2520
A Matched Case Control Study of Early Cervical Spondylotic Myelopathy Based on Diffusion Magnetic Resonance Imaging1Department of Radiology, Peking University Third Hospital, BeiJing, China, 2MR Collaboration, Siemens Healthineers Ltd., BeiJing, China, 3Department of Orthopedics, Peking University Third Hospital, BeiJing, China
Synopsis
Keywords: Spinal Cord, Spinal Cord, Cervical Spondylotic Myelopathy; Diffusion Magnetic Resonance Imaging
Motivation: Early cervical spondylotic myelopathy (CSM) is challenging to diagnose and easily missed.
Goal(s): To explore the value of diffusion MRI (dMRI) in diagnosing early-stage CSM and evaluating uncompressed segments in patients with early CSM.
Approach: Using diffusion tensor imaging (DTI), diffusion kurtosis imaging (DKI), and neurite orientation dispersion and density imaging (NODDI), a 1:1 matched case control study was conducted.
Results: The orientation division index (ODI) was positively correlated with early CSM, and the anisotropic water fraction (AWF) was negatively correlated. The ODI and AWF can assist in identifying the scope of early CSM involvement.
Impact: The orientation division index (ODI) was positively correlated with early CSM, and the anisotropic water fraction (AWF) was negatively correlated. The ODI and AWF can assist in identifying the scope of early CSM involvement.
Introduction
Introduction Cervical spondylotic myelopathy (CSM) is one of the most common nontraumatic spinal cord injuries in adults [1]. There is usually an insidious onset to early CSM, and as the disease progresses, it may lead to irreversible spinal cord damage. Therefore, accurate identification and intervention for CSM patients as early as possible can reduce the adverse consequences caused by continuous disease progression [2]. Due to the mild clinical symptoms and diverse manifestations of early CSM, its diagnosis is difficult and dependent upon the experience level of the clinician [3]. MRI is a common examination method for the noninvasive preoperative evaluation of CSM and an important reference for formulating individualized treatment plans [4]. However, there are no abnormal signals in the spinal cord or obvious spinal stenosis in early CSM, which can result in missed diagnoses in some early CSM patients [3, 5]. Diffusion MRI (dMRI) exploits the diffusion behaviour of water molecules to characterize local microscopic structural changes in tissue and has been used to evaluate CSM. Studies have proven that dMRI can noninvasively assess the severity of CSM and predict its prognosis before surgery.Methods
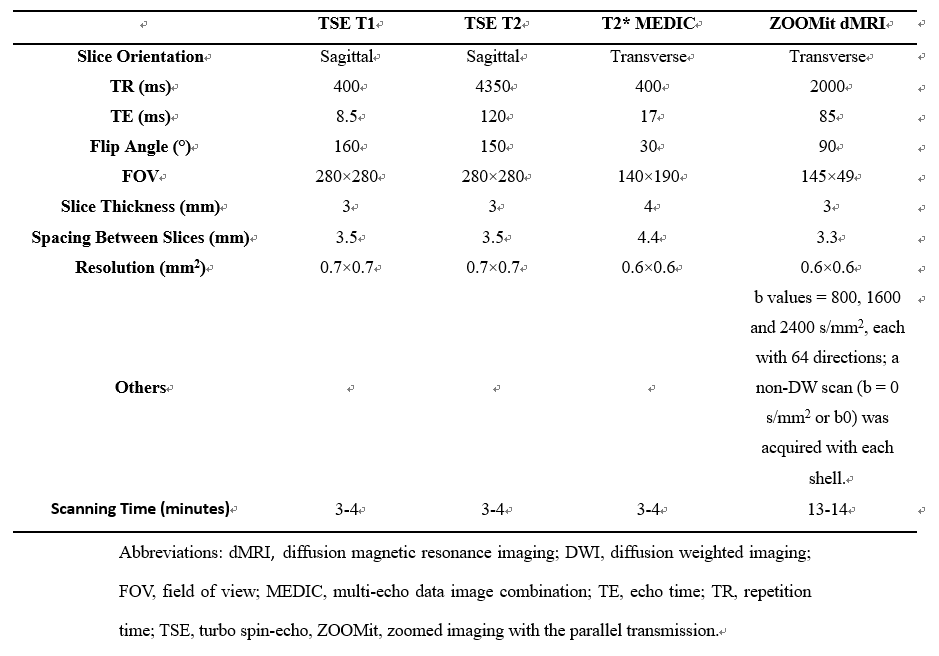
Data acquisitionBetween January 2021 and April 2023, patients with a clinical diagnosis of early CSM (no abnormal signal within the spinal cord) were prospectively enrolled, and paired volunteers (aged within five years) were recruited to undergo MRI examination. The dMRI cervical spinal cord segments of the volunteers were consistent with those of the matched CSM patients. At the same time, all patients were grouped according to age (<50 and ≥50 years). A 3T MRI scanner (MAGNETOM Prisma, Siemens Healthcare, Erlangen, Germany) equipped with a 20-channel head/neck coil was used to scan patients. The protocols for conventional MRI and dMRI are summarized in Table 1.
