2499
Evaluating Obstructive Sleep Apnea Neuropathophysiology with 1H-MRS and Cerebral Small Vessel Disease Imaging1Neuroscience Research Australia, Sydney, Australia, 2University of New South Wales, Sydney, Australia, 3St Vincent Applied Medical Research Centre, Sydney, Australia, 4Department of Biomedical Sciences, Macquarie University, Sydney, Australia, 5Heidelberg University Hospital, Heidelberg, Germany, 6The George Institute, Sydney, Australia, 7Kirby Institute, Sydney, Australia, 8Prince of Wales Hospital, Sydney, Australia, 9UNSW Ageing Futures Institute, Sydney, Australia
Synopsis
Keywords: Neuroinflammation, Spectroscopy, Obstructive sleep apnoea, cerebral small vessel disease
Motivation: 1H-MRS may be sensitive enough to detect neuropathological mechanisms of cerebral small vessel disease in obstructive sleep apnoea (OSA).
Goal(s): To investigate the relationships between nocturnal blood pressure surges (caused by sleep disturbances) and hypoxic burden (due to recurring apnoeas) on 1H-MRS metabolite levels and cognitive performance.
Approach: Seven controls and 23 participants with OSA underwent brain MRI, sleep physiological assessment and neuropsychological battery.
Results: A higher hypoxic burden was associated with higher cellular energy (Cr/H2O) and acute inflammation (GPC/H20), while more frequent blood pressure surges were associated with higher chronic neuroinflammation (mI/H20). There were no associations with cognitive performance.
Impact: Estimates of 1H-MRS metabolite levels, along with CSVD standard neuroimaging assessment, provide additional information concerning the neuro-cardiovascular and hypoxic burden associated with OSA that could potentially translate into improved early CSVD diagnosis in high-risk populations due to OSA.
Background
Obstructive sleep apnoea (OSA) is a sleep-breathing disorder affecting at least 10-20% of adults1. It is characterised by complete (apnoea) or partial (hypopnoea) upper airway collapses during sleep. It causes chronic intermittent hypoxia (due to recurrent apnoeas) and episodic increases in blood pressure via sympathetic nervous system activation during arousals from sleep2 that might play a critical role in the development of cerebral small vessel disease (CSVD)3. However, this remains to be determined as nocturnal blood pressure surges are difficult to capture with conventional blood pressure monitoring devices and neuroimaging standards for reporting CSVD4 do not capture subtle early brain injury. On the other hand, 1H-MRS, a useful technique for characterisation of metabolite changes in people with OSA5 and vascular cognitive impairment6, might be useful to characterise early neurovascular injury in OSA. Therefore, this study aims to investigate whether the nocturnal blood pressure surge frequency and the measure of hypoxic burden are related to 1H-MRS metabolite levels and measures of cognitive performance in mid-life people with and without OSA.Methods
The study was approved by the South Eastern Sydney Local Health District Human Research Ethics Committee (2019/ETH13574). Thirty participants (18 women, 45–64 years) with well-controlled hypertension (<140/90mmHg), non-alcoholic, non-smoker, non-diabetic and who deny a history of hypercholesterolaemia and neurological disorders underwent an in-lab polysomnography study to quantify during sleep the apnoea hypopnoea index (AHI)7, a measure of OSA, and the frequency of the nocturnal blood pressure surges (>10% systolic ↑BP) using a SOMNOtouch™ NIBP device. The hypoxic burden was calculated as the sum of individual desaturation areas divided by total sleep time8. Seven participants had no OSA (AHI 3.1±1.4 [1.0 – 5.0] events/h), and 23 had untreated OSA from mild to severe (22.9±17.0 [7.3 – 82.1] events/h).Participants also underwent a brain MRI scan (Ingenia 3CX, Philips) using a dStream-32 head coil to determine the CSVD score by counting one point for each neuroimaging signature of CSVD4, if present: white matter hyperintensities (FLAIR), silent brain infarction (DWI), enlarged perivascular spaces (T1, FLAIR) and cerebral microbleed (SWI). In addition, a 1H-MRS was collected from 4×2×1 cm3 VOIs in the frontal white and grey matter to measure total creatine (Cr: a marker of cellular energy), N-acetyl aspartate (NAA: a marker of neuronal density/loss), glycerophosphorylcholine (GPC: a marker of cellular membrane turnover/acute inflammation), glutamate/glutamine (Glu/Gln: an excitatory neurotransmitter and metabolite), myo-Inositol (mI: a marker of chronic neuroinflammation), and lactate (Lac: a marker of pyruvate clearance) in reference to water signal. A-PRESS scans, optimised for lactate measurement9, were acquired with TR/TE = 3000/110 ms, TE1/TE2 = 25/85 ms, 1024 data points using VAPOR water suppression, B1 = 22 μT, using high bandwidth π/2 (FREMEX05) and π (FREMREF04) pulses, 96 averages, scan duration 5 min 6 s. Data were analysed using QUEST (jMRUI, v7) fitting basis sets simulated using NMRSCOPE. Finally, a seven-cognitive domains neuropsychological battery assessed global performance (mean T-score). Cognitive impairment was defined with the Global Deficit Score (GDS≥0.5). Mann-Whitney test was used to determine the difference between groups, and the effect of blood pressure surge frequency was evaluated in a series of regression models on the CSVD and global performance scores.
