion borders.
(C) Segmentations were resliced into their native space (green arrow) to avoid interpolation errors.
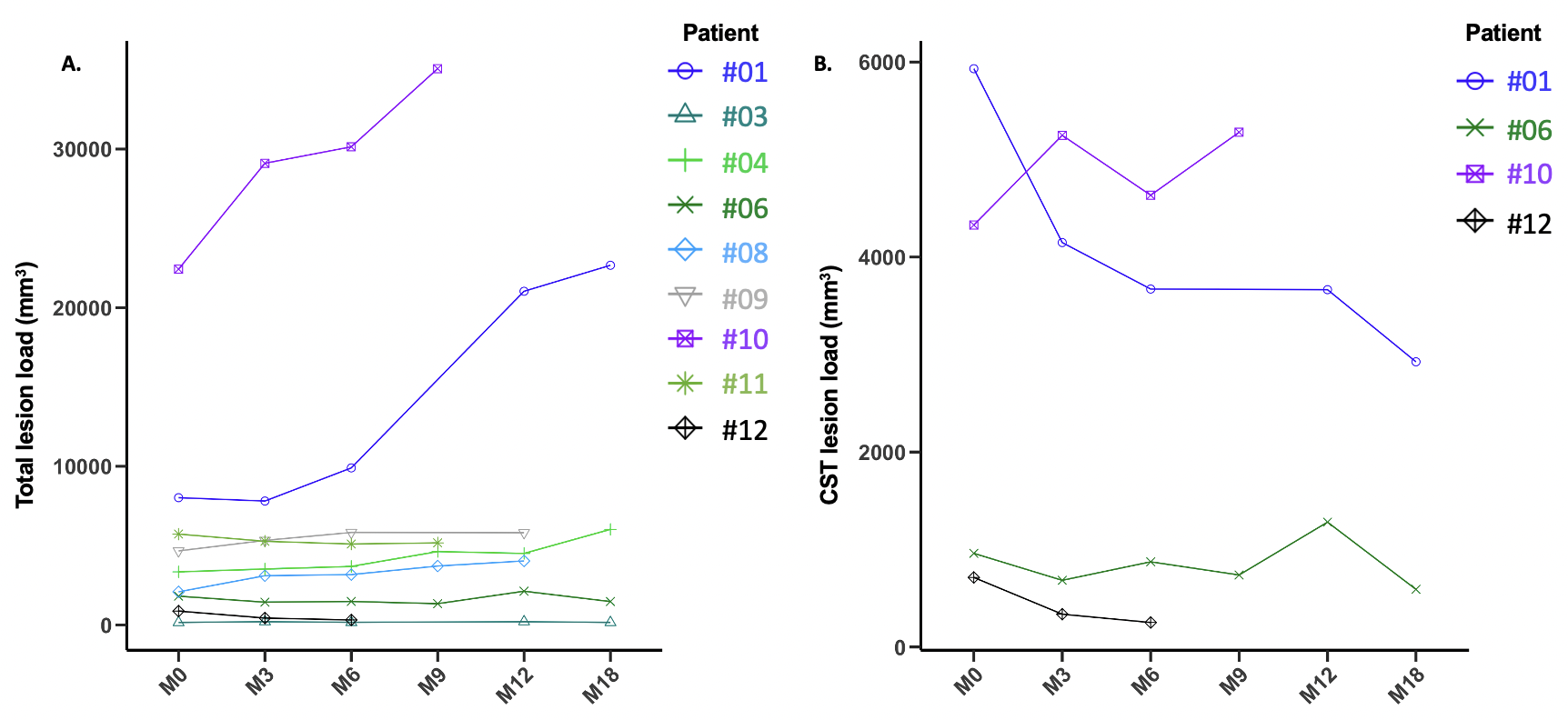
Evolution of total lesion load (A) and CST lesion load (B) over time.
Volumetric analysis was done on the 9 patients who did not have motion artefacts on FLAIR sequence.
(A) Total lesion load remained globally stable in most patients . Two patients (#01, #10) showed a continuous increase of lesion load, due to a progression of cerebellar white matter lesions in both cases.