Data processing
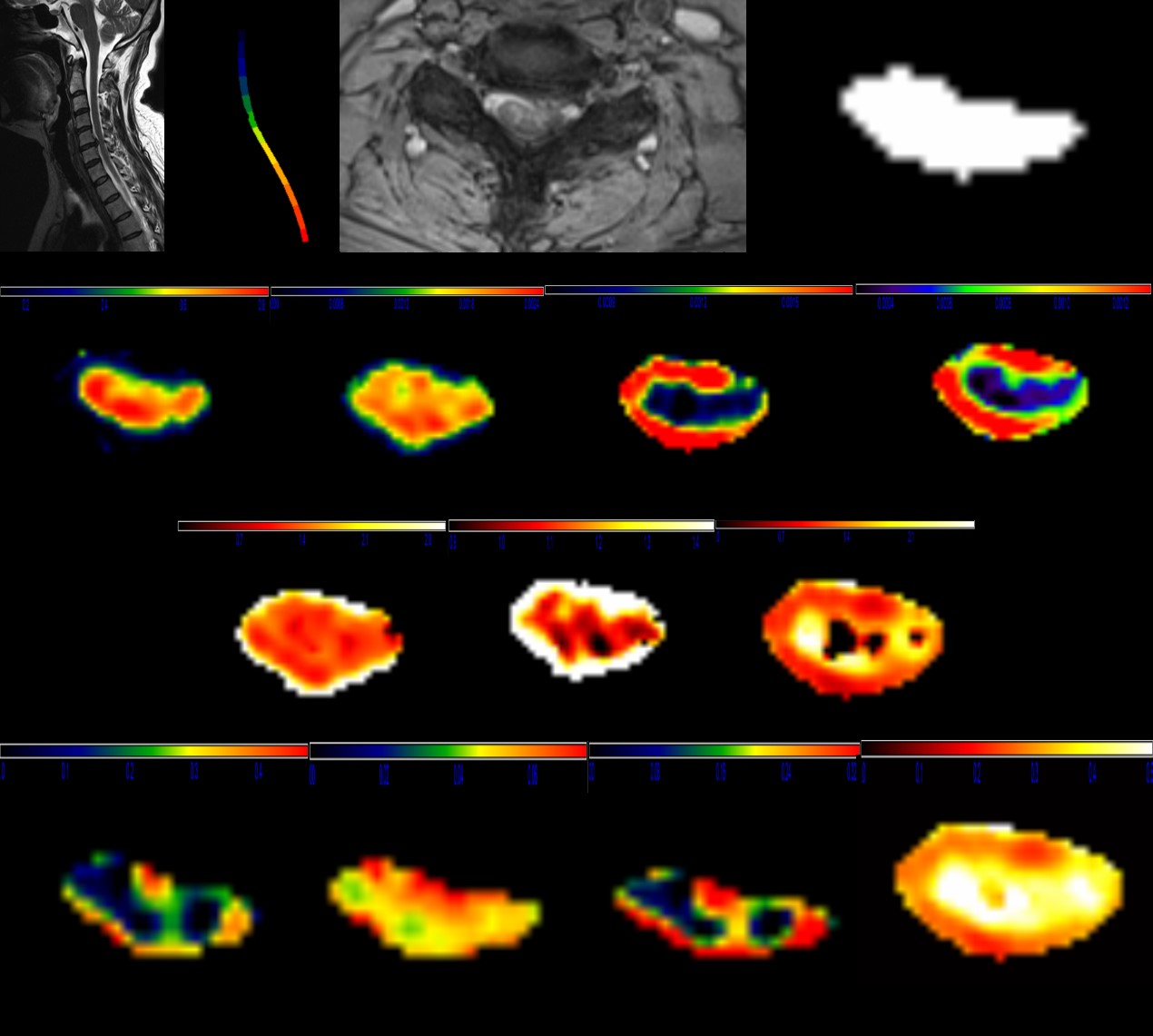
Regions of interest (ROIs) were obtained after automatically identifying spinal cord segments through Spinal Cord ToolBox (SCT, https://github.com/neuropoly/spinalcordtoolbox) software packages. The dMRI parameters included DTI-based fractional anisotropy (FA), mean diffusivity (MD), axial diffusivity (AD), radial diffusivity (RD), DKI-based mean kurtosis (MK), axial kurtosis (AK), radial kurtosis (RK), NODDI-based isotropic volume fraction (ISOVF), orientation division index (ODI), neural density index (NDI), and anisotropic water fraction (AWF). The automatic segmentation results and color maps of different dMRI variables are illustrated in Fig 1. The lesion area and adjacent uncompressed area on all dMRI scans were determined by three radiologists.
