2500
Comparison of postmortem in situ 3T MRI and ex vivo ultra-high-resolution 7T MRI in multiple sclerosis cortical lesions1Cleveland Clinic, Cleveland, OH, United States
Synopsis
Keywords: Neuroinflammation, Multiple Sclerosis, Ex vivo; Ultra-high-resolution; Postmortem
Motivation: Cortical lesions in multiple sclerosis are clinically relevant but cannot be detected reliably using conventional MRI. Ex vivo ultra-high-resolution MRI is reliable in cortical lesion detection.
Goal(s): Identify cortical lesions on ex vivo 7T MRI in comparison to postmortem in situ conventional 3T MRI.
Approach: Retrospective visual assessment of cortical lesions on conventional MRI.
Results: 3T T1-weighted MPRAGE showed the highest sensitivity (66%), followed by T2-weighted SPACE (52%), and 3D FLAIR (48%) for detection of cortical lesions. Purely cortical lesions were less visible on in situ MRIs. Some leukocortical lesions appeared juxtacortical white matter lesions on conventional MRI.
Impact: Ultra-high-resolution MRI provides a platform to investigate substrates of cortical pathology in multiple sclerosis by bridging the gap between macroscopic conventional MRI and pathology.
Background
Multiple sclerosis (MS) cortical lesions (CL) are believed to be clinically relevant and extensive but largely undetected on conventional MRI,1 but ex vivo ultra-high-resolution (UHR) MRI has shown excellent agreement with demyelination on histopathology.2 However, no study has compared UHR MRIs to postmortem in situ MRI. We used 7T UHR MRI of an MS hemisphere to identify CL and compared cortical lesion distribution with postmortem in situ MRIs at 3T.Methods
MRI: A postmortem in situ brain MRI of a patient with MS (46y, F, secondary progressive, disease duration 9y) was performed on 3T Siemens Trio TIM for T1-weighted MPRAGE (TE: 2.8ms, TI: 1100ms, TR: 1860ms, FA: 10°, 0.94mm3 , TA 4:20), 3D T2-weighted SPACE (TE: 514, TR: 3200, FA: 120°, 1x1x1.2mm3, TA: 2:40), and 3D SPACE FLAIR (TE: 402, TI: 2000, TR: 6500, FA: 120°, 1x1x1.2mm, TA: 5:10). The interval between the time of death and MRI was 7 hours. Immediately after the MRI, the brain and spinal cord were removed, and the left brain hemisphere was fixed in 4% formaldehyde for 4 weeks according to the published protocol.3 Then, the fixed ex vivo hemisphere was prepared in fomblin using a published protocol4 and scanned on 7T Siemens Terra with a standard knee coil (Siemens Healthineers, Erlangen) with a FLASH sequence (TE: 20.5, TR: 51, FA: 20°, 170µm3, TA: 4:08:00, 12 averages, total scan time 49.6 hours) .Image Processing: MRIs were linearly co-registered using minctracc.5 For registration of in situ and ex vivo MRIs, segmentation of white matter (WM, = normal-appearing WM plus WM hyperintensity), lateral ventricles, and Sylvian fissure were used to assist the registration because the ex vivo brain significantly deformed due to hemispheric division, fixation, and lack of surrounding cerebrospinal fluid. For in situ MRI, a deep learning model with a U-net architecture was used to segment white matter, lateral ventricles, and manually corrected as necessary.6 Then a binary mask of Sylvian fissure was manually segmented. On ex vivo UHR FLASH scan, lateral ventricles and Sylvian fissure were manually segmented on every 10th slice and morphologically closed to fill-in intermediate slices. Similarly, WM was segmented manually on every 10th slice. Then these were used to train another U-net model, and the remaining slices were segmented using the U-net. Then the in situ MPRAGE and ex vivo FLASH images along with masks of WM, lateral ventricles, and Sylvian fissure were co-registered nonlinearly and simultaneously using ANTS with mutual information and mean square difference as cost functions.7
CL Comparison: Regions-of-interest (ROI) were manually selected from 100 CL throughout the brain using ex vivo 7T UHR FLASH. Leukocortical lesions were identified as lesions that involved both cortex and WM, irrespective of subpial or perivascular nature. The outer cortex, layers I-IV, or beyond the line of Baillarger, demonstrated hyperintense appearance and intrinsically low myelin density, which may not associate with MS pathology. Therefore, irregular non-smooth surface or hyperintensity extending to WM border were the criteria for subpial CL. The ROIs were nonlinearly transformed to the space of in situ 3T MRI, and the corresponding areas were visually assessed retrospectively (with labelling of CL from UHR) as lesion is visible, subtle, or not visible. CL were also rated if leukocortical or purely cortical (no WM involvement) on the ex vivo UHR FLASH.