(B) CST lesion load decreased continuously in patients #01 and #12. It fluctuated in patients #06 and #10, decreasing in cerebral peduncles and increasing (transiently for patient #06) in internal capsules in both cases.
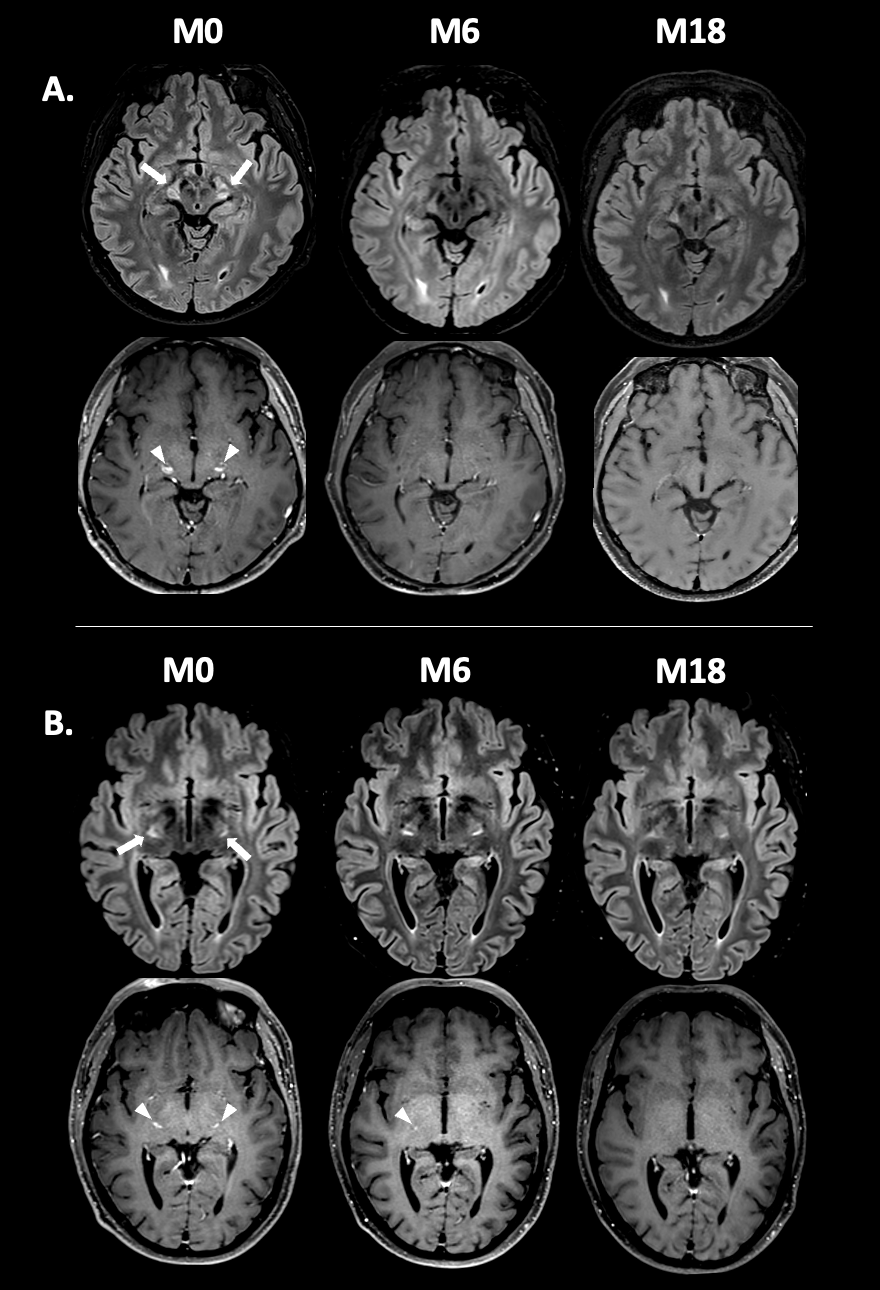
Evolution of CST lesion load and gadolinium enhancements in two CALD patients.