Results
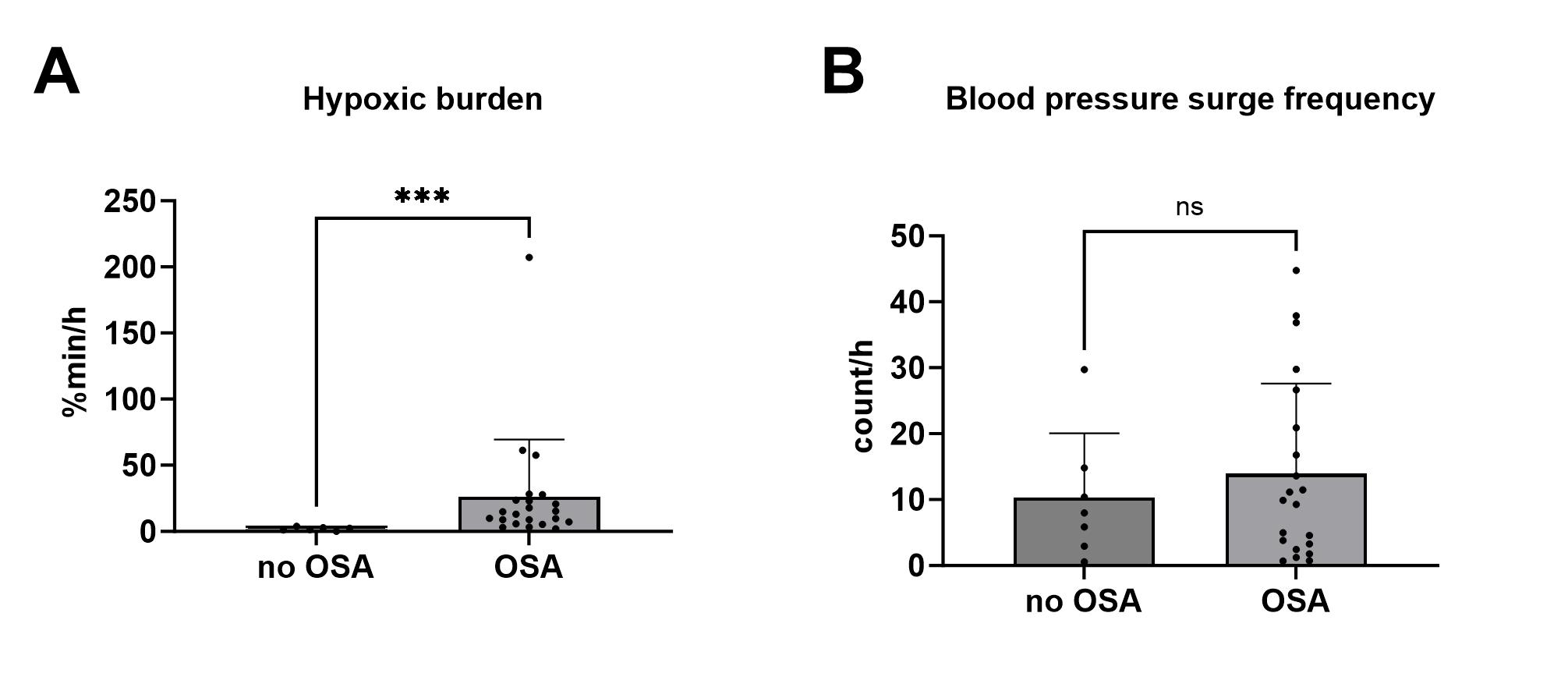
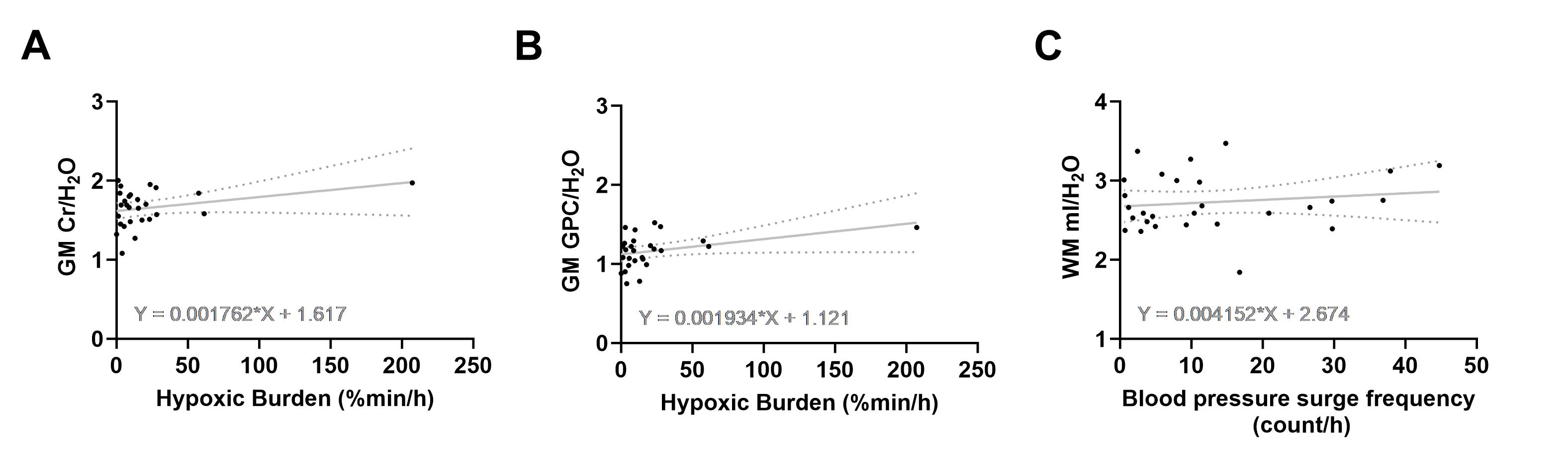
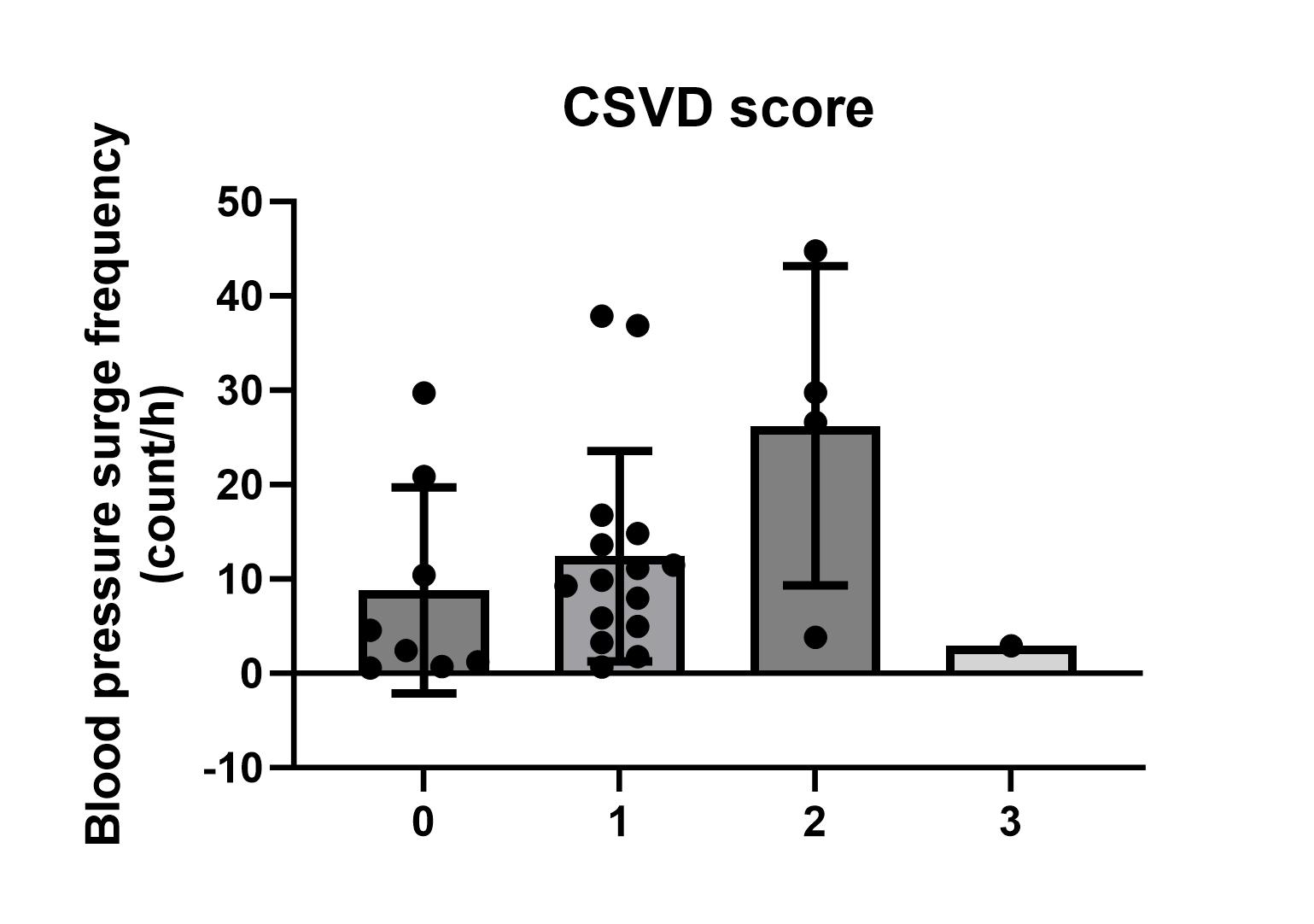
All participants had normal cognitive performance except for two with OSA (GDS=0.58 and 0.53, respectively). Seventy-two percent of the participants had CSVD (CSVD score≥1, 21/29). The hypoxic burden was higher in OSA patients than in controls, but not the blood pressure surge frequency (Figure 1 A and B).After controlling for age, BMI, gender, morning systolic blood pressure, AHI, and blood glucose and cholesterol, a higher hypoxic burden was associated with higher grey matter Cr/H2O and GPC/H2O (Figure 2 A and B). This was also the case when the outlier subject with a higher hypoxic burden was excluded (r=0.544, P=0.036, and r=0.538, P=0.039, respectively). In contrast, more frequent blood pressure surges were associated with higher white matter mI/H2O (r=0.522, P=0.038, Figure 2 C). Blood pressure surge frequency also had an effect on CSVD score (Figure 3) but not hypoxic burden or the interaction of both. For the mean T-score, no significant effects of blood pressure surge frequency or hypoxic burden were found.
Conclusions