Methods
The patient had high lesion load (74mL of T2- and 31mL of T1-lesion volumes). 87 of 100 ROIs were leukocortical and 13 were purely cortical. The overall sensitivity (visible) for CL at 3T was 66% for MPRAGE, 52% for T2w SPACE, and 48% for FLAIR (Fig 1-4). For purely cortical lesions, only FLAIR showed signs of subtle abnormality (Fig 1). Overall, CLs that occupied more WM area were more visible (Fig 3-4).Conclusion
The ex vivo UHR MRI provided a “reference-standard” for CL on the entire hemispheric brain. Some leukocortical lesions on UHR appeared juxtacortical WM lesions and not touching the cortex on in situ scans. The finding suggests that juxtacortical WM lesions seen on routine MRIs could be affecting the cortex and play more important roles in cortical pathology than previously thought. Purely cortical and mostly cortical leukocortical lesions were far less visible than predominantly WM leukocortical lesions, which indicates more research is needed to visualize purely cortical lesions such as subpial lesions.Acknowledgements
The study was supported by the American Society of Neuroradiology (ASNR2206), NIH NINDS (P01NS38667 and R35NS09730), and National Multiple Sclerosis Society (RG3099).References
1. Geurts JJ, Calabrese M, Fisher E, Rudick RA. Measurement and clinical effect of grey matter pathology in multiple sclerosis. Lancet neurology 2012;11:1082-1092.
2. Schmierer K, Parkes HG, So PW, et al. High field (9.4 Tesla) magnetic resonance imaging of cortical grey matter lesions in multiple sclerosis. Brain : a journal of neurology 2010;133:858-867.
3. Dutta R, Mahajan KR, Nakamura K, et al. Comprehensive Autopsy Program for Individuals with Multiple Sclerosis. Journal of visualized experiments : JoVE 2019:e59511.
4. Kim S, Sakaie K, Blümcke I, Jones S, Lowe MJ. Whole-brain, ultra-high spatial resolution ex vivo MRI with off-the-shelf components. Magnetic Resonance Imaging 2021;76:39-48.
5. Collins DL, Neelin P, Peters TM, Evans AC. Automatic 3D intersubject registration of MR volumetric data in standardized Talairach space. Journal of computer assisted tomography 1994;18:192-205.
6. Ronneberger O, Fischer P, Brox T. U-net: Convolutional networks for biomedical image segmentation. International Conference on Medical image computing and computer-assisted intervention; 2015: Springer: 234-241.
7. Avants BB, Epstein CL, Grossman M, Gee JC. Symmetric diffeomorphic image registration with cross-correlation: evaluating automated labeling of elderly and neurodegenerative brain. Medical image analysis 2008;12:26-41.