FLAIR sequences are shown in upper rows and T1 post-contrast sequences are shown in lower rows.
(A) Patient (#01) with bilateral lesions of cerebral peduncles at M0 (arrows) with bilateral enhancement (arrowheads), that decreased in size with disappearance of contrast uptake from M6 onwards.
(B) Patient (#06) with bilateral lesions in internal capsules at M0 (arrows) with bilateral enhancement (arrowheads). The enhancements disappeared at M12, with a fluctuating lesion volume that was minimal at M18.
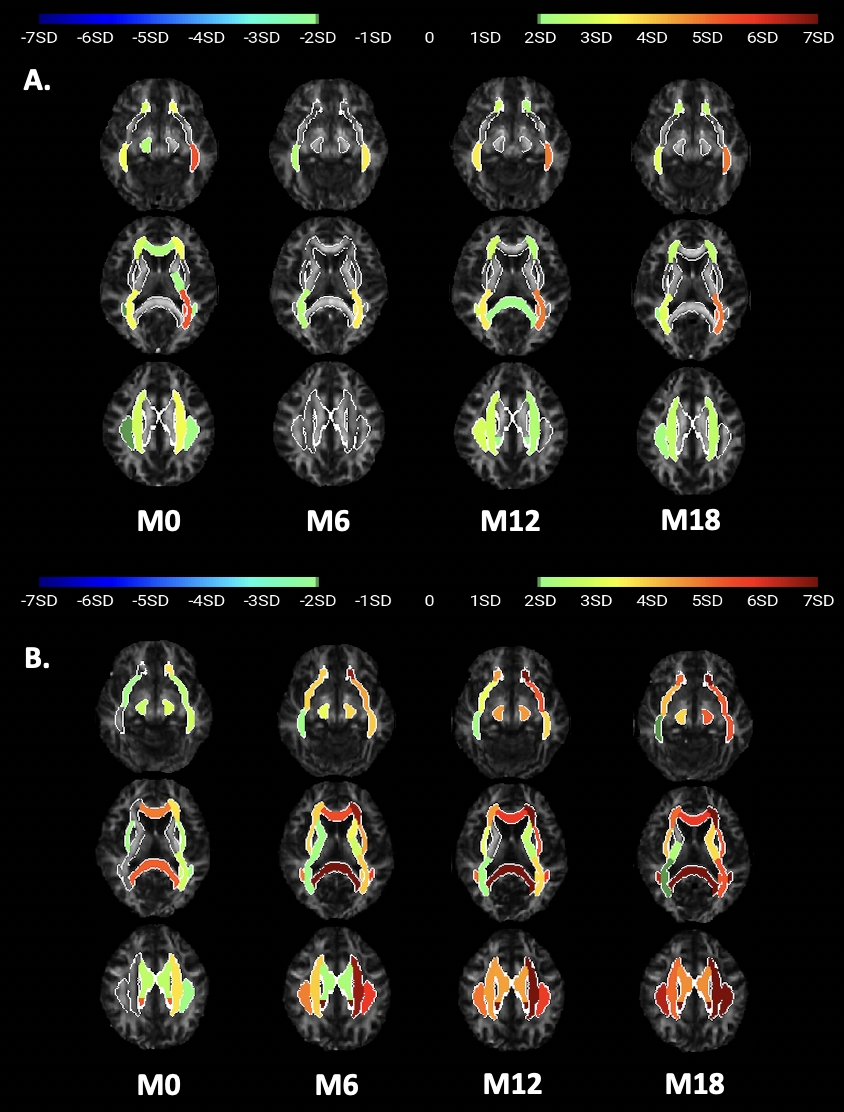
Evolution of the regional MD values (in standard deviations) in different regions of the deep white-matter atlas.
Diffusion analysis was done on 10 patients who did not have motion artefacts on diffusion sequence.
(A) Patient #06 showed a decrease of MD values at M6, that returned close to the baseline values at M12 and decreased at M18, in line with the volumetric evolution of his lesions.
(B) Patient #02 showed increased MD values in all regions from M6 onwards, in line with deteriorating clinical status and spreading of his lesions that turned gadolinium-positive on his latest brain MRI.