Preliminary 1H-MRS results suggest that nocturnal BP surges during sleep contribute to the chronic neuroinflammation process of the white matter, adding to the deleterious effect of the hypoxic burden of OSA in the grey matter. Therefore, estimates of metabolite levels provide additional information concerning the neuro-cardiovascular and hypoxic burden associated with OSA not captured by the standard neuroimaging assessment of CSVD.Acknowledgements
The authors acknowledge the facilities and scientific and technical assistance of the National Imaging Facility, a National Collaborative ResearchInfrastructure Strategy (NCRIS) capability, at Neuroscience Research Australia and the University of New South Wales (UNSW, Australia). This research was supported by funding from the UNSW Ageing Futures Institute, UNSW, Sydney, under an inter-disciplinary fund scheme.References
1. Benjafield AV, Ayas NT, Eastwood PR, et al. Estimation of the global prevalence and burden of obstructive sleep apnoea: a literature-based analysis. Lancet Respir Med. 2019; 7 (8): 687-698.
2. Catcheside PG, Chiong SC, Orr RS, Mercer J, Saunders NA, McEvoy RD. Acute cardiovascular responses to arousal from non-REM sleep during normoxia and hypoxia. Sleep. 2001; 24 (8): 895-902.
3. Durgan DJ, Bryan RM, Jr. Cerebrovascular consequences of obstructive sleep apnea. J Am Heart Assoc. 2012; 1 (4): e000091.
4. Duering M, Biessels GJ, Brodtmann A, et al. Neuroimaging standards for research into small vessel disease-advances since 2013. Lancet Neurol. 2023; 22 (7): 602-618.
5. Xia Y, Fu Y, Xu H, Guan J, Yi H, Yin S. Changes in cerebral metabolites in obstructive sleep apnea: a systemic review and meta-analysis. Sci Rep. 2016; 6: 28712.
6. Meng F, Yang Y, Jin G. Research Progress on MRI for White Matter Hyperintensity of Presumed Vascular Origin and Cognitive Impairment. Front Neurol. 2022; 13: 865920.
7. Berry RB, Brooks R, Gamaldo C, et al. AASM Scoring Manual Updates for 2017 (Version 2.4). J Clin Sleep Med. 2017; 13 (5): 665-666.
8. Sutherland K, Sadr N, Bin YS, et al. Comparative associations of oximetry patterns in Obstructive Sleep Apnea with incident cardiovascular disease. Sleep. 2022; 45 (12).
9. Juge L, Ball I, Rae C. The combined use of MEGA-editing and asymmetric-PRESS methods improves the precision of cerebral lactate detection in healthy adults. In: Proceedings from the International Society for Magnetic Resonance in Medicine; 2022; London, UK.
Figures