Figures
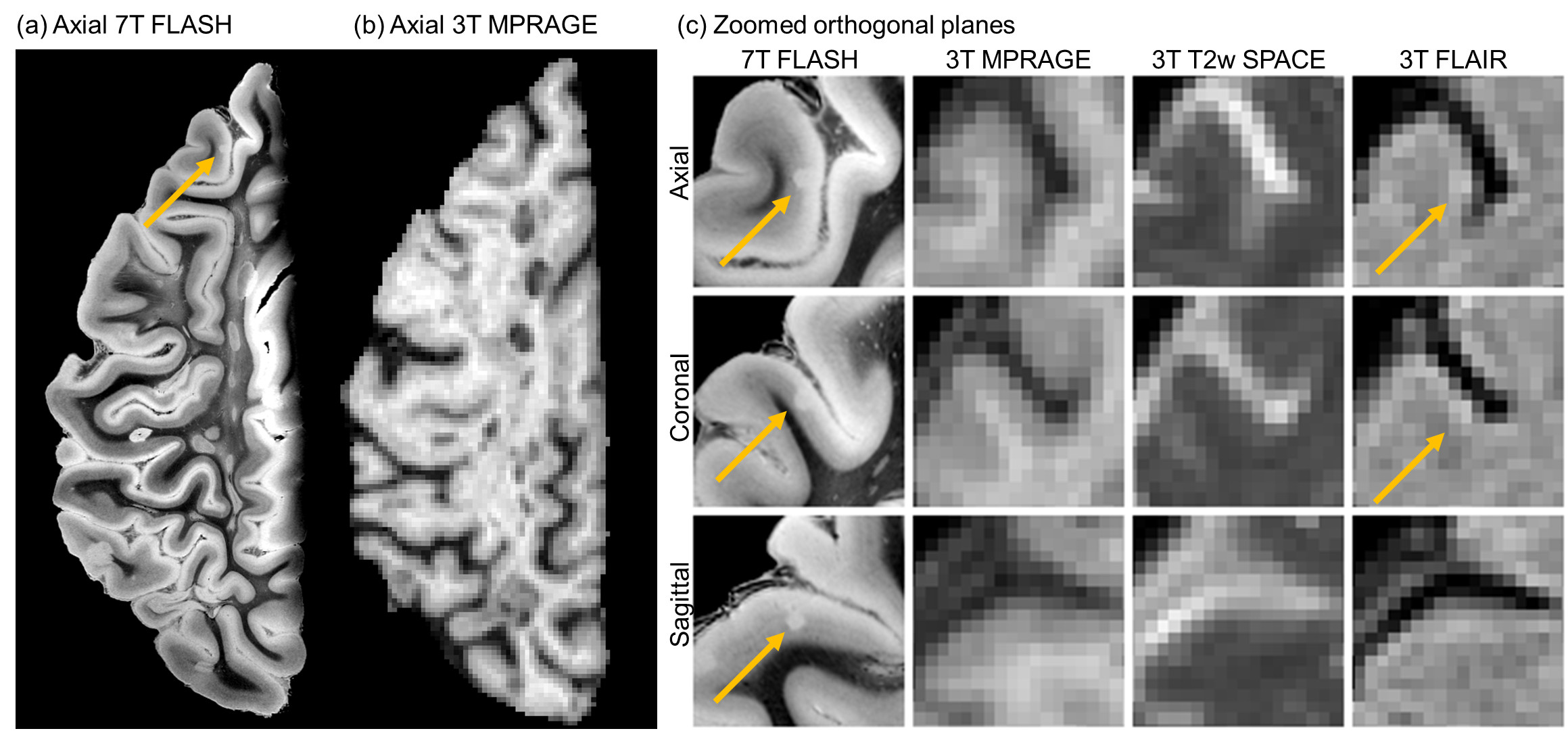
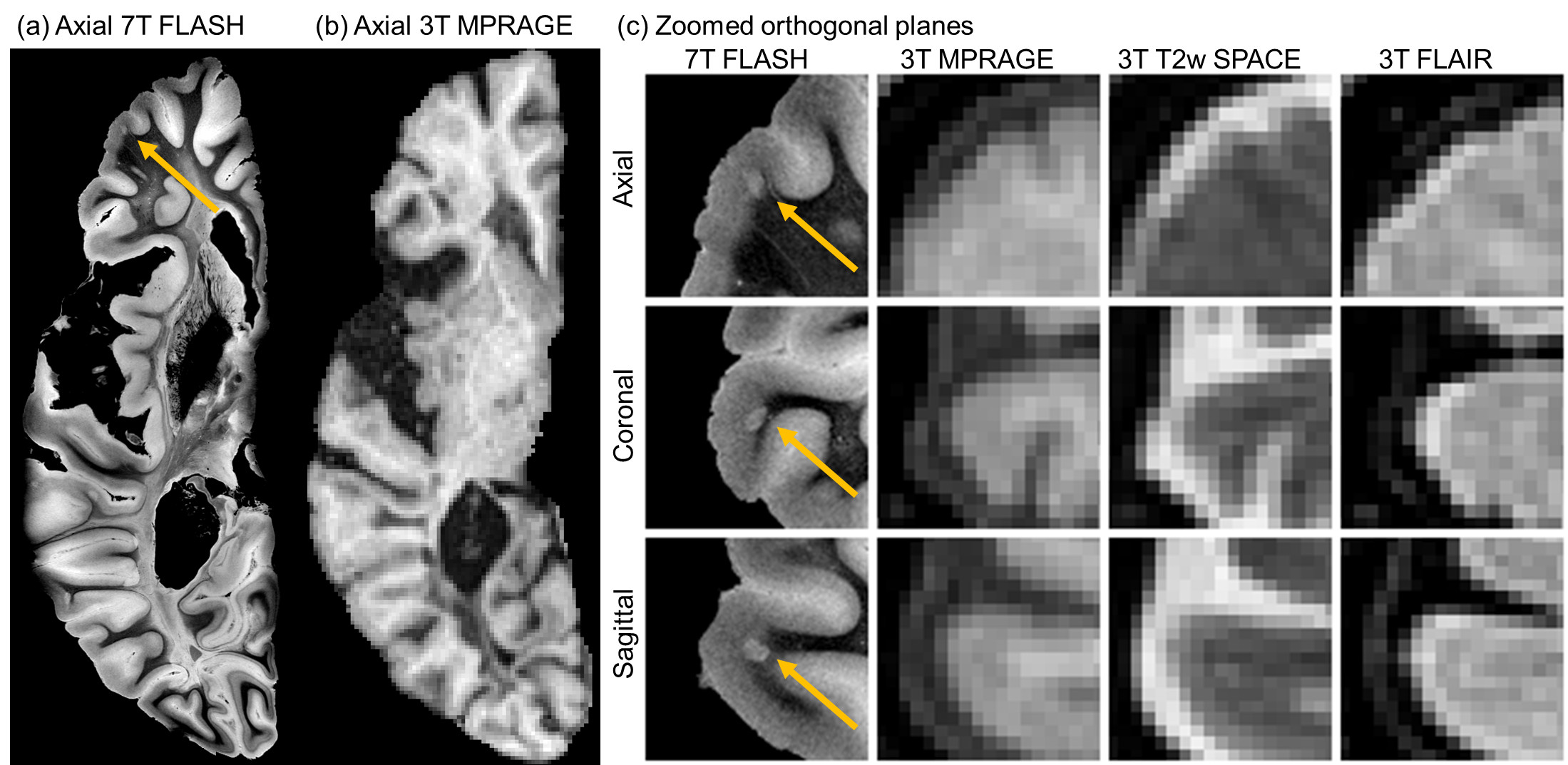
Figure 1: An example of purely cortical lesion that did not involve white matter. Panels (a) shows ultra-high-resolution FLASH and (b) corresponding 3T postmortem in situ conventional MRI, and (c) axial, coronal, and sagittal planes of the same lesion on 7T FLASH, 3T MPRAGE, 3T T2-weighted SPACE, and 3T 3D FLAIR. The lesion was not visible on T1-weighted or T2-weighted images and subtly visible on FLAIR. Note overall amount of lesion load in both white matter and cortex.