Statistical analysis
The variance inflation factor (VIF) was used to evaluate multicollinearity among the dMRI parameters. The filtered dMRI parameters were analyzed using logistic regression to obtain significant parameters that enabled distinguishing volunteers from early CSM patients. When researching CSM patients' adjacent upper and lower uncompressed areas, the difference method was used to eliminate the inherent differences in dMRI parameters of different spinal cord segments. Finally, the univariate t-test was used to verify whether the mean of the difference was equal to zero.
Results
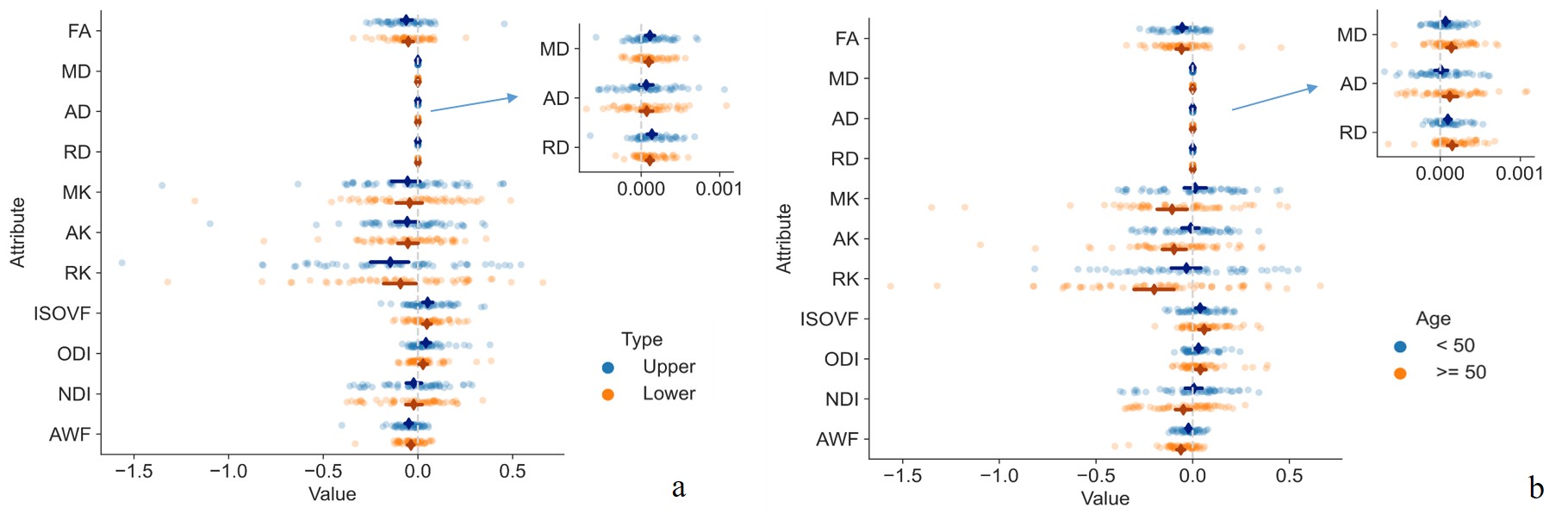
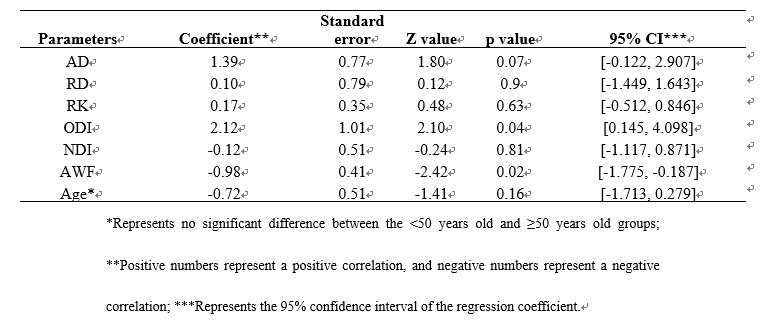
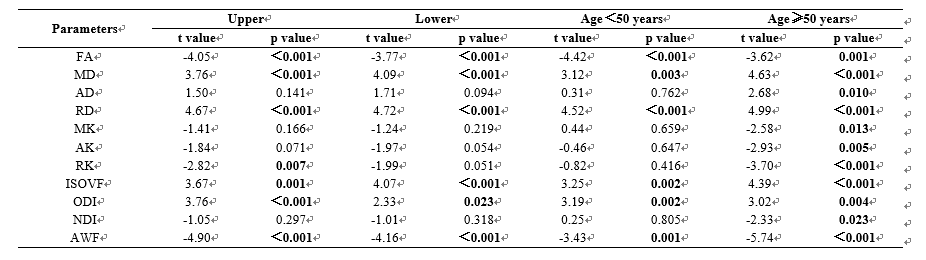
Results A total of 56 early CSM patients and 56 age matched volunteers was included in the study, for a total of 56 paired groups (1:1 matching). The multicollinearity of all dMRI parameters was calculated through the VIF. Finally, AD, RD, RK, ODI, NDI, and AWF were identified as having no significant multicollinearity. By performing logistic regression on the above-screened dMRI parameters, the results showed that the ODI and AWF parameters were significantly correlated with early CSM, with ODI showing a significant positive correlation (r=2.12, p=0.035) and AWF showing a significant negative correlation (r=-0.98, p=0.015). The results of the logistic regression analysis are detailed in Table 2. In the analysis of the adjacent uncompressed spinal cord of early CSM patients, the difference results obtained after subtraction between CSM patients and volunteers are shown in Figure 2. The univariate t-test showed that patients with CSM, FA, MD, RD, RK, ISOVF, ODI, and AWF were significantly different. FA, MD, RD, ISOVF, ODI, and AWF were significantly different in the adjacent lower uncompressed areas. The detailed results of the univariate t-test are shown in Table 3.Discussion and Conclusion