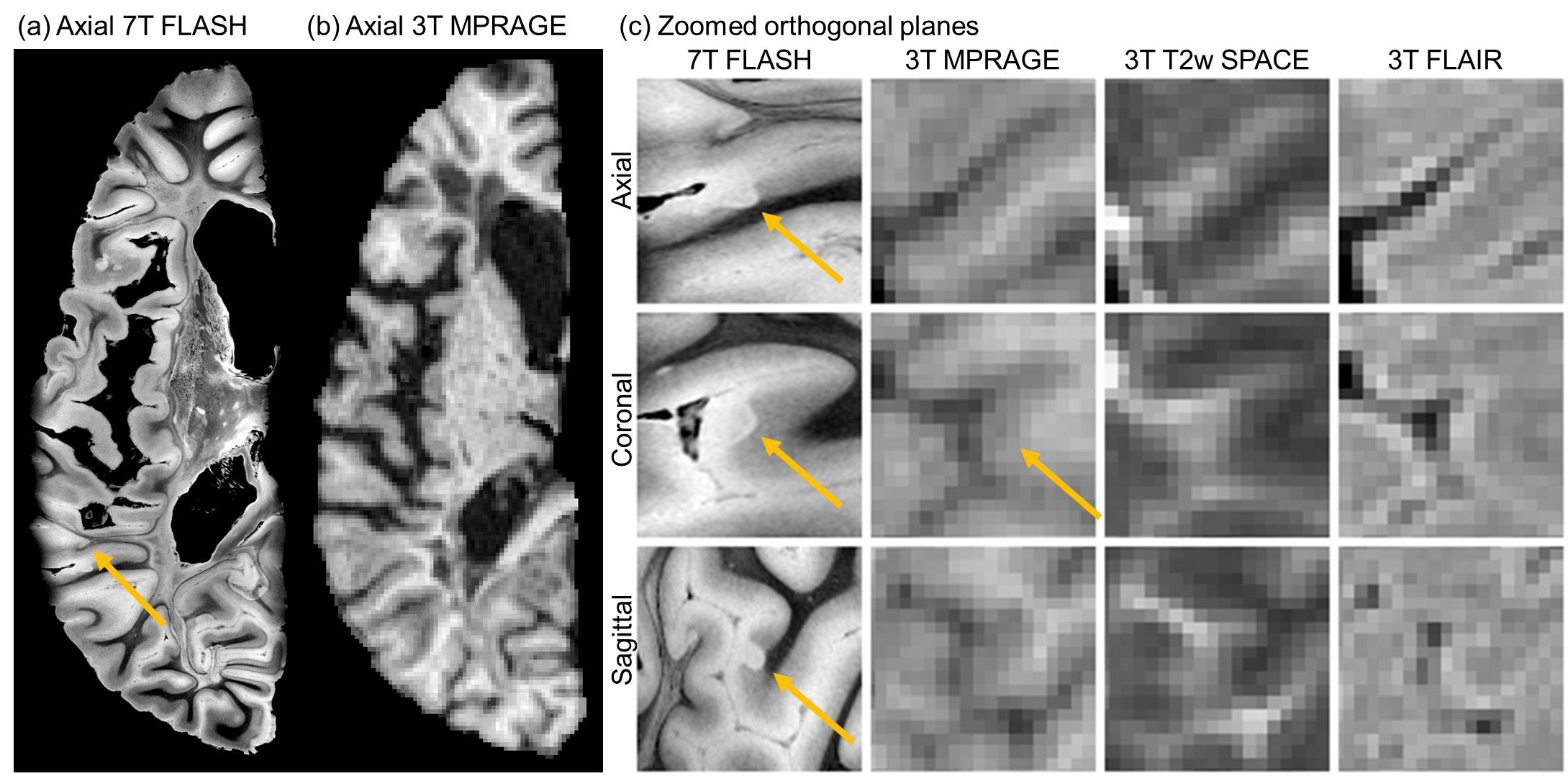
Figure 2: Purely cortical lesion not involving white matter is not visible on all 3 modalities: Panels (a) shows ultra-high-resolution FLASH and (b) corresponding 3T postmortem in situ conventional MRI, and (c) axial, coronal, and sagittal planes of the same lesion on 7T FLASH, 3T MPRAGE, 3T T2-weighted SPACE, and 3T 3D FLAIR. The lesion was not visible on T1-weighted or T2-weighted images and subtly visible on FLAIR. Note overall amount of lesion load in both white matter and cortex.
Figure 3: An example of leukocortical lesion that has small cortical involvement. Black hole and T2 hyperintensity are observed. FLAIR showed a black hole on a portion likely due to the inversion timing. Panels (a) shows ultra-high-resolution FLASH and (b) corresponding 3T postmortem in situ conventional MRI, and (c) axial, coronal, and sagittal planes of the same lesion on 7T FLASH, 3T MPRAGE, 3T T2-weighted SPACE, and 3T 3D FLAIR. The lesion was not visible on T1-weighted or T2-weighted images and subtly visible on FLAIR.