In this work, a case control study matched CSM patients and volunteers 1:1 according to spinal location and age. As the ODI increases, the probability of patients being diagnosed with CSM increases; as AWF decreases, the probability of patients being diagnosed with CSM increases. Combining the ODI and AWF can assist in identifying early CSM. The ODI and AWF can identify early CSM and reflect its microscopic pathology, disease, and developmental changes in the cervical cord of the adjacent upper and lower uncompressed segments, thus assisting clinicians to identify the scope of early CSM.Acknowledgements
National Natural Science Foundation of China (82171927 and 81971578), the Beijing Natural Science Foundation (7212126), and the Beijing New Health Industry Development Foundation (XM2020-02-006).References
[1] McCormick J R, Sama A J, Schiller N C, Butler A J, Donnally C J, 3rd (2020) Cervical Spondylotic Myelopathy: A Guide to Diagnosis and Management [J]. Journal of the American Board of Family Medicine : JABFM, 33(2): 303-13.
[2] Iyer A, Azad T D, Tharin S (2016) Cervical Spondylotic Myelopathy [J]. Clinical spine surgery, 29(10): 408-14.
[3] Behrbalk E, Salame K, Regev G J, Keynan O, Boszczyk B, Lidar Z (2013) Delayed diagnosis of cervical spondylotic myelopathy by primary care physicians [J]. Neurosurgical focus, 35(1): E1.
[4] Talekar K, Poplawski M, Hegde R, Cox M, Flanders A (2016) Imaging of Spinal Cord Injury: Acute Cervical Spinal Cord Injury, Cervical Spondylotic Myelopathy, and Cord Herniation [J]. Seminars in ultrasound, CT, and MR, 37(5): 431-47.
[5] Harrop J S, Naroji S, Maltenfort M, et al. (2010) Cervical myelopathy: a clinical and radiographic evaluation and correlation to cervical spondylotic myelopathy [J]. Spine, 35(6): 620-4.
Figures